 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 41-45 Original Article Programmed cell death as a prognostic indicator for radiation therapy in cervical carcinoma patients: A pilot study Bhosle S.M., Huilgol N.G., Mishra K.P. Radiation Biology and Health Sciences Division, Bhabha Atomic Research Centre, Mumbai - 400 085 Code Number: cr05010 Abstract Purpose: In clinical practice, radiation therapy often fails in cervical carcinoma stage IIIB and there is a need to develop a predictive assay for prognosis of radiation treatment outcome in cancer patient. We have attempted to evaluate the relevance of changes in Membrane Fluidity (MF) and associated apoptotic cell death in cervical cancer cells after first fractionated dose of radiation therapy to treatment outcome of stage IIIB cervical carcinoma patients.
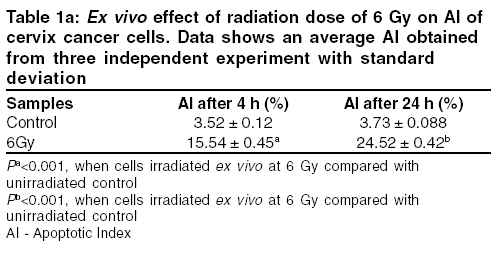
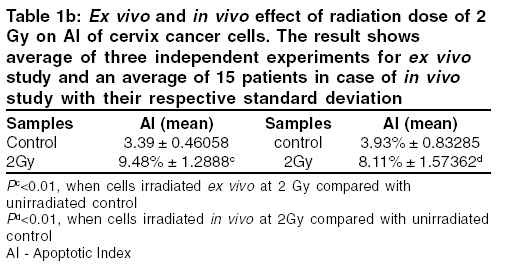
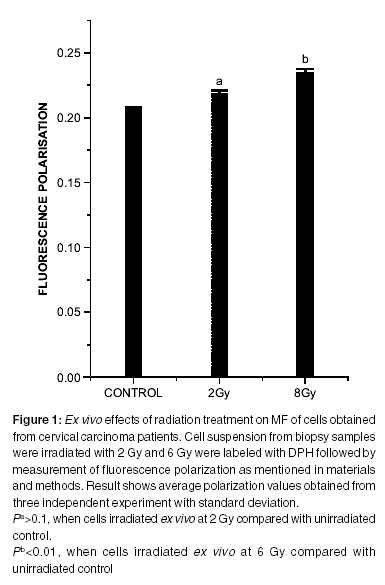
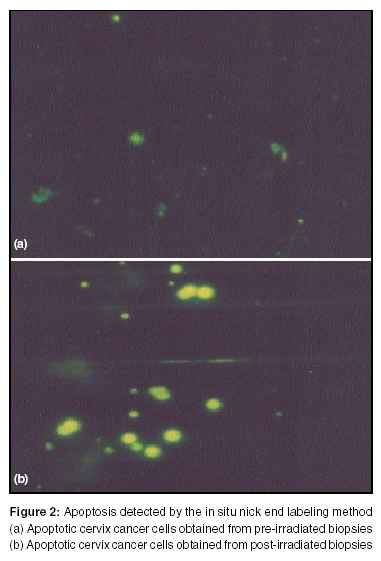
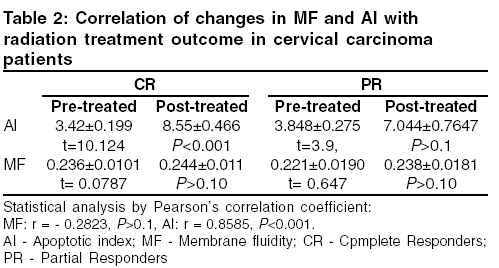
Introduction Cancer of uterine cervix is the most common cancer amongst women in developing countries and the second most prevalent cancer world over.[1-3] Human papillomavirus (HPV) is the major cause of cervical carcinoma and other risk factors such as hormones, cigarette smoke, dysregulation of oncogenes and tumor suppressor genes are believed to be involved in malignant transformation.[4-6] Cervical carcinoma patients with extensive locoregional prevalence have a high rate of local relapse when treated surgically. Therefore, patients with stage IIB, IIIB or IVA tumors are treated with radiotherapy which are reported to show the survival rates of 65, 40 and less than 20% respectively after 5 years.[4] Cellular effects associated with dose fractionation and low dose rate irradiation of cells are accepted as useful protocols in clinical radiotherapy. Radiation is suggested to induce apoptosis in large number of major functional and structural cells of lymphoid tissue but the role of apoptotic tumor regression in radiation therapy outcome of cancer remains unclear.[7],[8],[9] Apoptosis is a fundamental biological process that is observed in normal embryonic development, aging and in some tissues in response to both chemical and physical stresses. It is characterized by condensation of chromatin, nuclear fragmentation, loss of surface contact, shrinkage of the total cell volume and increased cell density.[10] A thinking is gaining ground that DNA damage may be necessary but not sufficient to induce cell death. Ionizing radiation induced oxidative damage in susceptible membrane phospholipids may cause the significant alteration in membrane function and structure possibly leading to apoptosis.[11],[12],[13] A physical and chemical change in lipid bilayer induced by radiation and a relationship between radiation induced membrane oxidative damage and apoptosis has been indicated in liposomal model membrane as well as in cell membrane.[14],[15],[16] The importance of membrane as a target for ionizing radiation was thus identified as delayed or indirect consequence of the damage.[17] Studies have reported radiation induced rigidization of membrane i.e, decrease in MF due to oxidative damage.[17],[18] The factors controlling apoptotic pathway have provided a deeper molecular insight on pathogenic mechanisms leading to cancer and intrinsic cellular radiosensitivity to apoptosis is considered important in determining radiation treatment outcome in cervical carcinoma patients.[18],[19],[20] Materials and methods Sample collectionBiopsy samples were collected from 15 patients with the informed consent in the age group of 40-60 with stage IIIB cervical cancer patients who received only radiation therapy at Radiation Oncology Department of Nanavati Hospital, Mumbai. The classification of disease in cervix cancer patients is according to TNM system (4th Ed. 1987). Patients were categorized under stage IIIB as per the International Federation of Gynecology and Obstetrics (FIGO) and the World Health Organization (WHO). All patient were irradiated with Co60 g-rays by Theratron 780C (Atomic Energy of Canada Ltd., Chalk River, ON, Canada), a telecobalt equipment. Patients were treated at a dose rate of 1.2-1.4 Gy/min with a parallel opposed field, box technique or with multiple beams to encompass the entire pelvic disease. The upper margin of the field was placed at the L5/S1 junction, whereas the lower margin included the lowest palpable disease with a centimeter of margin. All patients received 70 Gy with conventional fractionation (2 Gy daily with no radiation on Saturday and Sunday). For ex vivo studies cell suspension obtained from unirradiated biopsies were irradiated at a dose rate of 0.55 Gy/min with Co60g-rays by Theratron and incubated at 370C in CO2 incubator. The initial response as assessed clinically was categorized as complete or partial by the WHO criterion. In accordance with the established clinical practice, patients showing complete regression of clinically detectable tumor were considered as Complete Responders (CR) and those showing less than complete response but more than 50% tumor regression were considered as Partial Responders (PR). Preparation of cell suspension: The biopsy samples were collected in DMEM with 25% glycerol before and 24 h after radiation therapy and stored at -20° C under similar condition. Cell suspension was prepared under sterile conditions from biopsy samples obtained from patients in DMEM by mincing with curved scissor for 20 minutes and filtering twice through nylon filter. The cell suspension obtained were washed twice with DMEM and the viability of samples was determined by trypan blue (0.04% w/v) dye exclusion method. Cell suspensions were stored in DMEM with 25% glycerol at -20° C and further experiments were performed using the stock suspension. Measurement of MF of cervix cancer cells by DPH probe For fluorescence polarization studies, 1 ml of 1,6-Diphenyl 1,[3],5-Hexatriene (DPH) 100 mM in Dimethyl Sulphoxide (DMSO) was incubated with 2.5 ml of cell suspension (1x106 cells) in Phosphate Buffer Saline (PBS) for 20 min at 25° C followed by measurement of polarization as described by other investigators.[13] Measurement of AI by TUNEL method The percentage apoptosis in cervical carcinoma cells (1x106 cells) in (PBS) was determined by TUNEL method following the protocol provided with kits using fluorescence microscope (Optophot 2, Nikon, Japan). A minimum of 400 cells were randomly counted from the sample population to determine AI. Statistical analysis The decrease in MF and increase in AI in cervical cancer cells obtained from biopsies of patients after radiation treatment compared with control were evaluated by Student′s t-test. The significance of correlation of the changes in MF and AI with radiation treatment outcome of the patients were determined by Pearson′s correlation coefficient test. Results Measurement of AICervix cancer cells were irradiated ex vivo at 6 Gy and apoptosis was measured in irradiated samples and unirradiated control after 4 h and 24 h. A time dependent increase in AI in irradiated samples as compared to the control was measured by TUNEL assay (Table 1a). A significant increase in AI was detected in cells obtained from patients irradiated with first fractionated dose of 2 Gy as compared to the cells from the same patients before irradiation and also in cervix cancer cells irradiated ex vivo at 2 Gy (Table 1b). Apoptotic cancer cells of cervix cancer patient before and after radiation treatment stained with FITC labeled nucleotide are shown in Figure 1. Measurement of MF The cervix cancer cell suspension obtained from biopsies of patients were irradiated with Co60 g-rays ex vivo at the dose of 2 and 6 Gy and MF was measured by DPH polarization method. A significant increase in fluorescence polarization was observed in samples irradiated with 6 Gy as compared to control (Figure 2). Change in AI and MF after radiation treatment and prognosis of the patient The change in AI of pre-treated and post-treated cervix cancer cells showed significant P value ( P <0.001) in CR group and insignificant P value ( P >0.1) in PR group. A variation in the significance level of the difference in AI was seen between the two groups. A positive correlation (r = 0.8585) of changes in AI with treatment outcome of patients with a significance of P <0.001 was obtained (Table 2). The changes in the MF of the pre-treated and post-treated cervix cancer cells in both CR and PR groups showed insignificant P values with no difference in the significance level of the changes in MF between the groups. A negative correlation of MF with treatment outcome of patients is not significant (r = -0.2823, P > 0.1). Discussion Carcinoma of the cervix is a tumor that is well suited for studies to examine the clinical applicability of laboratory based predictive assays for radiotherapy as it is a cancer which in many patients is treated by radical radiotherapy alone with 40-60% of five years survival rate and for which local reccurence rates are in the range of 3-6% for stage 1 to 45% for stage III disease.[19],20][,[27] It is commonly observed that radiation therapy is not always successful in stage IIIB uterine cervix cancer patients. Hence, there is a need to predict radiation response in the beginning of radiation therapy i.e. after giving first fractionated dose of 2 Gy. Many factors like stage, tumor volume, lymph node status, tumor differentiation and age are considered as possible indicators of prognosis of patients with carcinoma of the cervix. Several cytosolic antioxidant enzymes and proteins are suggested for use as biomarkers to predict response of radiation in cancer patients,[27] but predictive assays developed so far are inadequate for predicting radiation therapy prognosis in cancer patients. To our knowledge data are not available on the changes in structure and properties of membrane bilayer after radiation therapy and its possible correlation with the clinical outcome of radiation treatment. We have investigated the changes in lipid bilayer MF and the rate of apoptosis after treatment with first fractionated dose of radiation as a factor for predicting tumor regression after completion of radiation therapy. A decrease in MF of cells irradiated ex vivo at 6 Gy suggests rigidization of the cell membrane, indicative of oxidative damage to the cervix cancer cell membrane. It has been suggested that marked alteration in DPH probe environment in the hydrophobic region of the bilayer and fluorescence decay is correlated with radiation peroxidative damage in artificial membrane.[28] A significant decrease in antioxidant enzyme superoxide dismutase level (SOD) and an increase in AI was earlier observed in cervix cancer cells obtained from biopsies of patients irradiated with 2 Gy as compared to the unirradiated control.[29] Results suggested that one of the cause of membrane oxidative damage may be mediated through lipid peroxidation and the rigidization of the cervix cancer cell membrane after radiotherapy might be due to decrease in the level of the antioxidant enzyme SOD. In view of ex vivo data, studies were designed to predict radiation response in terms of changes in MF and AI after giving first fractionated dose of radiation in cervix cancer patients.. A negative correlation between MF and treatment outcome was not found to be significant. Radiation induced apoptosis has been intensively investigated in intestinal crypts, thymocytes and lymphocytes. The rate of spontaneous apoptosis in solid tumors including cervical carcinoma are not more than 10%, but there is a possibility of induction of increased apoptosis by irradiation in tumors. In an earlier report, significant increase in AI at 5th dose was seen in cervix cancer cells as compared to that of prior to radiation treatment.30],31] It is seen that AI in cervix cancer cells obtained from patients prior to radiation treatments is in the range of 3.5-5% as measured by TUNEL assay. AI increases by 2-3 fold in the patients 24 h after 2 Gy of radiation therapy. This significant increase in AI was seen to be associated with CR in patients i.e, the change in AI after radiotherapy is significant in CR group whereas it is found to be insignificant in PR group.This preliminary report shows marked increase in AI during early course of radiotherapy and a significant correlation with treatment outcome of patient undergoing radiation therapy. Apoptosis plays an important role in radioresponse and it has been shown that cell membrane changes are also seen following ionizing radiation. However the change in MF after radiation treatment of patient and the correlation of MF with treatment outcome are not significant. Hence a study with larger sample size is continuing in this direction and the ongoing project aims at evaluating the changes in biomarkers after first fractionated radiation dose to predict radioresponse in stage IIIB cervix cancer patients. This might have potential to develop predictive assay for radioresponse in clinical oncology. References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05010t2.jpg] [cr05010f2.jpg] [cr05010f1.jpg] [cr05010t1b.jpg] [cr05010t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}