 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
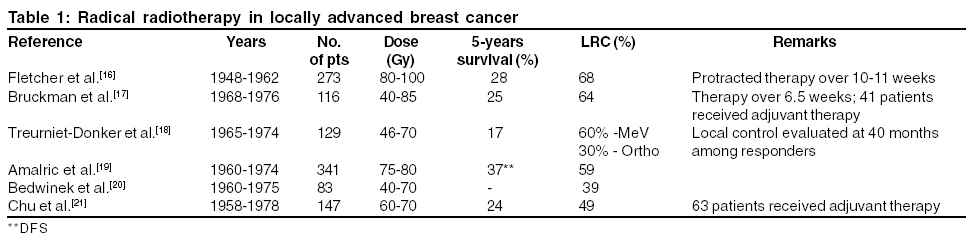
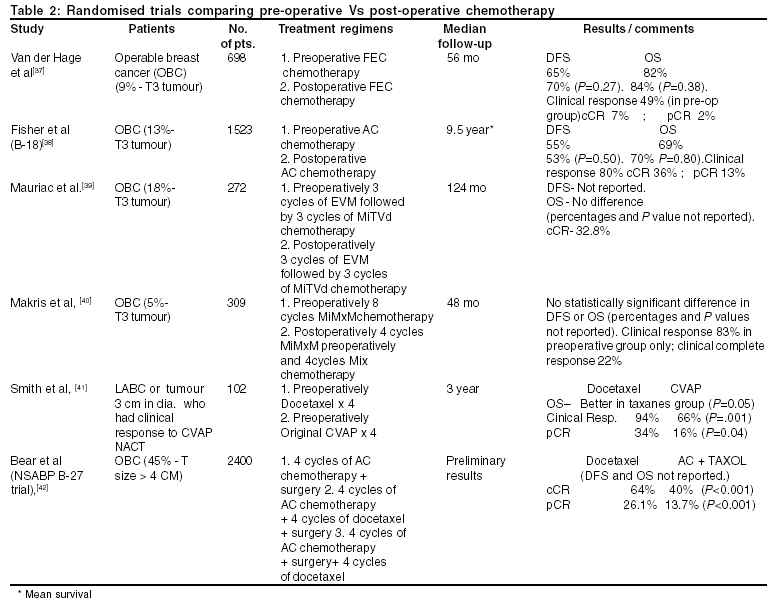
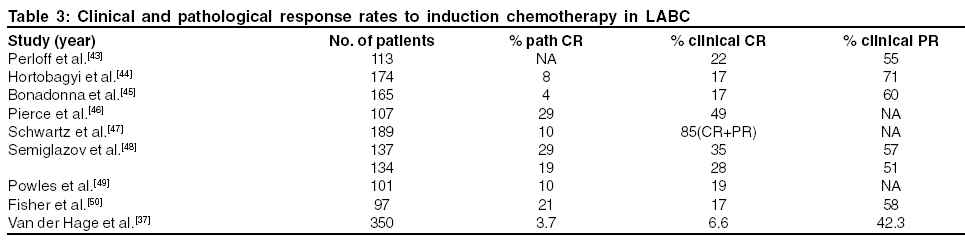
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 21-30 Review Article Management of locally advanced breast cancer: Evolution and current practice Rustogi Ashish, Budrukkar Ashwini, Dinshaw Ketayun, Jalali Rakesh Department of Radiation Oncology, Tata Memorial Hospital, Parel, Mumbai Code Number: cr05006 Abstract Locally advanced breast cancer (LABC) accounts for a sizeable number (30-60%) of breast cancer cases and is a common clinical scenario in developing countries. The treatment of LABC has evolved from single modality treatment, consisting of radical mutilating surgery or higher doses of radiotherapy in inoperable disease to multimodality management, which along with the above two included systemic therapy. Neoadjuvant chemotherapy (NACT) has made a tremendous impact on the management of LABC. NACT was initiated to institute systemic therapy upfront at the earliest in this group of patients with a high risk of micrometastasis burden. While NACT did not yield a survival advantage, it has however made breast conservation possible in selected group of cases. Large number of studies and many randomised trials have been done in women with LABC in order to improve the therapeutic decisions and also the local control and survival. With this background we have reviewed various treatment options in patients with LABC which should possibly help in guiding the clinicians for optimal management of LABC. Breast cancer is the commonest malignant disease among women in the Western world accounting for 1/5 th (18%) of all cancers in women. Every year about one million women and several thousand men are diagnosed with breast cancer worldwide and approximately 60,000 die from it.[1] It is also rapidly emerging as a very common cancer in the developing countries as well. In India, it is the second most common cancer in females with 75,000 new cases occurring every year as per the cancer registries in the country.[2] Surgery Historically, surgery has been the oldest treatment for breast cancer, yet its enthusiasm has waxed and waned over a period of time. Different surgeries have been devised, discarded, rediscovered, changed and abandoned again in seemingly endless fashion as physicians sought to employ the science and technology of their own times. William Halsted at the end of nineteenth century described a surgical technique for removal of the entire breast and en bloc removal of all axillary lymphatics, the chest wall muscles and at times a part of chest wall with the majority of cases being locally advanced in that era. With the success of Halstedian mastectomy, this surgery became a standard in the management of breast cancer. However the long-term results were poor with survival ranging from 13-20% at 5 years.[6] The pioneering work by McWhirter et al. in the mid 20th century showed that less mutilating surgery produced results equal to that of radical mastectomy (RM).[7] The switch from RM to less mutilating surgery came when it was largely recognised that treatment failure from breast cancer was largely due to systemic dissemination prior to surgery.[8] A number of prospective randomised trials comparing RM with modified radical mastectomy (MRM) confirmed the evidence.[9-12] The failure of Halstedian principle of en bloc extirpation of breast and draining lymph nodes to cure many patients of breast cancer, frequent identification of small breast cancer by mammography and success of moderate doses of RT in eliminating sub clinical foci of breast cancer led to the development of MRM. MRM is the term used to describe a variety of surgical procedures, but all involve complete removal of the breast and some of the axillary lymph nodes. Although it may not seem to differ significantly, it seemed to represent a major departure from Halstedian mastectomy. Considering the above evidence, MRM became the standard of care as compared to RM (NIH consensus conference).[13]Radiation Therapy (RT) After the criteria of inoperability by Haagensen and Stout it was suggested that RT could be used alone in radical treatment of breast cancer.[14] Radiation therapists in the early 20th century inherited and applied the concept of radical en bloc ablation.[15] Two major queries arose in this scenario:Could radical radiation be a substitute for radical surgery? Could radiation improve the results of radical surgery? In the initial studies doses administered to the breast were limited by acute skin reactions from the available orthovoltage treatment units. Protracted fractionation with higher doses of upto 60 Gy showed improvement in survival in women with T3, T4 disease (Table 1).[16-21] Higher doses of 80-90 Gy were also attempted which led to higher complications such as cardiac and pulmonary complications, breast oedema, arm oedema, brachial plexus injury, shoulder stiffness, fibrosis and necrosis of chest wall.16],18] The survival of these patients who received radical radiotherapy alone was dismal. Combination of Surgery and Radiation therapy Irradiation, which was initially focussed on inoperable cases, was then considered as an adjunct to radical surgery. Extensive experience using RT alone or in combination with surgery (pre or post Surgery) has been reported from large institutional series.[22] In a large randomised trial, Kaae and Johnson demonstrated the effectiveness of RT in control of subclinical disease.[23] Initial experiences with radical surgery and postoperative radiotherapy showed that significant improvement in local control does occur when surgery is followed by RT but at the same time these trials consistently showed higher cardiac morbidity, the reason for which was the larger volume of heart and lung that was irradiated in order to encompass the internal mammary lymph nodes.24],25] An overview analysis by Cuzick (patients treated in four randomised trials) demonstrated equivalent survival for patients treated with RM Vs simple mastectomy (SM) + RT. But all these trials consistently showed that in the post RT arm the survival advantage due to RT was lost due to high treatment related cardiac mortality.[26] The two biggest trials which showed unequivocal survival advantage with RT in stage II and III breast cancer were by Danish breast cancer group (DBCG) in both premenopausal and post menopausal women. In DBCG 82b 1,708 premenopausal women after MRM were randomly assigned to nine cycles of chemotherapy alone or 8 cycles of CMF chemotherapy and local RT.[27] At a median follow up 114 months, the 10 year locoregional recurrence rate was 32% vs 9% ( P <0.01) and the overall survival 45% vs. 54% ( P <0.01) in the chemotherapy alone and combined chemotherapy and radiation therapy arm respectively. In the DBCG 82c study 1,375 postmenopausal women with stage II and III breast cancer were randomly assigned to tamoxifen for 1 year + locoregional RT.[28] At a median follow up of 123 months, the 10 year locoregional failure improved from 35% vs 8% with the overall survival was 36% vs 45% ( P value <0.05) in the tamoxifen and tamoxifen + RT arms respectively. Another trial that showed the value of postmastectomy is the British Columbia trial, which clearly showed an improvement in overall survival ( P =0.03) and disease free survival ( P =0.009) in favour of RT in high risk women.[29] The cardiac and pulmonary toxicity in these trials decreased to <2% as they included patients who were treated with improved radiotherapeutic techniques and with the use of megavoltage units and more importantly cardiac safe techniques employing computerized planning and use of electron beam for internal mammary chair portals. Therefore with the availability of level I evidence from these well conducted large studies, postoperative RT has now become the standard of care for stage III breast cancer. Although these above trials did include some patients with LABC, no specific randomised trial has addressed this category of disease. The practice of post mastectomy radiotherapy in LABC is based on the data from various large single institutional series.30],31] One such series from M.D. Anderson cancer centre addressing women with non-inflammatory LABC who were treated with mastectomy followed by external beam RT, showed locoregional control rate of 88% for stage IIIA disease and 74% for stage IIIB disease at a median follow up of 17.7 years with doses of 50Gy of external beam RT.[30] As the role of RT was established, trials were done to compare RT alone with surgery followed by post op RT. Perez et al treated 281 patients with LABC reported a locoregional control of 81% at 5 years and 70% at 10 years respectively in the patients treated with mastectomy and RT compared to 42% and 35% at 5 and 10 years respectively for RT alone.[32] It was observed that with higher doses of RT there was significant improvement in the locoregional control. Thus RT has become an integral component in the locoregional management of LABC with improvement in the locoregional control and survival. Radiation therapy to the chest wall and supraclavicular fossa (SCF) to a dose equivalent of 50 Gy has now become the standard even after a good and adequate surgery.Chemotherapy After achieving reasonable local control with a combination of surgery and radiation therapy, the overall survival of LABC still remained dismal with distant metastasis the most common type of treatment failure, appearing in majority of patients within 24 months.[33] Therefore addressing the systemic component of the disease was considered important with an aim to achieve good survival in these women. Adjuvant chemotherapy has over the last 3-4 decades established a firm place in the management of operable and advanced breast cancer. Specifically for LABC management, both adjuvant systemic therapy and neoadjuvant chemotherapy (NACT) were developed simultaneously.In the last three decades, NACT especially has gained a major foothold in the management of LABC. The use of NACT in LABC dates back to 1973, when a regimen containing doxorubicin caused prompt tumour shrinkage and thereby facilitated subsequent radiation therapy or mastectomy.[34] The use of NACT in LABC was based on the rationale that these patients present with a relatively high burden of micrometastasis and therefore makes sense to initiate systemic therapy upfront at the earliest.35],36] Further studies also showed that response to NACT could be considered as a short-term surrogate marker for long-term outcome and therefore act as an in-vivo marker for tumour response to chemotherapy, especially in the primary tumour.[33] There is however a debate in the application of this strategy. While the use of NACT certainly allows an early initiation of systemic treatment, inhibition of post surgical growth spurt, delivery of chemotherapy through intact tumour vasculature, in vivo assessment of response, and downstaging of primary tumour and lymph node metastases to even facilitate less radical locoregional therapy, the local treatment for non responders could become delayed with risk of drug resistance, chemotherapy having to act on a larger tumour burden, inaccurate pathological staging and a possible increase in the risk of surgery and radiotherapy related complications. With the increasing usage of NACT, an interesting spin off was noted. Since a number of patients achieved significant reduction in their tumour and nodal masses, it became apparent that breast conservation therapy (BCT) could be explored even in these patients, a possibility almost unimaginable in the conventional management paradigm. NACT vs Postoperative Chemotherapy Multiple large randomised trials have proven the safety of NACT in LABC (Table 2).[37-42] Most of these trials have shown a good objective response rate of about 60-80% without a detriment in survival as opposed to post-operative chemotherapy. The biggest randomised trial comparing pre-op versus post operative chemotherapy is NSABP B-18 in which 1523 patients with primary operable breast cancer were randomized to preoperative doxorubicin and cyclophosphamide (AC) therapy vs postoperative AC therapy.[38] Tumours with a clinical complete response (cCR) were further categorised as either pathologic complete response (pCR) or invasive cells (pINV). There was no significant difference in the disease free and overall survival in either group. However the frequency of BCT was greater in the NACT arm (67% for NACT Vs 60% post operative chemotherapy, P =0.002). Outcome was better in women whose tumours showed a pCR than in those with a pINV, clinically partial response (cPR), or clinically no response (cNR) (relapse-free survival [RFS] rates, 85.7%, 76.9%, 68.1%, and 63.9%, respectively; P <0.0001), even when baseline prognostic variables were controlled. NACT is therefore considered as effective as postoperative chemotherapy and permits more breast conserving surgeries. In the light of the current evidence it may be concluded that although there is no survival benefit, there is no disadvantage from the use of NACT.Response rates after NACT NACT leads to complete clinical response in 10-30% of patients and a partial response in 50-60% (Table 3).37],43-50] Only a third of patients with a clinical CR have been found to have pathological CR.[36] The best data in this regard comes from the NSABP B18, which showed that out of the 608 patients that received NACT, breast tumour size was reduced in 80% of patients after NACT of which 36% had a cCR[51] (Fisher ER; Cancer. 2002). Tumour size and clinical nodal status were independent predictors of cCR. Twenty-six percent of women with a cCR had a pCR. Clinical nodal response occurred in 89% of node-positive patients: 73% had a cCR and 44% of those had a pCR. There was a 37% increase in the incidence of pathologically negative nodes. Overall, 12% more lumpectomies were performed in the NACT group; in women with tumours >5.1 cm, there was a 17% increase in lumpectomies. Thus approximately 13% of primary breast carcinoma cases exhibited both cCR and pCR. In addition 7% of patients exhibited a pCR in the absence of a cCR. A pCR occurred in 38% of those patients determined to have achieved a cCR. The assessment of clinical response in the axilla has yet not been standardised and is measured by different techniques. Kuerer et al. found that of 55 patients with LABC who appeared to have had complete resolution of axillary disease by both physical examination and ultrasonography, 29 patients (53%) had pathologic evidence of axillary metastasis after NACT.[52] Despite the difficulty in accurately assessing the tumour response it has been shown that patients who achieve a complete clinical or pathological response have better outcome. Kuerer et al in their series of 372 patients with LABC observed pathological CR in 43 (12%) patients and showed better survival outcome in these patients as compared to those who did not have pCR.[53] When pathology specimens in the NSABP-B18 trial were reviewed, patients with the pCR exhibited a better OS and DFS compared with those with a pathologic partial response (presence of sparse invasive tumour [pPR]) or no pathologic response (pNR).[54] Type of chemotherapy Over the years it has been proven in large randomised trials that anthracycline based chemotherapy are the most effective agents in the management of invasive breast cancers. The EBCTG meta- analysis involving 11 randomised trials comparing anthracycline based polychemothrapy and non anthracycline based chemotherapy clearly showed a modest benefit in terms of recurrence rates and overall survival.[55] The results can be further improved if anthracyclines can be combined with other non-cross resistant chemotherapy i.e. taxanes. Taxanes namely docetaxel and paclitaxel given as either single agents or as a combination are emerging to be quite effective in the management of breast cancer. Given the encouraging response rates to taxanes in metastatic breast cancer and the significant disease-free and overall survival benefit shown by the addition of paclitaxel in stage II disease, taxanes are used extensively as non-cross-resistant agents with doxorubicin in stage III breast cancer.[41],42] When docetaxel has been compared head -on with anthracycline based chemotherapy it seems to show a better response rate in selected patients as reported in a small series.[41] The NSABP B-27 trial has shown that use of taxanes with doxorubicin sequentially did show a better response rates in terms of superior partial and complete response both in estrogen receptor positive and negative patients.[42] The final word regarding the routine use of taxanes and the choice of drug has not been conclusively resolved as yet and awaits confirmation from ongoing studies. Number of Neoadjuvant chemotherapy cycles There is a lot of variation in the number of cycles of chemotherapy that are given in neoadjuvant setting in the literature.[44] Investigators have administered either 3-4 cycles of chemotherapy were administered[38],[39],[41] or chemotherapy was continued upto maximal response.[46] This is an important issue, and may have several pitfalls. Current techniques of evaluating response to NACT (physical examination, mammography, and ultrasound) remain imprecise. The significance of small reduction in tumour mass may be difficult to evaluate because of peritumoral oedema and fibrosis. There is fear amongst the clinicians that tumour might actually grow during a protracted treatment of NACT. The biological significance of an early clinical response may be entirely different from that of a late response, a possibility suggested by complete lack of correlation between response and outcome as shown by Pierce et al.[46] As maximal response is always determined retrospectively this may result in delay in surgical planning and thus consequent reduction of chemotherapy dose intensity. The advantages of giving chemotherapy upto maximal response are that if the patient has achieved good clinical response in less than planned cycles, continuation of further chemotherapy consolidates the complete response by maintaining the dose intensity. However it is well known that the complete clinical response does not equate to complete abolition of all disease pathologically.[56] Another advantage of continuing NACT upto maximal response is that it may be possible that a fixed number of cycles may not be enough to achieve the amount of response necessary to do BCT and if chemotherapy is continued there may be still further regression. Most of the retrospective studies have shown that post NACT tumour burden has a direct effect on locoregional control and survival.[57] Even in control of the systemic micrometastasis giving more no. of cycles is beneficial and has an effect on the locoregional disease. This can be based on the Skipper′s theory that the primary tumour and its micrometastasis may respond differently to chemotherapy.[58] Further data can be extrapolated from the studies in metastatic breast cancer. In patients with metastatic breast cancer the median number of cycles to achieve an objective response (mostly partial response) were three, whereas that required to achieve a complete response is five.[59] Neoadjuvant hormonal therapy Efforts to improve response to chemotherapy include attempts to synchronise tumour cells with hormonal agents. Conte and associates used estrogenic recruitment in conjunction with cytotoxic chemotherapy and achieved a 15% clinical complete response rate. The 3-year rate of progression-free survival was 54%.[60] A subsequent randomized trial done by Chua et al. with FAC chemotherapy, with or without diethylstilbestrol, showed higher response and disease-free survival but no overall survival benefit for patients receiving estrogenic recruitment.[61] Others also found higher objective response rates with hormonal manipulation, without improvements in overall survival rates. Pierce and associates[46] and Lippman and colleagues[62] at the NCI also used a strategy for hormonal synchronisation with both estrogens and antiestrogens in their approach to locally advanced disease. Despite complete clinical response rates of 50% with stage IIIA disease and 57% with inflammatory disease, the 5-year survival rates did not significantly differ from survival results in other series that did not use hormonal synchronisation. Adjuvant hormonal therapy Bartelink et al. did the largest randomized trial completed in patients with LABC with adjuvant hormonal therapy. A reanalysis of the same was done after 8 years.[64] Specifically, 410 patients with LABC, including 48 women with inflammatory disease, were randomised to receive radiation therapy alone, radiation therapy with chemotherapy, radiation therapy with hormonal therapy, or radiation therapy with both chemotherapy and hormonal therapy. Patients who were randomized to receive chemotherapy received 12 cycles of CMF. Premenopausal women who were randomized to receive hormonal therapy received ovarian irradiation, whereas postmenopausal women who were randomized to receive hormonal therapy received tamoxifen. With a median follow-up of 8 years, both hormonal therapy and chemotherapy reduced the risk of locoregional failure from approximately 60% to 47%. Hormonal therapy significantly improved survival, with a 25% reduction in the death hazards ratio. Unlike an interim analysis that showed a significant improvement in survival in the chemotherapy arm, this benefit did not remain statistically significant with further follow-up. In the most recent analysis, however, the greatest survival benefit was observed in women who received both hormonal therapy and chemotherapy with radiation, with a 35% reduction in the death hazards risk. Locoregional therapy following NACT Currently the sequencing of different modalities and their choice is a topic of major controversy. Oncologists across the globe have combined these modalities in various sequences and combinations. With more and more number of patients of LABC being treated with NACT a difference in the local therapy offered has been observed amongst various institutions. After NACT, surgery alone, radiotherapy alone or a combination of both has been attempted in the context of multidisciplinary management. Surgery has mainly been in the form of MRM, even though wide excision lumpectomy has been attempted. Multiple randomised trials and non-randomised studies have been conducted to address the issue of choosing the best local therapy either alone or in combination. The Cancer and Leukemia Group B attempted to define the choice of local treatment following NACT in patients with inoperable disease.[43] One hundred and thirteen patients (67% with stage IIIB disease) received 3 months of NACT with CAFVP. Eighty one percent of patients were deemed operable and randomised to either surgery or radiotherapy, followed by an additional 2 cycles of CAFVP. At a median follow up of 37 months, there was no significant difference in either DFS (29.2 vs. 24.4 months) or OAS (39.3 vs 39 months) between the two groups. However, the local recurrence rates were much higher in radiotherapy arm (55%) than surgery (42%). De Lena et al from Milan treated 132 patients with three cycles of NACT (doxorubicin and vincristine) followed by surgery or radiation therapy, than an additional seven cycles of same chemotherapy.[65] Although the group randomised to surgery following initial chemotherapy had better initial local control than those treated with radiation therapy alone (100% vs 60%). The short and the long term outcome in both the groups were essentially same (75%) after completion of the additional cycles of chemotherapy. The results of the study failed to indicate that surgery improved the overall results including local control, over radiotherapy in a combined modality setting. Thus both these trials clearly showed that although initial local control is higher when NACT is followed by surgery there was no difference in ultimate local control and survival. Although no randomised data exists, indirect comparisons between trials that included only one form of regional therapy versus two types of regional treatment, have suggested that when both surgery and radiotherapy are employed, ultimate local control rates are higher than when only surgery or radiotherapy is utilized. However, only one randomized trial that addresses this question has been reported, and no significant differences between the two arms were detected.[66] This trial included 184 patients with LABC that received 2 cycles of NACT with CAFVM, which was followed by mastectomy and after which they were randomised to receive RT vs no RT. This was then followed by 10 additional cycles of chemotherapy. They found that those patients who received radiotherapy had a higher incidence of distant metastasis as compared to those not receiving RT. This was attributed to delayed institution of chemotherapy due to the use of radiotherapy and immunosuppresion caused by mediastinal irradiation. Breast conservation in LABC While MRM still perhaps remains the standard of care for the surgical management of women with LABC, less extensive surgeries (without compromising local control and/or survival) are being increasingly explored with the use of NACT. The down-staging of tumours seen in 60-70% of women not only makes them operable but also, on many occasions can be considered for BCT. Attention has therefore been directed towards the identification of patients with an excellent response to NACT who could possibly be the candidates for BCT. The goals of this approach are to achieve optimal locoregional control with acceptable cosmesis. A lot of interest has been generated in the last 15 yrs, to make BCT feasible in the patients suffering from large operable breast cancer (LOBC) and LABC. Several centres have reported their experience with combined modality therapy of LABC and BCT. However there is a great variability in the methods utilized, as well as the selection criteria for patients to undergo BCT. As in early breast cancer, presence of multicentric disease, extensive micro-calcification, extensive skin changes, and lymphatic permeation are generally considered as contraindications for BCT in these scenarios as well.One of the early attempts in assessing the feasibility of BCT in LABC was the study done at M.D. Anderson Cancer Centre (MDACC) in which mastectomy specimens from 143 patients with stage IIB and III breast cancer (77% stage IIIA or IIIB) were retrospectively analyzed after NACT.[67] Sixteen percent had a CR and 84% a PR response after three cycles of CHOP chemotherapy. Using the criteria for breast preservation in early-stage disease, it was observed that in 23% of these women BCT could be offered after NACT. Based on this experience, BCT started being offered to selected subset of women with LABC at MDACC. Investigators at the NCI and the University of Michigan reported their results with breast conservation using a selection process based on biopsy-proven pathologic criteria.46],68] Investigators at both institutions prospectively administered NACT and performed a biopsy at the primary site, either after maximal clinical response or after a fixed number of cycles. For patients with a pCR, definitive locoregional radiation therapy was delivered. The more conventional mastectomy with postoperative RT was administered to patients with residual disease at biopsy. With a median follow-up of 5.3 years, the 5-year actuarial locoregional failure rate as first site of failure was 23% with BCT in the NCI series. Similarly, with a median follow-up of 4.5 years, the 5-year actuarial estimate of locoregional failure as isolated first failure was 18% in the Michigan series. In a retrospective study at the Jefferson medical college, Schwartz and associates treated 189 women belonging to stage IIB and III with NACT.[47] Eighty five percent had a response to the induction chemotherapy. Of these 103 (64%) were treated by mastectomy while 55 (36%) had BCT. The 5 yr DFS was 56% for the mastectomy group and 77% for those treated with BCT. The 5 year overall survival for mastectomy group was 67% and 80% for the BCT group. Notably 10% of the mastectomy specimens were found to have no evidence of insitu or invasive carcinoma and 7% having only carcinoma in situ and no residual disease. While the best responders were obviously in the BCT group but when the responders were stratified with respect to age there was no difference in survival between mastectomy arm and the BCT arm. This issue of administering the choice of local therapy after NACT is a little controversiual, especially in patients with complete clinical response. An important French study tries to address this issue where Touboul et al. treated 147 patients with tumours more than 3 cm in size with NACT comprising of CVAF for four cycles. Ninety-five patients were eligible to undergo BCT of which 48 patients had a complete response and 47 had a residual disease at the primary.[69] Patients with CR underwent only a radiotherapy boost to the tumour bed, whereas the patients with residual disease underwent a wide excision lumpectomy, received 2 more cycles of AC chemotherapy followed by radiotherapy. The 5 year OAS in the BCT group was 81% in patients that underwent wide excision+RT while it was 65% in the radiotherapy alone group. In contrast the 5 year survival was 76% in the patients who underwent mastectomy. These studies therefore demonstrate the importance of surgical modality in the locoregional management, even if there is complete clinical response after NACT. It is important therefore that the surgeon defines the initial tumour extent before starting NACT. This could be done with tattooing the entire tumour extent, placing radiographic markers and taking X-ray or CT images or putting the biopsy scar in the epicentre of the tumour, a technique adopted at our centre. This also has critical implications for marking out the target volume for radiotherapy boost treatment. Data of locoregional recurrence rates following BCT in LABC is relatively sparse. A study from M.D Anderson cancer centre reported results in 340 women including 130 patients (38%) staged IIIA, IIIB, and IIIC who underwent NACT followed by BCT.[57] The five-year actuarial rates of Ipsilateral breast tumour recurrence (IBTR) - free and locoregional recurrence (LRR) -free survival were 95% and 91%, respectively at a median follow-up period of 60 months. Variables that correlated positively with IBTR and LRR were clinical N2 or N3 disease, pathologic residual tumour larger than 2 cm, a multifocal pattern of residual disease, and lymphovascular space invasion in the specimen. The presence of any one of these factors was associated with 5-year actuarial IBTR-free and LRR-free survival rates of 87% to 91% and 77% to 84%, respectively. The authors showed that BCT after NACT results in acceptably low recurrence rates and even in those patients with stage III and IV disease and advanced nodal stage, residual tumour more than 2 cm, multifocal disease and LVI predict for higher local and locoregional recurrence rates. As in operable breast cancer, radiotherapy is indeed critical in the management of BCT in LABC as well. The technique of irradiation is more or less but emphasis is to be laid on irradiating peripheral glandular areas such as supraclavicular fossa even in patients with complete response to NACT. The issue of internal mammary chain lymphatics is not unequivocally resolved as yet mainly due to relatively high cardiac complications by direct photon irradiation techniques. Irradiation of the internal mammary chain (IMC) of lymph nodes especially in LABC is highly controversial issue. While it seems logical that patients with LABC (skin involvement, heavy axillary nodal burden, etc.) would harbour a high micrometastatic burden in IMC warranting irradiation in these sites, the issue is likely to be crystallised with the availability of results from the recently concluded EORTC randomised trial.[71] If the results indeed favour irradiating IMC area, this will have to be done with individualised computer planning and the use of electrons in the treatment delivery (to limit cardiac dose), an issue which will have huge implications in countries with limited resources. In this regard, we are at the moment conducting a study examining a novel way of IMC irradiation with iridium 192 brachytherapy, a modality much more commonly used and therefore potentially appealing in our set up.[72] Boost irradiation in operable cancer is well established, especially in younger women. In LABC however, there is a relative paucity of data, especially as to the choice of target volume for boost. At some institutions the boost is given taking into consideration the pre-chemotherapy size while at some centres, volume is determined by the post chemotherapy clinical/mammography size.[70] The situation gets complicated when there is complete response of the tumour following NACT. Due to the frequently large tumour sizes seen upfront, the boost portals are sometimes larger and may encompass large volume of the breast tissue. Although the issue of taking pre or post chemotherapy volumes for boost targeting is unresolved, a majority of the institutions including ours take pre-treatment volume for boost portals. The effect of such larger volumes on cosmetic outcome needs to be evaluated. While there is reasonable data to suggest that BCT even in patients with locally advanced breast cancer is feasible in a selected group of patients after downstaging with neoadjuvant therapy without compromising local control, survival and cosmesis, ultimate validation of will obviously come from generating level 1 evidence. This very important question is being addressed by the EORTC randomised trial which compares the overall survival and time to loco-regional failure in women with LABC treated with BCT vs mastectomy followed by RT after they have received prior NACT.[71] With a target accrual of 1200 patients, which was completed in December 2003, the results of this study are most awaited and will hopefully resolve the issue of local surgical therapy in the management of LABC. Conclusion Multidisciplinary therapy has now become the standard for women with LABC. Surgery has evolved from the era of RM to MRM to present era where BCT is being attempted. MRM still remains the standard of care in the surgical management of LABC in many parts of the world. The role of BCT in LABC is establishing slowly and the recently concluded EORTC randomized trial will hopefully resolve this issue. Chemotherapy plays an important role in the treatment of LABC, which could be delivered as NACT or postoperative chemotherapy. NACT has an advantage of downsizing of the tumour and making a select group of patients suitable for conservative surgeries with comparable survival outcome. Radiation therapy to the breast and supraclavicular fossa in women with BCT and chest and supraclavicular fossa in women with MRM to a dose equivalent of 50 Gy remains the standard. Therefore NACT followed by locoregional therapy which includes surgery (either MRM or BCT) and radiotherapy followed by postoperative systemic chemotherapy is now an accepted strategy. Inspite of generally improved outcome, the long term cure rates of these tumours are still less than 50% and new strategies in the form of greater understanding and application of molecular characteristics along with novel drugs should further improve the results.References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05006t3.jpg] [cr05006t2.jpg] [cr05006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}