
|
Journal of Cancer Research and Therapeutics
Medknow Publications on behalf of the Association of Radiation Oncologists of India (AROI)
ISSN: 0973-1482 EISSN: 1998-4138
Vol. 1, Num. 1, 2005, pp. 34-37
|
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 34-37
Original Article
Three dimensional conformal radiation therapy in prostate adenocarcinoma: Survival and rectal toxicity
Kannan V., Sathiyanarayanan V.K., Sagde S., Anand
Vivek, Almel Sachin, Kapadia Asha, Srinivas V.
P. D. Hinduja National Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim, Mumbai
Correspondence Address:Radiation Oncology, P. D. Hinduja National
Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim, Mumbai
- 400 016. E-mail: drkannaniyengar@yahoo.com
Code Number: cr05008
Abstract
Technological advances in radiation beam planning and linear accelerator based radiation delivery have led to the development of three dimensional conformal radiation therapy (3D-CRT). The 3D-CRT clinical treatment in our hospital was started in September 1998 and till December 2002, 51 patients with M0 stage prostate carcinoma were treated. Treatment method consisted of pelvis and leg immobilization, planning CT scan, marking of planning target volume and organs at risk and 3D beam plan using multileaf collimated beam shaping through beam's eye view display. Network controlled 3D conformal radiation therapy was delivered with portal image verification. The median 3D-CRT dose was 72 Gy. Of the 51 patients, 35 were followed-up till December 2002 (minimum follow-up 2 years) in whom 32 were disease free and 3 had progressive disease. Eleven patients died, 8 of progressive disease, one due to second malignancy and two of intercurrent illness. Five patients were lost for follow up during 0 - 29 months period, after 3D-CRT. The acute rectal reaction (RTOG criteria) in 51 patients was grade 0 in 4, grade I in 31 and grade II in 16. None had greater than grade II rectal toxicity. The late rectal toxicity in 49 patients who had a minimum 6 months follow-up was grade 0 in 41, grade I in 3 and grade II in 5. Our experience suggests that a dose of 72 Gy by 3D-CRT can be safely delivered to the prostate and gastrointestinal tolerance during treatment and follow-up period was excellent.
Keywords: Conformal Radiation, Prostate cancer, Doses collection
Introduction
Response of tumor clonogen to radiotherapy depends on tumor radiation sensitivity, total radiation dose delivered and adequate coverage of the target. Increase in total dose increases the local control.[1] However, there are restrictions in higher dose delivery with conventional two dimensional (2D) radiation planning and delivery system as there is concomitant increase in normal tissue dose leading to enhanced acute and late toxicity.
Progress in computer technology has favoured the development of precision fractionated radiation delivery system, the three dimensional conformal radiation therapy (3D-CRT). This uses the advances in imaging, high speed computer workstations, computer assisted radiation beam planning and automated multileaf collimated linear accelerator machine. These technological advances have enabled the conformation of the radiation dose to the tumor - target volume. The 3D-CRT technique targets the prescribed radiation dose to the tumor, contouring the spatial distribution of the dose to the precise 3D configuration of the tumor. A special feature of 3D planning is the ability to calculate the dose at each point in the entire 3D space of the irradiated tissues using computer algorithms. Improved precision decreases the risk of anatomical misses and tumor under dosage. The beam′s eye-view display in the 3D planning assists beam orientation and collimation for protection of normal tissue. This permits dose-escalation to the tumor without higher doses to the normal tissue.
The dose-response observation in prostate cancer radiotherapy by the Patterns
of Care Study suggested improvement in local control with a dose of >70
Gy in stage C tumor.[2] However
there was an increase in normal tissue toxicity. 3D-CRT has changed the
scenario. 3D-CRT studies have shown that doses > 70 Gy can be
delivered to achieve better local control in prostate tumor with no increase
of acute or late toxicity.[3],4][
The first 3D-CRT system in India was installed in our hospital and clinical services were started in September 1998. We present our initial experience of 3D-CRT in the treatment of prostate cancer.
MATERIALS AND METHODS Over the period from September 1998 to December 2002, 54 prostate tumor patients were treated with 3D-CRT which included 51 patients with M0 stage prostate adenocarcinoma. This paper reports the survival and toxicity in this group of 51 patients.
All patients had complete clinical evaluation and laboratory studies including complete blood count, renal and liver function tests and PSA estimation. CT scan of abdomen and pelvis, chest radiography and bone scan formed part of staging procedure.
The 3D-CRT equipment in our hospital consists of dual energy digital linear accelerator (Clinac 2300 C/D, Varian Oncology System) incorporating asymmetric X and Y collimators, 80 leaf multileaf collimator (MLC), electronic portal image device (EPID) and Micro MLC, Simulator-CT, 3D beam planning computer workstation (Cadplan Plus) and networking (Varis network).
The technique of 3D-CRT is as follows : Patients were immobilized (pelvis and leg) in thermoplastic mask system or vacuum lock fixation device in supine position. All underwent treatment planning intravenous contrast enhanced CT scans with 3 mm axial contiguous cuts which extended from midpoint of sacroiliac joint to below lesser trochanter of femur. In the 3D planning system the scans were imported through network. Gross tumor volume (GTV) and organs at risk (OAR) were contoured. The GTV included the prostate and seminal vesicles. The lower pelvic nodal areas were included in GTV for planning till December 2000, after which they were contoured only if pre treatment CT / MRI scans revealed involvement of the pelvic nodal area. The OAR included urinary bladder and rectum. The planning target volume (PTV) was contoured by automated or manual expansion of the GTV with a margin of 1-1.5 cm in X, Y and Z axis except at prostate-rectal wall interface where a margin of 0.6 - 1 cm was used. The dose planned to prostate was 70-76 Gy. The seminal vesicles were planned to receive 50.4-60 Gy and the lower pelvic nodal region till December 2000 received a prophylactic dose of 45 Gy.
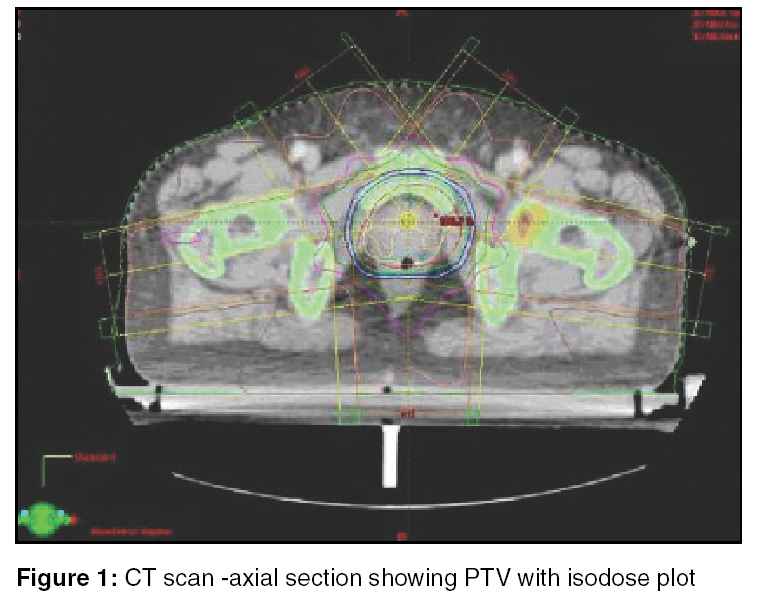
All beam arrangements were visualized using beam′s eye view (BEV) display. MLC beam shaping was used to create beam apertures. Asymmetric collimation and wedges were used when necessary. X-ray beam energy used was 15 MV. All were coplanar beams. Four field (AP, PA and two lateral) conformal technique was used when lower pelvic nodes were part of treatment volume. Five or six field conformal planning was done when PTV included only prostate and seminal vesicles. Dose distribution was calculated with a pencil beam convolution algorithm with pixel-by-pixel inhomogeneity correction. The prescribed dose was normalised to 100% at the isocentre and 95% isodose surface covered the PTV. The maximum isodose within the PTV was 107%. Multiple beam plans were created and compared using dose volume histograms and images before selecting the optimal plan. Digital reconstructed radiograph (DRR) image from the axial CT images was created to visualize the fields of the selected plan. With the patient positioned in immobilization cast in simulator-CT, fluroscopic simulation and field marking was done. The DRR of the plan was used for field marking. Axial CT scan was done in simulator-CT for precise verification and isocenter marking (Figure
1). Following field markings, the 3D beam plan was transferred from planning to linear accelerator computer workstation through network. The MLC field shape in linear accelerator was checked with BEV printout of all fields from the 3D planning system. 3D-CRT was delivered in linear accelerator with patient immobilized in supine position. Treatment delivery was controlled by network. Field verification with online EPID was done before the first fraction.
Patient evaluation was performed thrice weekly during treatment. Follow-up evaluations were at 3-6 month interval thereafter. Acute and late rectal radiation toxicity was graded according to RTOG criteria.[5]
RESULTS In 51 patients with M0 stage adenocarcinoma prostate treated with 3D-CRT, the median age was 68 years. Of the 51 patients, the primary curative treatment in 41 was 3D-CRT in our hospital. The remaining 10 patients were treated for recurrent prostate tumor, after they had treatment elsewhere with orchidectomy and hormone therapy or prostatectomy. In this 41 patients, 22 were in T2N0 and 19 were in T3N0 stage group. The pre-treatment PSA was < 10 ng/ml in 10 and >10 ng/ml in 31 patients. The Gleason′s score was < 6 in 18 and > 7 in 23 patients.
The median dose to the prostate PTV in the entire cohort of 51 patients
was 72 Gy. One patient with external and internal haemorhoids received
64.8 Gy. Two patients with T2N0 stage had transperineal
brachytherapy to a dose of 16.5 and 20 Gy followed by 3D-CRT to 45 and
40 Gy respectively. The remaining 48 patients received > 70
Gy (range 70-76 Gy).
Of the total of 51 patients, 35 have survived, 5 were lost for follow-up and 11 have died. The median follow up for the surviving patients is 32 months (range 24-72 months). In this group 32 are alive, disease free with biochemical control (PSA < 1 ng/ml) at a median time of 31 months. In the 11 patients who have died, 8 died of progressive disease. One patient with second malignancy and 2 with intercurrrent illness died with prostate tumor under control. In the 5 patients who were lost for follow-up, 2 did not report after completing 3D-CRT. The other 3 were disease free during their last visit at 6, 16 and 29 months respectively.
Acute rectal toxicity evaluated during treatment and for 3 months after completion of 3D-CRT in 51 patients was grade 0 in 4, grade I in 31 and grade II in 16. The late rectal complications in 49 patients who had at least 6 months follow up (41 had minimum 24 months follow up) was grade 0 in 41, grade I in 3 and grade II in 5. None had greater than grade II acute or late rectal toxicity.
DISCUSSION
Trends and predictions of cancer incidence projected by Indian Cancer Society, Bombay Cancer Registry upto the year 2002, identified prostate cancer as one of the common cancer in Mumbai occupying the fourth position of the leading cancer by site.[6] Prostate cancer is the most frequently diagnosed non-skin cancer in the Western male population.[7] The prostate cancer clinical guidelines panel of the American Urological Association recommended radiation therapy as an important option in management of localized prostate cancer.[8] A comparison of external beam therapy versus radical prostatectomy for 382 patients with low risk prostate carcinoma treated at a single institution revealed similar 7 year rates of biochemical control and cause specific survival.[9]
Radiation dose to the prostate has been found to be an important predictor of local control and relapse free survival. In 738 patients with localized prostate cancer, radiation dose of > 72
Gy, resulted in biochemical relapse free survival of 85% versus 54% for dose <72
Gy.[10] However the incidence of long-term complication increases with doses exceeding 70 Gy.[11]
The radiation dose planning and delivery techniques have evolved from 2D to 3D treatment with increased ability to deliver higher target dose.[12] 3D-CRT overcomes the limitation of normal tissue toxicity. In 3D-CRT the prescribed radiation doses conform to the outline of planned target volume in its entire 3D configuration. Therefore the risk of underdosing the target is reduced. Effective exclusion of normal tissues permits dose-escalation to the target to high levels.
Fox Chase Cancer Centre dose-escalation study in prostate cancer by 3D-CRT
showed a significant improvement in biochemical freedom from failure (bNED)
as assessed by serum PSA. The 3 year bNED rates were 36% and 69% with
70 and 80 Gy respectively.[13] Since a significant proportion of local or regional failures occurs 3 years beyond treatment, the 5 year follow-up of the above study confirmed the three year results of increased bNED with doses of above 70 Gy.[3]
Dose-escalation studies using 3D-CRT is an ongoing clinical trial at Memorial
Sloan Kettering Cancer Center. From baseline dose of 64.8 Gy, increments
of 5.4 Gy have been evaluated upto 81 Gy.[14] The
initial clinical response was dose dependent with 90% of patients
receiving 75.6 Gy or 81 Gy achieving a PSA nadir of < 1.0 ng/ml
compared to 76% and 56% for those treated with 70.2 Gy and
64.8 Gy respectively.
Dose-escalation with 3D-CRT has been identified as an independent prognostic factor in multivariate analysis for survival.[15] With 3D-CRT dose above 74 Gy the biochemical freedom from disease, cause specific survival and overall survival was significantly higher than dose below 74 Gy. Lyons et al.[10] proposed
that radiation dose exceeding 72 Gy should be considered the standard care
following their evaluation of 738 patients where with dose above 72 Gy
the biochemical relapse free survival was 85% at 5 years compared to 54% for
dose below 72 Gy.
The other major dose-escalation report in prostate cancer is from MD Anderson Cancer Centre. Pollock and Zagars[16] studied 938 men with prostate cancer at three dose levels, < 67
Gy, >67-77 Gy and >77 Gy. 3D-CRT was employed for doses of 74-78 Gy. The actuarial freedom from failure at 3 years was 61%, 74% and 96% respectively
for the above 3 dose levels.
Rectal and bladder tolerance dose have been the main blocking factors for
dose escalation in prostate cancer. With the introduction of 3D-CRT, the
early results reveal no significant increase of gastrointestinal and genitourinary
toxicity with increased dose to prostate. In 96 patients treated with 3D-CRT
to 75.6 Gy or 81 Gy the acute grade II rectal morbidity was 17% and urinary morbidity was 36%.[4] All
others had either no or grade I morbidity. No acute grade III side effects
were observed. Late rectal morbidity was nil or grade I in 85%. Grade II morbidity occurred in 15%.
The acute and late effects to high dose 3D-CRT was studied in RTOG 9406
prostate cancer trial.[17] In 262 patients of T1T2 prostate cancer, treated to dose levels of 74 Gy, the tolerance has been found to be better than expected compared historical data. The study from France in 306 patients treated with conformal radiotherapy randomized to 70 Gy or 80 Gy dose reported similar rectal toxicity in both arms.[18] Morbidity evaluation from Fox Chase Cancer Centre 3D-CRT dose-escalation trial was reported on 232 patients who had a median follow up of 60 months and treated to a median dose of 71.58 Gy.[3] The
5 year grade III and IV gastrointestinal toxicity was <1%.
The post 3D-CRT prostate biopsy was obtained at or >2.5 years after
completion of therapy in 170 patients.[19] The
positive biopsy for 64.8 Gy, 70.2 Gy, 75.6 Gy and 81 Gy doses were 57%, 36%, 27% and 4% respectively.
In our report of 51 patients treated to a median dose of 72 Gy, the tolerance to treatment was excellent. None developed acute or late grade III or more rectal morbidity. The tumor response to treatment has been satisfactory.
The appropriate dose for cure of early prostate cancer is still under investigation.
3D-CRT and intensity modulated radiation therapy dose escalation studies
have provided strong evidence for radical treatment of early prostate cancer
with doses >72 Gy. These doses can be safely delivered with 3D-CRT with
no increase in gastrointestinal toxicity.
ACKNOWLEGEMENTS We acknowledge with thanks the secretarial assistance of Mrs. Bala Kannan and Mrs. Bindu Jacob.
References
| 1. | Fowler JF. Potential for increasing the differential response between tumors and normal tissues: Can proliferation rate be used? Int J Radiat Oncol Biol Phys 1986;12:641-5. Back to cited text no. 1 [PUBMED] |
| 2. | Hanks GE, Martz KL, Diamond JJ. The effect of dose on local control of prostate cancer. Int J Radiat Oncol Biol Phys 1988;15:1299-1305. Back to cited text no. 2 |
| 3. | Hanks GE, Hanlon AL, Schultheiss TE, et al. Dose escalation with 3D conformal treatment: Five year outcomes, treatment optimization and future directions. Int J Radiat Oncol Biol Phys 1998;41:501-10. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Zelefsky MJ, Fuks Z, Wolfe T, et al. Locally advanced prostatic cancer: Long term toxicity outcome after three - dimensional conformal radiation therapy - a dose escalation study. Radiology 1998;209:169-74. Back to cited text no. 4 [PUBMED] |
| 5. | Lawton CA, Won M, Pilepich MV, et al. Long term treatment sequelae following external beam irradiation for adenocarcinoma of the prostate: Analysis of RTOG studies 7506 and 7706. Int J Radiat Oncol Biol Phys 1991;21:935-9. Back to cited text no. 5 [PUBMED] |
| 6. | Yeole BB. Trends and predictions of cancer incidence cases by site and sex for Mumbai. Ind J Cancer 1999;36:163-78. Back to cited text no. 6 [PUBMED] |
| 7. | Parker SL, Tong T, Bolden S, Wingo PA. Cancer Statistics, CA. Cancer J Clin 1997;47:5-27. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Middleton RG, Thompson IM, Austenfeld MS, et al. Prostate cancer clinical guidelines panel summary report on the management of clinically localized prostate cancer. J Urol 1995;154:2144-8. Back to cited text no. 8 [PUBMED] |
| 9. | Martinez AA, Gonzalez JA, Chung AK, et al. A comparison of external beam therapy versus radical prostatectomy for patients with low risk prostate carcinoma diagnosed, staged and treated at a single institution. Cancer 2000;88:425-32. Back to cited text no. 9 [PUBMED] [FULLTEXT] |
| 10. | Lyons JA, Kupelian PA, Mohan DS, et al. Importance of high radiation doses (72 Gy or greater) in the treatment of stage T1-T3 adenocarcinoma of the prostate. Urology 2000;55:85-90. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | Smit WGJM, Helle PA, van Putte WLJ, et al. Late radiation damage in prostate cancer patients treated by high dose external radiotherapy in relation to rectal dose. Int J Radiat Oncol Biol Phys 1990;18:23-9. Back to cited text no. 11 |
| 12. | Vijayakumar S, Hellman S. Advances in radiation oncology. Lancet. 1997;349:1-3. Back to cited text no. 12 |
| 13. | Hanks GE, Schultheiss TE, Hanlen AL, et al. Optimization of conformal radiation treatment of prostate cancer: Report of a dose-escalation study. Int J Radiat Oncol Biol Phys 1997;37:543-50. Back to cited text no. 13 |
| 14. | Zelefsky MJ, Leibel SA, Gaudin PB, et al. Dose escalation with three-dimensional conformal radiation therapy affects the outcome in prostate cancer. Int J Radiat Oncol Biol Phys 1998;41:491-500. Back to cited text no. 14 [PUBMED] [FULLTEXT] |
| 15. | Hanks GE, Hanlon AL, Pinover WH, et al. Survival advantage for prostate cancer patients treated with high dose three-dimensional conformal radiotherapy. Cancer J Sci Am 1999;5:152-8. Back to cited text no. 15 [PUBMED] |
| 16. | Pollock A, Zagars GK. External beam radiotherapy dose response of prostate cancer. Int J Radiat Oncol Biol Phys 1997;39:1011-8. Back to cited text no. 16 |
| 17. | Michalski JM, Winter K, Purdy JA, et al. Toxicity after three-dimensional radiotherapy for prostate cancer with RTOG 9406 dose level IV. Int J Radiat Oncol Biol Phys 2004:58:735-42. Back to cited text no. 17 |
| 18. | Beckendorf V, Guerif S, LePrise E, et al. The GETUG 70 Gy Vs 80 Gy randomized trial for localised prostate cancer: Feasibility and acute toxicity. Int J Radiat Oncol Biol Phys 2004:60:1056-65. Back to cited text no. 18 |
| 19. | Zelefsky MJ, Leibel SA, Fuks Z. Letters to the editor. Int J Radiat Oncol Biol Phys 1999;43:235. Back to cited text no. 19 |
Copyright 2005 - Journal of Cancer Research and Therapeutics
The following images related to this document are available:
Photo images
[cr05008f1.jpg]
|

{kind=link}