 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
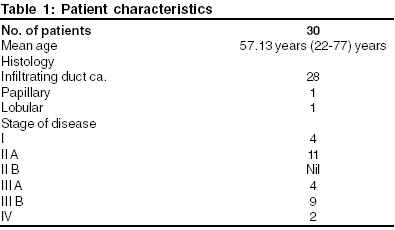
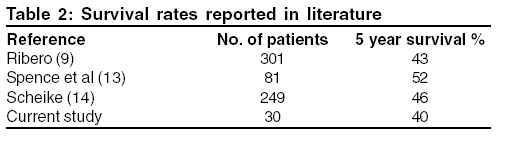
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 31-33 Original Article Breast cancer in males: A PGIMER experience Rai Bhavana, Ghoshal Sushmita, Sharma Suresh C. Department of Radiotherapy, Post Grade Institute of Medical Education and Research, Chandigarh Code Number: cr05007 Abstract Aim: Male breast cancer is a rare disease representing 1% of all breast cancers and less than 1% of all cancers in men. Because of its rarity, carcinoma breast has not been studied extensively and this prompted us to carry out this retrospective study. The aim of the study was to observe the clinical and pathological features, evaluate the prognostic factors and to co-relate the outcome in patients of male breast cancer. Keywords: Loco regional Radiation, Temoxifin Adjuvant Chemotherapy Introduction Breast cancer in males accounts for less than 1% of that in women. Unlike in women, breast cancer in males affects predominantly older population with a peak incidence at 60 years of age and the histology is usually ductal carcinoma. The various potential risk factors that have been attributed are family history of first-degree relatives, single marital status, previous benign disease of the breast and history of previous chest wall irradiation. The contributions of several other variables like smoking, alcohol consumption, obesity, hormonal therapy, Klienfelters syndrome and exposure to electromagnetic radiation remains uncertain.[1] MATERIALS AND METHODS A total of 1526 patients with cancer breast were treated at the department of radiotherapy at PGIMER, Chandigarh from years 1996-2000. The total number of male patients with cancer breast was only 30. Thus, male breast cancer accounted for only 0.5% of the total patients with breast cancer presenting to us. The age of patients ranged from 22-75 years with a median age of 56.13 years. Infiltrating duct carcinoma was the most common histology (28/30). One patient had papillary carcinoma. Lobular carcinoma though thought to be rare, was present in one patient. Staging of the tumor was done according to the UICC (TNM Classification 1992) and the distribution according to stage is given in Table 1. Majority of patients i.e. 43.3% presented with stage III disease. Two out of 30 patients had distant metastasis at presentation. Twenty-five patients underwent total mastectomy with axillary clearance. Lumpectomy was done in 3 out of 30 patients. Axillary lymph node metastasis was present in 18 of 30 patients. Metastasis in more than 4 axillary lymph nodes were present in 11 patients and in less than 4 axillary lymph nodes were present in 7 patients.Seventeen patients received radiotherapy as an adjuvant treatment. External radiotherapy was delivered to a dose of 35 Gy in 15 fractions over three weeks to the chest wall by two tangential fields and 40Gy in 15 fractions over three weeks was delivered to the axilla and supraclavicular fields. Seventeen of 30 patients received adjuvant hormone therapy with tamoxifen 20mg given once a day for five years. Six of 30 patients underwent orchiectomy. Six of 30 patients received chemotherapy with CMF (4/30) and FAC regimen (2/30). Follow up of patients ranged from 2-83 months. RESULTS The actuarial five year disease free survival was 40%Loco-regional Loco-regional recurrence occurred in 10% i.e. 3 of 30 patients. One patient who did not previously receive radiotherapy recurred. Two of three patients who recurred locally had more than 4 axillary lymph nodes positive for metastasis at presentation All the recurrences occurred in patients with locally advanced disease at presentation. Distant Metastasis Distant metastasis occurred in 9 patients out of whom 6 patients (66.6%) had T3-T4 tumor and 1 patient had T1-T2 tumor. Seven of 11 patients (63.3%) with more than 4 axillary lymph node positive as compared to 2 out of 7 (28.5%) with less than 4 axillary lymph nodes positive developed distant metastasis. Sites of distant metastasis included bone-4, lung-3, brain-2, liver-2. DISCUSSION Male breast cancer is rare accounting for less than 1% of mammary neoplasia in females. The natural history of the disease closely parallels to that of females. The cause of carcinoma of the breast is no better understood in men than in women. The causative factors that have been implicated in the development of male breast cancer include hyper-estrogenic state, Klienfelter′s syndrome, gynaecomastia, trauma and radiation injury.[1] None of the patients in our study had Klienfelter′s syndrome, sterility or history of exposure to ionization radiation. The median age at which male breast cancer presents is several years later than in women. The median age at diagnosis was 59.13 years and the age of patients ranged from 45-82 years. The median age reported by Circhlow was 59.6 years, which is similar to that reported in our series.[3] In our series, we confirmed the large prevalence of infiltrating duct carcinoma but one patient (3.33%) had papillary carcinoma and 1 patient (3.33%) had lobular carcinoma. Borgen et al have reported a similar histological pattern with lobular carcinoma being extremely rare.[4] It has been observed that male breast cancer typically presents with an advanced stage of disease than do women. It has been suggested that because breast tumors in men are usually superficial and centrally located, these tumors have a ready access to dermal lymphatics, pectoral fascia and sub areolar lymphatic channels thus explaining the advanced disease at presentation.[5] Similar observation was made in our study too, which showed a preponderance of stage III disease (43.33%). 30% patients (9 of 30) had stage III b disease and 13.3% (4 of 30) had stage III a disease at presentation. Rate of axillary lymph node metastasis in our series was 64.2% (18 of 30). Eleven patients i.e. 36.6% had more than 4 axillary lymph nodes positive for metastasis and seven patients i.e. 23.3% patients had less than 4 lymph nodes positive for metastasis. The risk of axillary lymph node metastasis co-related to the clinical tumor size, as reported by other studies too.[6] There has been a transition in the standard approach to surgery for male breast cancer over the years. Modified radical mastectomy has supplemented radical mastectomy and radical mastectomy has been reserved as an option for patients where lesion invades the pectoralis major muscle or involves Rotter′s nodes (interpectoral nodes). The use of lumpectomy is usually limited as the paucity of breast tissue in men often renders adequate tumor excision by lumpectomy impossible.[7] In our study, out of 28 patients who underwent surgery, total mastectomy with axillary clearance was done in 25 patients and lumpectomy in only 3 patients. Post operative radiation therapy is recommended for female patients with lesion larger than 5 cm, any skin, fascia or muscle involvement, poorly differentiated tumors, positive or close tumor margins, lymphatic permeation, matted lymph nodes. Post -operative radiation therapy has been found to reduce the loco-regional recurrence and improve the disease free survival.[8] In our study also, chest wall irradiation seemed to reduce the rate of local recurrence, however, its impact on survival could not be evaluated. The frequency of dermal and muscle involvement and high rate of axillary lymph node involvement justifies the need for chest wall radiation in male patients with breast cancer. In contrast to females with breast cancer, a high proportion of men with carcinoma of the breast have tissue positive for ER and PR (76.4%).[9] Thus, endocrine therapy plays an important role in the management of male breast cancer. Orchiectomy as an initial ablative procedure yields objective response rates varying from 31-68%. Tamoxifen has been seen to be effective in patients without orchiectomy, and following both orchiectomy and adrenalectectomy.[10] Tamoxifen, due to its low incidence of side effects, reluctance of men to undergo orchiectomy and a tumor response of up to 80% remains an ideal treatment. In our study, 17 of 30 patients received tamoxifen and six patients underwent orchiectomy. Though experience of adjuvant therapy for males with breast cancer is very limited, two studies have reported the benefits of adjuvant chemotherapy in men11][,[12] however, as the median age of patients presenting with male breast cancer is high and with frequently associated chronic diseases, tamoxifen as an adjuvant treatment may be a favorable option. Adjuvant chemotherapy may be used with extensive axillary nodal involvement and or negative hormone receptor status. In our study, the actuarial five- year disease free survival was 40%. In literature, five year survival has ranged from 43-74%. (Table 2) The prognostic factors considered in literature are tumor size, histological grade and axillary lymph node status. Axillary lymph node status remains the best prognostic factor. The relatively low disease free survival rate in our study may be attributed to the high incidence of axillary lymph node involvement and an advanced disease at presentation. In conclusion, due to the rarity of the disease, much knowledge remains to be gained about male breast cancer due to the rarity of the disease, which limits feasibility of large randomized clinical trials. Modified radical mastectomy followed by external radiation therapy is the optimal treatment. As an adjuvant treatment, anti- estrogen therapy seems to be the first line approach in a majority of patients and chemotherapy is reserved for patients with poor prognostic factors. References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05007t1.jpg] [cr05007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}