 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
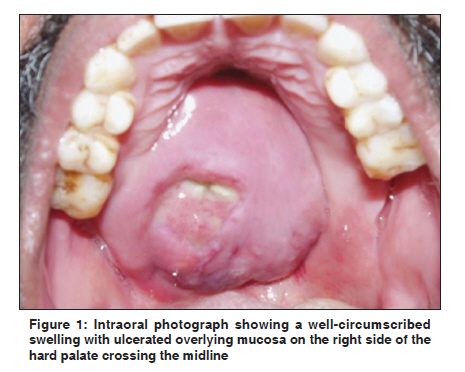
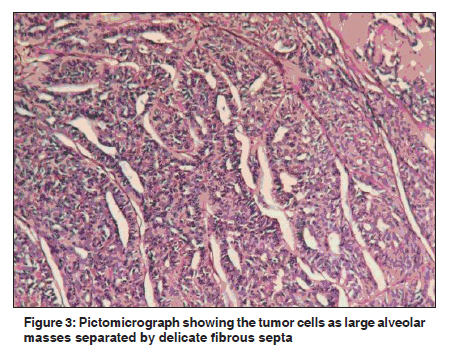
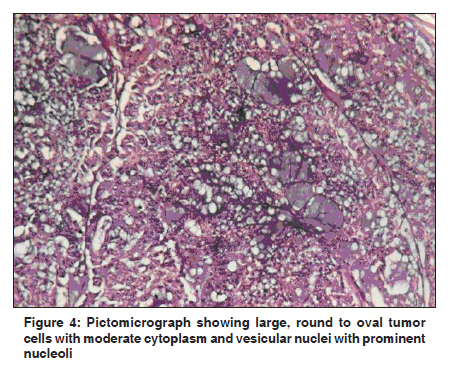
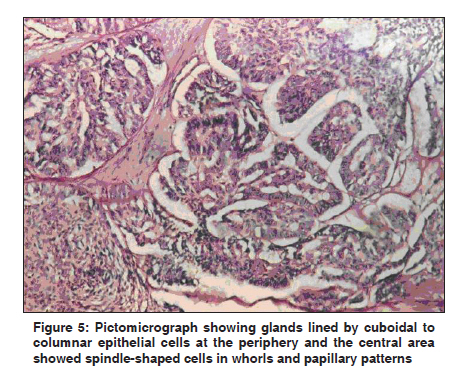
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 518-519 Letter to Editor Polymorphous low-grade adenocarcinoma of the palate: Report of a case S Gupta, CA Kumar, N Raghav Department of Oral Medicine and Radiology, K.D. Dental College, NH-2, Mathura, Uttar Pradesh, India Code Number: cn11139 PMID: 22293274 Sir, Polymorphous low-grade adenocarcinoma (PLGA) is a malignancy arising predominantly from minor salivary glands. PLGAs account for 10% of all tumors of the minor salivary glands and 25% of all malignancies of the minor salivary glands. PLGA was firstly described as a distinct entity in 1983. [1] In 1984, Evans and Batsakis proposed the term "polymorphous low-grade adenocarcinoma". [2] A 52-year-old male patient reported with a complaint of swelling on the palate since 8 years. The swelling was static in size but a sudden increase in the size of swelling was noticed since the last 3 months. The patient gave a history of two to three episodes of bleeding through the right external nares and increased mucus secretion through the left external nares since 3 months and nasal twang in his voice for the past 2 months. A well-circumscribed swelling with an ulceration was present on the right side of the hard palate crossing the midline [Figure - 1]. The swelling was firm in consistency, and was nontender and nonpulsatile. Maxillary cross-sectional radiograph and computed tomography scan revealed an advanced lesion involving the right maxillary antrum, palate and nasal cavity with extensive bony destruction and extension into the surrounding structures [Figure - 2]. Fine needle aspiration cytology revealed large sheets of atypical epithelial cells with scanty cytoplasm and dark-stained nuclei in tight clusters. A wedge biopsy was performed and histopathologic section showed bits of tissue lined by stratified squamous epithelium with subepithelial tumor. The cells are seen as large alveolar masses separated by delicate fibrous septa [Figure - 3]. At places, glands and vague acini were seen. The cells were large, round to oval with moderate cytoplasm and vesicular nuclei with prominent nucleoli and occasional mitosis [Figure - 4]. Many large glands were seen lined by cuboidal to columnar epithelial cells at the periphery, and the central area showed spindle-shaped cells in whorls, papillary pattern suggestive of PLGA [Figure - 5]. A subtotal maxillectomy was performed and the defect was restored with an obturator [Figure - 6]. PLGA is a well-defined neoplasm characterized by architectural diversity, cytological uniformity and indolent clinical behavior. [3] It commonly arises in the palate (49-77.8%), followed by either the buccal mucosa or upper lip (7.4-13.4%), and can also involve the floor of the mouth, lower lip, alveolar ridge and tongue. [4] Because PLGA shares many of the histologic characteristics of pleomorphic adenomas, adenoid cystic carcinomas and low-grade papillary adenocarcinomas, these tumors should be considered in the differential diagnosis of PLGA. [3],[4] The treatment of choice for PLGA is wide local excision with clear margins. Postoperative radiation therapy is reserved for cases of positive or close surgical margins, but it has not been shown to alter outcome in patients without lymph node metastasis. The presence of cervical metastasis is considered an indication for adjuvant radiation therapy. For the treatment of recurrences, radical excision is warranted. [4] PLGA is the second most common minor salivary gland malignancy, characterized by architectural diversity, cytological uniformity and indolent clinical behavior. The understanding of the site, gender, age and prevalence and histological typing aids in proper diagnosis and appropriate management of PLGA. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11139f6.jpg] [cn11139f4.jpg] [cn11139f3.jpg] [cn11139f1.jpg] [cn11139f5.jpg] [cn11139f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}