
|
Journal of Cancer Research and Therapeutics
Medknow Publications on behalf of the Association of Radiation Oncologists of India (AROI)
ISSN: 0973-1482 EISSN: 1998-4138
Vol. 1, Num. 1, 2005, pp. 38-40
|
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 38-40
Original Article
A phase I trial of tocoferol monoglucoside in patients undergoing hemi-body radiation
Huilgol N.G., Nair C.K.K., Merhotra P., Kagiya
V.T.
Division of Radiation Oncology, Nanavati Hospital, Vile Parle (W), Mumbai
Correspondence Address:Division of Radiation Oncology, Nanavati Hospital, Vile Parle (W), Mumbai
nagrajh@vsnl.net
Code Number: cr05009
Abstract
Purpose: To evaluate Tocoferol monoglucoside (TMG), a water soluble vit. E. in a phase I trial, as a radiation protector in those undergoing hemi-body radiation for disseminated disease.
Materials and Methods: Patients scheduled to receive modified hemi-body radiation were accrued for the study. Patients not only had disseminated skeletal disease but, were heavily pretreated Seven patients were accrued for the study. Patients received 1 and 2 gms of TMG. 30-40 minutes before hemibody radiation. A dose of 600 cGy was delivered on telecobalt equipment at mid plane. Immediate Toxicities were evaluated as well as response to pain.
Results: All the seven patients underwent radiation uneventfully. There was no drug related toxicity. Pain relief was adequate.
Conclusion: Tocoferol monoglucoside an effective antioxidant with
no significant acute toxicity, when administered in a dose of 1 or 2
gms per oral route. TMG being water-soluble can have global antioxidant
and radio protective effects. This needs further clinical evaluation.
Keywords: Tocoferol Monoglucoside, Hemidbody Radiation, Radiation Protector,
Anti Oxidant
Introduction
Injury to normal tissue is an inevitable consequence of therapeutic radiation. The degree of injury depends on dose, fraction size and radiation technique. The pathogenesis of normal tissue is complex and dynamic changes take place over a period of time to manifest as acute and late radiation reactions. Acute and chronic normal tissue reaction are dose limiting and impose constraints on the total deliverable dose. Radiation protection of normal tissues with pharmacological intervention, which can have considerable impact on clinical outcome, was first proposed in 1940.[1]
The search for an ideal radiation protector has been going on relentlessly since 40s. Amifostine is the only molecule to have gained a wider acceptance in the clinic.[2] The mechanism of cytoprotection by amifostine against ionizing radiation in various tissues is complicated. Amifostine after dephosphorylation acts as a free radical scavenger, that protects subcellular components like membranes and DNA from damage.[3-5]
Tocoferal monoglucoside (TMG) is a water-soluble vitamin E. Vitamin E is one of the most potent free radical scavengers, which significantly reduces chemical damage to DNA and cell membrane peroxidation.[6]
TMG like, amifostine has the potential of an efficient radical scavenger,
hence, a cytoprotector against radiation induced cellular injury. This
study is the report of phase I trial of TMG in those patients who underwent
hemi-body radiation.
Pharmacology and Chemistry
Tocopherol monoglucoside (TMG) is a highly water-soluble derivative of a-tocoferol where the isoprenoid side chain of a-tocopherol is replaced by a glucose moiety through a a-glycosidic
bond. Figure 1 shows structure of various Vit.E derivatives. TMG has been shown to be an effective radical scavenger with a greater intracellular permeability due to its higher water solubility. It is shown to be an effective DNA protector.7],8]
TMG is an amorphous white powder, which is sensitive to light. It is highly soluble in water, the solubility being 100g/100ml water. The octanol: water coefficient of TMG is 3.5 suggesting a very high lipophilicity.
The high water solubility is attributed to glucose moiety while; higher lipophilicity could be due to chroman unit of TMG. Figure
1 shows the structure of TMG.
TMG can be administered orally or intravenously. TMG when administered orally reaches a peak plasma level within 10-15 minutes while intravenously the plasma peak is reached instantaneously. The drug is completely eliminated within 2 hours of oral and i.v. administration.[9]
The drug when administered intraperitoneally at 1.5 gm/kg body weight proved fatal in all the studied mice.[10]
Elimination has bi-exponential decay suggesting equilibration of the drug in both central and, peripheral compartment at two different rates. The drug is well tolerated though intraperitoneal administration of TMG in mice proved to be more toxic. Oral administration of TMG up to 7g/kg body wt. was well tolerated in mice.
Mechanism of action
TMG is analogous to a-tocopherol, a compound known to protect DNA, cell membrane and, other targets for damage, by scavenging free radical. TMG with high lipophilicity and water solubility can scavenge free radicals more effectively than the parent compound. It also has a greater cellular penetration.
TMG has been shown to be a radioprotector in the lab. Thymine glycol concentration, a marker for radiation damage has been shown to decrease with increasing concentration of TMG. This suggests[11] a decrease in radiation-induced lethality due to TMG. It has been demonstrated that TMG can protect cells against radiation induced single strand breaks as well as damage to cell membrane.[12]
The LD50 (30) for mice receiving whole body radiation increased from 6 to 6.48 Gy following per oral administration of 2g/kg of TMG. TMG has shown to be an effective radiation protector in mice and in vitro experiments.[13]
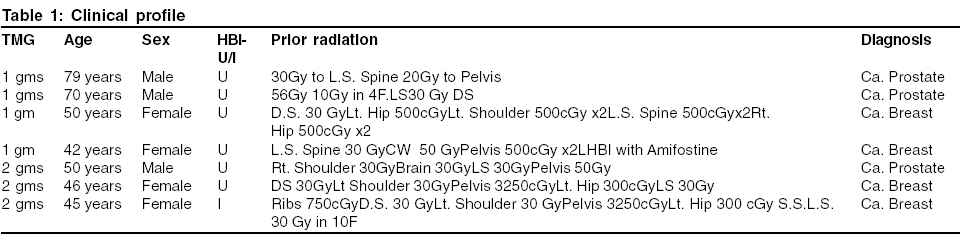
Materials and Methods Patients with disseminated skeletal disease and scheduled for modified hemi-body radiation, were accrued for this phase I study to assess the feasibility of administering water soluble Vit. E (TMG) as a radiation protector. Three patients with cancer of Prostate and, three other with cancer of breast were included following documentation of previous treatment schedules and clinical details. All the patients qualified to be on step II analgesia management with opioid analgesics with moderate pain. None of the patients had fractures or neurological deficits due to metastases. Patients underwent routine hematological checks including complete blood counts with platelets and, serum creatinine. It was mandatory for the patients to have had white blood counts at a minimum of 4000 c/cc and platelets above 107. Patients with severe renal impairment were not eligible for this study. Table
1 shows the clinical details of six patients included in the study. All the patients received modified HBI. Upper HBI included the field from root of neck to umbilicus, while, lower HBI, included the field extending from L2-3 to upper third femur. Patients were treated with parallel opposed fields on telecobalt (Theratron 80, AECL) at 80 cms, SSD but, without any compensators. The dose was calculated at maximum separation. A dose of 600 cGy single session was delivered to UBI while 800cGy was delivered to LBH. All patients received oral antiemetics like ondensetron 8mgs thrice a day and half an before radiation. TMG was administered orally half an hour prior to radiation. The first four patients received 1 gm. of TMG while three others received 2 gms.
Acute GI toxicities were scored following radiation and hematological parameters were repeated after a week. A WHO criterion was adopted.[14]
Results
Table 1 shows the clinical profile of patients included for the study. All the patients were heavily pre-treated with radiation, surgery and chemotherapy. All patients following HBI complained of mild nausea and, further loss of appetite. None of the patients showed any significant drop in white blood count done after one week of radiation. A ten percent drop or counts over the baseline was to be considered change due to radiation. None of the patients had febrile episodes.
All patients showed improvement in pain though non-narcotic analgesics were continued. All patients had acceptable and anticipated GI and hematological toxicities, which meant TMG, did not add to the known toxicity profile. Oral administration of TMG was acceptable. There were no fatalities within 30 days of the treatment.
Discussion Cytoprotection following ionizing radiation is a complex and dynamic phenomenon. Ionizing radiation induces scavengble and nonscavengable injury. Thus free radical scavengers can only partially prevent the injury if present during the interaction of radiation cells. TMG an analogue of Vit.E, like Trolox is a better scavenger of free radicals due to its higher water solubility and greater cellular penetration. TMG has been shown to scavenge various free radicals to effectively protect DNA and membranes against ionizing radiation.[15]
Besides, animal studies also suggest a pro-oxidant role in tumour bearing mice. (Personal communication Dr. C. K. K. Nair). A role of selective sensitization of tumour was purported following this study.
TMG if effective can be a global protector as it can penetrate the blood brain barrier unlike Amifostine. This study has shown the safety of administering adequate single dose of TMG in previously treated patients undergoing hemi-body radiation. The next step is to ensure the safety of long-term administration. TMG with pro and antioxidant potential at various concentrations has, the potential to be a good cytoprotector in the clinic. It′s a purported pro-oxidant and its sensitization potential may make it an ideal molecule to widen the narrow therapeutic ratio of clinical radiation.
References
| 1. | Pan HM, Tyree EB, Strause RC. Cysteine protection against x-radiation. Science 1949;110: 213-4. Back to cited text no. 1 |
| 2. | Wasserman TH, Radiotherapeutic studies with amifostine (Ethyol) Semin. Oncology 1994;21:21-5. Back to cited text no. 2 |
| 3. | Hall EJ. Radioprotectors: Radiobiology for the radiologist. Philadelphia, PA: Lippincott; 2000. p. 136-46. Back to cited text no. 3 |
| 4. | Travis EL. The oxygen dependence of protection by aminothiols. Implications for normal tissues and solid tumours. Int J Radiat Oncol Biol Phys 1984;10:1495-502. Back to cited text no. 4 |
| 5. | Denekamp S, Michael BD, Rojas A. Radioprotection of mouse skin by WR-2721: The critical influence of oxygen-tension. Int J Radiat Oncol Biol Phys 1982;8:531-4. Back to cited text no. 5 |
| 6. | Claycambe KJ, Meydani SN. Vit.E and genome stability, a tocoferol. Mutation Research 2001;37:475. Back to cited text no. 6 |
| 7. | Kapoor S, Mukherjee T, Kagiya VT, Nair CKK, Redox reactions of tocopherol monoglucoside in aqueous solutions: A plus radiolysis study. Radiat Res 2002;43:99. Back to cited text no. 7 |
| 8. | Inhibition of gamma radiation induced DNA - damage in plasmid pBR322 DNA by TMG, a derivative of vitamin E. J Radiat Res 2002;42:153. Back to cited text no. 8 |
| 9. | (unpublished data by Nair CKK). Back to cited text no. 9 |
| 10. | Nair CKK, Umadevi P, Shiman SRN, Kuniguta HM, Yeun-Hwa Gu, Kagiya VT, Water Soluble Vit. E as a radioprotector. Indian J Exp Biol 2003;41:1365-71. Back to cited text no. 10 |
| 11. | Thomas MJ, Bielski BHJ, Oxidation and reaction of Trolox-C, a tocopherol analogue 8in aqueous solution A pulse radiolysis study. J Am Chem Soc 1999;111:3315. Back to cited text no. 11 |
| 12. | Rajagopalan R, Wani K, Huilgol NG, Kagiya VT, Nair CKK. Inhibition of gamma-radiation-induced DNA damage in plasmid pBR322 DNA by TMG, a derivative of Vitamin E. J Radiat Res 2002;42:153. Back to cited text no. 12 |
| 13. | Nair CKK, Umadevi P, Shimanskaya R, Kunugita N, Murase H, Yeun-Hwa Gu, et al. Water soluble Vit E (TMG) as a radio protector. Indian J Exp Biol 2003;41:1365-71. Back to cited text no. 13 |
| 14. | A Practical Guide to EORTC Studies. Hawthorn J, Vantongelen K, editors. 1994. p. 116-8. Back to cited text no. 14 |
| 15. | Salvi VP, Satav JG, Kagiya VT, Nair CKK. Radioprotection membrane damage by TMG. International conference on Natural Antioxidants and Free Radicals in Human Health and Radiation Biology, Mumbai: Abstract Book; 2001. p. 188. Back to cited text no. 15 |
Copyright 2005 - Journal of Cancer Research and Therapeutics
The following images related to this document are available:
Photo images
[cr05009t1.jpg]
|

{kind=link}
{kind=link}