
|
Journal of Cancer Research and Therapeutics
Medknow Publications on behalf of the Association of Radiation Oncologists of India (AROI)
ISSN: 0973-1482 EISSN: 1998-4138
Vol. 1, Num. 1, 2005, pp. 51-56
|
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 51-56
Original Article
A prospective study of pharyngocutaneous fistulas following total laryngectomy
Qureshi S.S., Chaturvedi P., Pai P.S., Chaukar
D.A., Deshpande M.S., Pathak K.A., D'cruz A.K.
Department of Surgery, Head and Neck Surgical Service, Tata Memorial Hospital, Mumbai
Correspondence Address:Head and Neck service, Tata Memorial Hospital, EB Road, Parel, Mumbai - 400 012
drchaturvedip@rediffmail.com
Code Number: cr05012
Abstract
Pharyngocutaneous (PC) fistula is a common complication following laryngectomy.
It leads to increased morbidity, delay in adjuvant treatment, prolonged
hospitalization and an increase in treatment costs. Although a number
of factors that result in PC fistula have been described, there is still
no agreement on the most significant factors. We undertook a prospective
study to critically analyze PC fistula and its association with various
tumors, patient and treatment related factors. This was a prospective
study that included 143 patients who underwent laryngeal surgery for
squamous cell carcinoma of the larynx and pyriform sinus. Use of pectoralis
major myocutaneous flap to reconstruct the neopharynx, primary disease
in pyriform and extensive soft tissue infiltration were significantly
associated with PC fistula. Prior treatment (radiotherapy and chemotherapy),
type of closure (T closure, Y closure and vertical closure), Layers of
closure (full thickness interrupted, submucosal interrupted, submucosal
continuous) type of suture material (silk, vicryl ), age, sex, stage,
preoperative tracheostomy, cut margin status, pre/postoperative hemoglobin
and experience of surgeons did not relate significantly.
Keywords: Pharyngocutaneous fistula, total laryngectomy, morbidity
Introduction
The development of a pharyngocutaneous fistula (PCF) is the most common
and troublesome postoperative complication following laryngectomy. Its
occurrence leads to increased morbidity, delay in adjuvant treatment,
prolonged hospitalization and an increase in treatment costs. The reported
incidence of PCF is extremely variable in the literature, ranging from
5% to 65%.[1],[2],[3] A
rate between 13 and 25%[4-23] has
been often reported and only few reports had a rate of less than 10%.[3],[24],[25],[26],[27]
Although a number of factors that result in PCF have been described, there
is still no agreement on the most significant factors. We undertook a prospective
study to critically analyze PC fistula and its association with various
tumors, patient and treatment related factors.
Materials and Methods This was a prospective study that included all patients who underwent laryngeal surgery for squamous cell carcinoma of the larynx and pyriform sinus between January 2003 to December 2004. A total of 143 laryngectomies were performed during this period. All the patients had similar pre-operative/post-operative care. We studied all the previously reported factors that could influence fistula formation such as - age, sex, site of primary, T stage, extent of nodal dissection, soft tissue infiltration, prior treatment (radiotherapy), type of closure (T closure, Y closure and vertical closure), technique of closure (full thickness interrupted, submucosal interrupted, submucosal continuous) suture material (silk, vicryl), preoperative tracheostomy, cut margin status, serum hemoglobin and albumin level, experience of surgeons ( consultant Vs residents).
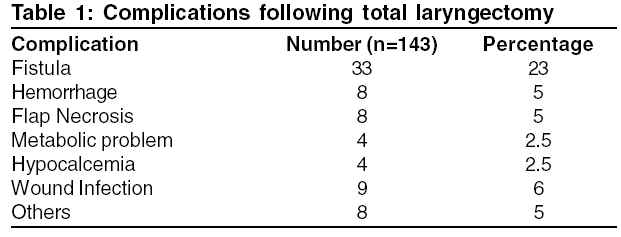
Results Two third (67%) of the patients had hypopharyngeal cancers and one third were laryngeal cancers. Of the 143 laryngectomies, 130 required total laryngectomy with or without partial pharyngectomy and 13 underwent near total laryngectomy. One hundred and five (73%) patients had primary closure of the mucosa, 18 patients required pectoralis major myocutaneous flap for neopharynx augmentation and 7 patients required a gastric pull-up. Table
1 enlists the common complications encountered in our study.
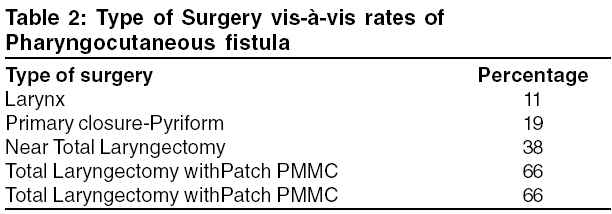
The overall fistula rate was 23% (33/143) but 14% in patients with primary closure. (Table
2) Of 18 patients who underwent pectoralis major myocutaneous flap for neopharynx reconstruction two third witnessed a PC fistula. There was no PC fistula in patients who underwent neopharynx reconstruction with gastric pull up (7/143). Majority of leaks manifested within first 2 weeks (25/33) and most appeared in the lateral part of the suture line (29/33). In most patients (27/33) the fistula healed with conservative management alone. The conservative management involved adequate drainage, neck compression and frequent dressings. In patients with evidence of infection, suitable antibiotics were used. Half of these fistulas healed within 14 days and 3/4th healed within 4 weeks. Eighteen percent of the patients (6/33) required surgical intervention by way of a myocutaneous flap for control of PC fistula. All these patients had undergone primary mucosal closure at the time of laryngectomy. The indications of were hemorrhage in 4 patients and high output fistula in 2. Following the leak, these patients required PMMC flap to cover the exposed neck vessels and to close the mucosal dehiscence. Interestingly, the PMMC did not completely stop leakage in any of these patients. It only reduced the salivary output of the fistula and probably prevented a vascular catastrophe common in such patients. 80% patients were discharged within first 2 weeks of the index surgery. Oral feeds could be initiated in nearly 2/3rd of these patients in first 2 weeks. Average hospital stay in the patients having PCF was 27 days. Three patients (9%) could not undergo planned adjuvant radiotherapy because of the leak.
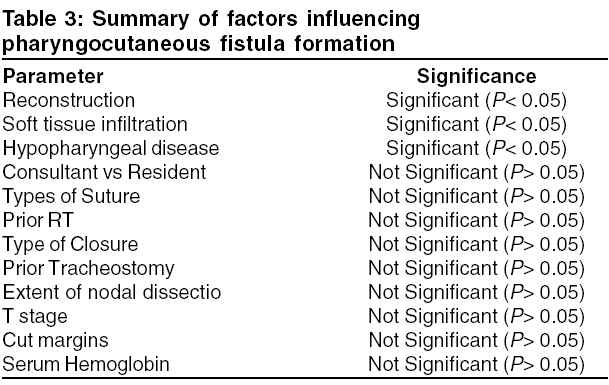
Amongst the various possible contributory factors, reconstructions, primary disease in pyriform and extensive soft tissue infiltration were significantly associated with PC fistula. (Table
3) Prior treatment (radiotherapy and chemotherapy), type of closure (T closure, Y closure and vertical closure), layers of closure (full thickness interrupted, submucosal interrupted, submucosal continuous) type of suture material (silk, vicryl), age, sex, stage, preoperative tracheostomy, cut margin status, pre/post-operative hemoglobin and experience of surgeons did not relate significantly.
Discussion
Even though much controversy still surrounds the prevention of pharyngocutaneous
fistulas, it is generally agreed that most fistulas respond well to conservative
management: figures between 60% and 80% are commonly reported.[10],[11],[14],[17],[19],[28],[29] Two
third of our fistulas also healed with conservative management. The differences
appear to be mainly related to previous radiotherapy: spontaneous closure
was achieved in 44% to 82% of previously treated patients[11],[17],[19] versus
80% to 95% of patients who had not been previously treated.[17],[20],26-28]
Local wound care (drainage, local antiseptic, removal of necrotic tissue,
curettage of the fistulous borders and tract and pressure dressing above
the flaps) should be associated with introduction of the feeding tube
and administration of general antibiotics, if signs of local infection
are present.[30] In contrast
a curious conservative approach was adopted by Fradis et al.[23] Reinsertion
of the nasogastric tube for fluid intake, oral feeding for solid foods
and suspension of antibiotic therapy favored, in their patients, granulation
tissue formation and spontaneous closure of the fistula. Even though
surgical repair has been performed after more than 3 months of conservative
treatment,[5],[7],13][,26][ but
if closure of the fistula is not obtained in a month with medical management,
it is not wise to wait any longer and surgery should be planned.[30] Cure
of infection is an important prerequisite for a successful outcome. Many
surgical options are available,[4],[13][,31-38]
and the choice of the surgical technique should be dictated by the diameter
of the fistula and previous radiation history. Along with direct suture
or local flaps, the favored reconstructive methods are deltopectoral
and pectoralis major myocutaneous flaps5][,[7],[10],[11],[13],[14] In
recent years, reconstruction with free flaps such as the radial forearm
and jejunal has gained some popularity.[36-40] None of our patients who
had undergone fee jejunal flap for pharynx reconstruction witnessed PCF.
The observation in our study suggests that though PMMC in patients having
fistula, reduces the salivary output, does not totally stop it. Probably
it gives a vascular cover to the exposed neck vessels and prevents a
vascular catastrophe.
The type of surgery is one of the less controversial predisposing factors for fistula development in the literature, and extended laryngectomy invariably carries a higher incidence of fistulization by a factor of two or more.5],10-13,24],29] Resection of large amount of pharyngeal mucosa leads to closure made under tension. These wound are more prone for break down and formation of PCF.[41] In
our study, the pyriform disease appeared significantly associated with
PCF because of the above mentioned reasons. A pyriform primary necessitates
partial pharyngectomy along with total laryngectomy. Since 2/3rd of our
patients have advanced pyriform disease, our average leak rate (25%) may appear very high. The leak rate dropped to half (11%) the average rate (25%)
when patients underwent laryngectomy alone.
Many authors believe that delayed oral feeding reduces fistula formation
after laryngectomy as there is no stress on the suture line due to feeding.
In our study, three fourth (75% and 25/33) of our patients had leak
in less than 2 weeks i.e. before the oral feed was initiated in them. A
poll conducted by Boyce and Meyers[20] revealed
that 84.5% of the practicing head and neck surgeons wait at least 7 days to feed their patients after laryngectomy, and only 2.8% feed
at 4 days or before. However, there is little evidence to support the view
that the timing of oral feeding influences fistula formation following
laryngectomy, and in most cases, PCF had developed before the patients
received any oral feeding. Most authors20],21],42],43] no longer consider delayed oral feeding necessary until after the seventh postoperative day unless fever, wound erythema, swelling, or continuous elevated drainage (which raise the suspicion of an impending fistula) is present. A few authors did not even adopt the nasogastric tube and instead started oral feeding on the first[22] or the third[27] postoperative day. Moses et al[21] reported a lower incidence of fistula in the group of patients who resumed feeding on postoperative day 7, whereas it was much higher in patients who did so after 7 days. Aprigaliano[27] reported
a 9% fistula rate without use of nasogastric tube and oral feeding
on postoperative day 3.
Numerous patient related factors have been studied for their role in causation of PCF. Patients requiring a tracheostomy prior to surgery are at increased risk of developing a PCF.[13] It is probably due to contamination and the higher T stage. This did not happen in our study. Few other authors have reported similar experience where prior tracheostomy was not found to be a risk factor for PCF.44],45]
Pre/postoperative hemoglobin level lower than 12.5 g/dL have been associated with PCF.28],30] Zinis et al[30] found a nine fold increase in the risk of PCF. Horgan et al[13] also
found a rise in the number of fistulas in patients with hemoglobin values
less than 11.5 g/dl. Postoperative anemia is a consequence of high intraoperative
blood loss and can be compared to the need for intraoperative transfusion
which significantly increased the incidence of PCF from 7% to 28% in
the report by Hier et al.[14] On the other hand preoperative hemoglobin has not been found to be a significant risk factor.[41] We did find such a relation in our study. May be the sample size was inadequate to reach to such a conclusion in our study.
The anesthesiologic risk which is mainly an index of concomitant diseases
was associated with a 19% fistula rate compared to 4% in
patients without concomitant diseases.[26] This view is also supported by Horgan et al[13] and Cavalot et al.[45] Conversely Zinis et al[30] did not found concomitant diseases to be predictive of fistula formation. Age, sex, smoking, alcohol, preoperative hemoglobin, Karnofsky performance status, body mass index have not been considered as significant factors increasing the risk of PCF.[41] We had similar findings in our study too.
The role of previous radiotherapy has been extensively reported in the
literature. Grau et al[46] in
a large series of 472 patients undergoing salvage laryngectomy after radiotherapy
reported a PCF rate of 21%. Numerous authors have also found significant
correlation with radiotherapy and PCF[4],8-10,[26],[27],[29],[41],45] but
at the same time some authors have also reported no correlation with radiotherapy.[11],14],15],23-25,30] In
our subset of 13 patients who had prior RT before laryngectomy, there was
no significant increase in fistula rate. As regards to the time between
radiotherapy and surgery some authors did not find any significant correlation.[13],[47] However,
Hier et al[14] stated that
preoperative radiation appears to be a risk factor if surgery is performed
within 3 months. This could probably due to the vasculitis which develops
after radiotherapy and increases the risk of infection. Vasculitis generally
subsides within 3 months. Briant[48] in
contrast stated that if surgery after radiotherapy is performed within
3 months the complications were comparable between radiotherapy and surgery
alone control group. Also the fistulas appear earlier and the sizes are
significantly larger in patients with preoperative radiotherapy than in
patients with no pre-operative irradiation.[41] Bresson
et al[2] and Briant[48] found
the fistulas to be more serious and associated with higher mortality rates
in patients who had fistulas develop after radiotherapy than in a purely
surgical group of patients. In our study, majority (11/13) of the fistulas
in the post radiation laryngectomy group stopped by conservative treatment
and 2 required PMMC. The incidence of fistulas was significantly increased
in patients who received cobalt/roentgen treatment compared with those
who had been treated with photons in a few studies.6],41] Photons
have the advantage of sparing the subcutaneous tissue during irradiation.[41] Dedo
et al[49] identified a RT
dose of more than 30 Gy as a contributing factor, but Virtaneimi et al[41] did
not find the dose and height of radiation field as important for causing
PCF. McCombe et al[9] also noted
a prolonged hospital stay (112 vs. 28 days) and increased requirement of
surgical closure of PCF in patients with preoperative radical RT.
In the literature, T closure is reported as another risk factor for PCF formation.1],50] According to Shah et al[51] the
weakest point was the three-point junction, if "T" or "Y-shaped" closure
was performed. This further stresses the importance of the vertical line
repair, which was also stressed by Stell et al.[4] Soylu et al[44] demonstrated a statistically significant difference in the formation of PCF between vicryl and catgut groups, in favor of vicryl. Vicryl has unique properties when compared with catgut, in that it is much stronger, is less inflammatory, and has a longer half-life. It is believed that low PCF rate with vicryl can be explained by these properties.[44] We did not have any such experience in our study.
Association of neck dissection with fistula development is controversial.[13],[50] In
one study the incidence of PCF is reported to be increased from 11.3% to
17.5% when
neck dissection is combined with total laryngectomy.[13] Whereas
some authors have reported a lower rate of PCF in patients who had accompanying
neck dissection.[44] In our
study the neck dissection did not have significant correlation with PCF.
Advancing tumor stage has been considered as a risk factor for PCF by some
authors[7],[44],[52] however,
at the same time Hier,[14] Cavalot[45] and
Lavelle et al[28] did not
find this to be significant. We found that advanced T stage alone did not
contribute to fistula formation unless it was associated with extensive
soft tissue infiltration.
Virtaneimi et al[41] noted supraglottic tumors had significantly more leak than glottic tumors. They attributed this due to extension of the supraglottic tumors either to the vallecula or the pyriform sinus, consequently requiring excision of large amount of pharyngeal mucosa and resulting in closures performed under tension. In our study the leak rate was higher in patients with pyriform primary.
Histological infiltration of the surgical margins were found to be statistically significant in the development of PCF by Markou et al,[53] however at the same time this did not had impact on the local tumor recurrence in their follow-ups. Only 3 of our patients had tumor at the cut margin and none had PCF.
Various studies have been conducted to predict fistula as early as possible.
Some of these studies have managed to diagnose PCF within an average of
5 to 10 days.[21],[26] Krouse
and Metson[3] noted the presence
of a sinus tract 2 cm or longer on barium swallow as a predictor of a postlaryngectomy
PCF. Friedman et al[54] studied
the fever (_101.5° F) in the first 48 hours after the surgery as
an indicator of PCF and suggested that fever was an excellent tool for
early identification of PCF. The relevance of wound amylase concentration
for early detection of PCF has been shown in many studies. An increase
in the wound amylase concentrations can be a useful marker in the early
identification of PCF, thus leading to early rehabilitation.[55-57] We
routinely do not employ any of the above techniques to detect or diagnose
fistula. Our diagnosis of fistula is clinical based on factors such as
- skin flap edema, neck erythema, salivary leak etc.
Much controversy also surrounds the management of laryngectomized patients
in preventing pharyngocutaneous fistula. Smith et al[58] demonstrated
a significant decreased incidence of PCF by the routine addition of a pectoralis
major myogenous flap to cover the pharyngeal defect. They also noted a
substantial and dramatic reduction in patient′s morbidity and mortality
and reduction in hospital stay, with major financial savings to the health
care system. Righini et al[59] also
confirmed the advantage of pectoralis myogenous flap in post radiotherapy
laryngectomy in a selected group of patients (with diabetes mellitus, history
of vascular disease or poor nutritional status). Prophylactic antibiotic
therapy is generally recommended. A modification of the antimicrobial prophylaxis
with the addition of metronidazole, electively used against anaerobes,
was suggested by Innes et al[60] and
systematically adopted by Cousins et al[16] and
Johansen et al,[47] all of
whom obtained a significant drop in the fistulization rate. Seikaly and
Park[42] proposed a gastroesophageal
reflux prophylaxis with continuous drip tube feeding for the first 3 postoperative
days and ranitidine and metoclopramide hydrochloride given intravenously
for 7 days. No fistula and a significant reduction in mean hospitalization
was observed in the group of patients treated with the protocol. Most authors
do not routinely perform radiographic studies, others always conduct a
contrast study because it can decrease the fistula rate,[42],61] still
others recommend the study only in patients with an increased risk of PCF
(previous radiotherapy, neck dissection, pharyngolarygectomy)[62]
Conclusion We encountered higher incidence of PC fistula because majority of the patients had cancers of the pyriform sinus, extensive soft tissue infiltration and significant proportion of them required PMMC reconstruction of the neopharynx. Subset analysis of patients with localized larynx cancers showed 11% leak rate. On the contrary, whenever extensive hypopharynx involvement necessitated removal of large areas of pharynx, leak rate increased by 6 folds. Patients who had reconstruction, though had higher leak, did not have vascular catastrophe and their leak were contained by conservative management. All 4 patients who developed post operative hemorrhage with PCF did not have PMMC reconstruction up front and required it at the time of re-exploration. Though, all these patients continued to have salivary fistula, the volume of the saliva markedly reduced and none of these patients had re-bleed. All other parameters such as - age, sex, nodal dissection, prior treatment (radiotherapy and/or chemotherapy), type of closure, Layers of closure, type of suture material, preoperative tracheostomy, cut margin status, pre/postoperative hemoglobin, experience of surgeons did not relate significantly correlate with PCF.
References
| 1. | Thawley SE. Complications of combined radiation therapy and surgery for carcinoma of the larynx and inferior hypopharynx. Laryngoscope 1981;91:677-700. Back to cited text no. 1 [PUBMED] |
| 2. | Bresson K, Rasmussen H, Rasmussen PA. Pharyngocutaneous fistulae in totally laryngectomized patients. J Laryngol Otol 1974;88:835-42. Back to cited text no. 2 [PUBMED] |
| 3. | Krause JH, Metson R. Barium swallow is a predictor of salivary fistula following laryngectomy. Otolaryngol Head Neck Surg 1992;106:254-7. Back to cited text no. 3 |
| 4. | Stell PM, Cooney TC. Management of fistulae of the head and neck after radical surgery. J Laryngol Otol 1974;88:819-34. Back to cited text no. 4 [PUBMED] |
| 5. | Dedo D, Alonso WA, Ogura JH. Incidence, predisposing factors and outcome of pharyngocutaneous fistulas complicating head and neck cancer surgery. Ann Otol Rhinol Laryngol 1975;84:833-40. Back to cited text no. 5 |
| 6. | Lundgren J, Olofsson J. Pharyngocutaneous fistulae following total laryngectomy. Clin Otolaryngol 1979;4:13-23. Back to cited text no. 6 |
| 7. | Wei WI, Lam KH, Wong J, Ong GB. Pharyngocutaneous fistula complicating total laryngectomy. Aust NZ J Surg 1980;50:366-9. Back to cited text no. 7 [PUBMED] |
| 8. | Mendelsohn MS, Bridger GP. Pharyngocutaneous fistulae following laryngectomy. Aust NZ J Surg 1985;55:177-9. Back to cited text no. 8 [PUBMED] |
| 9. | McCombe AW, Jones AS. Radiotherapy and complications of laryngectomy. J Laryngol Otol 1993;107:130-2. Back to cited text no. 9 [PUBMED] |
| 10. | Natvig K, Boysen M, Tausjψ J. Fistulae following laryngectomy in patients treated with irradiation. J Laryngol Otol 1993;107:1136-9. Back to cited text no. 10 |
| 11. | Weingrad DN, Spiro RH. Complications after laryngectomy. Am J Surg 1983;146:517-20. Back to cited text no. 11 [PUBMED] |
| 12. | Arriaga MA, Kanel KT, Johnson JT, Myers EN. Medical complications in total laryngectomy: Incidence and risk factors. Ann Otol Rhinol Laryngol 1990;99:611-5. Back to cited text no. 12 [PUBMED] |
| 13. | Horgan EC, Dedo HH. Prevention of major and minor fistulae after laryngectomy. Laryngoscope 1979;89:250-8. Back to cited text no. 13 |
| 14. | Hier M, Black MJ, Lafond G. Pharyngo-cutaneous fistulas after total laryngectomy: Incidence, etiology and outcome analysis. J Otolaryngol 1993;22:164-6. Back to cited text no. 14 [PUBMED] |
| 15. | Sellars SL. Complications of total laryngectomy. South Afr J Surg 1978;16:145-8. Back to cited text no. 15 [PUBMED] |
| 16. | Cousins VC, Milton CM, Bickerton RC. Hospital morbidity and mortality following total laryngectomy. J Laryngol Otol 1987;101:1159-64. Back to cited text no. 16 [PUBMED] |
| 17. | Cummings CW, Johnson J, Chung CK, Sagerman R. Complications of laryngectomy and neck dissection following planned preoperative radiotherapy. Ann Otol Rhinol Laryngol 1977;86:745-50. Back to cited text no. 17 [PUBMED] |
| 18. | Sheehan AJ, Shaw HJ. Total laryngectomy for squamous carcinoma of the glottis. J Laryngol Otol 1979;93:461-75. Back to cited text no. 18 [PUBMED] |
| 19. | Farrington WT, Weighill JS, Jones PH. Total laryngectomy for cancer of the larynx. J Laryngol Otol 1986;100:53-7. Back to cited text no. 19 [PUBMED] |
| 20. | Boyce SE, Meyers AD. Oral feeding after total laryngectomy. Head Neck 1989;11:269-73. Back to cited text no. 20 [PUBMED] |
| 21. | Moses BL, Eisele DW, Jones B. Radiologic assessment of the early postoperative total-laryngectomy patient. Laryngoscope 1993;103:1157-60. Back to cited text no. 21 [PUBMED] |
| 22. | Akyol MU, O¨ zdem CC¸ Elikkanat S. Early oral feeding after total laryngectomy. Ear Nose Throat J 1995;74:28-30. Back to cited text no. 22 |
| 23. | Fradis M, Podoshin L, David JB. Post-laryngectomy pharyngocutaneous fistula-a still unresolved problem. J Laryngol Otol 1995;109:221-4. Back to cited text no. 23 |
| 24. | Gall AM, Session DG, Ogura JH. Complications following surgery for cancer of the larynx and hypopharynx. Cancer 1977;39:624-31. Back to cited text no. 24 |
| 25. | Kent SE, Liu KC, Das Gupta AR. Post-laryngectomy pharyngo-cutaneous fistulae. J Laryngol Otol 1985;99:1005-8. Back to cited text no. 25 [PUBMED] |
| 26. | Papazoglou G, Doundoulakis G, Terzakis G, Dokianakis G. Pharyngocutaneous fistula after total laryngectomy: Incidence, cause and treatment. Ann Otol Rhinol Laryngol 1994;103:801-5. Back to cited text no. 26 [PUBMED] |
| 27. | Aprigliano F. Use of the nasogastric tube after total laryngectomy: is it truly necessary? Ann Otol Rhinol Laryngol 1990;99:513-4. Back to cited text no. 27 [PUBMED] |
| 28. | Lavelle RJ, Maw AR. The aetiology of post-laryngectomy pharyngo-cutaneous fistulae. J Laryngol Otol 1972;86:785-93. Back to cited text no. 28 [PUBMED] |
| 29. | Sarkar S, Mehta SA, Tiwari J, Mehta AR, Mehta MS. Complications following surgery for cancer of the larynx and pyriform fossa. J Surg Oncol 1990;43:245-9. Back to cited text no. 29 [PUBMED] |
| 30. | Redaelli de Zinis LO, Ferrari L, Tomenzoli D, Premoli G, Parrinello G, Nicolai P. Postlaryngectomy pharyngocutaneous fistula: Incidence, predisposing factors, and therapy. Head Neck 1999;21:131-8. Back to cited text no. 30 [PUBMED] [FULLTEXT] |
| 31. | Bellinger CG. Classification of pharyngostomes: A guideline for closure. Plast Recontr Surg 1971;47:54-60. Back to cited text no. 31 [PUBMED] |
| 32. | Myers E. The management of pharyngocutaneous fistula. Arch Otolaryngol 1972;95:10-7. Back to cited text no. 32 |
| 33. | Chandler JR. Treatment of pharyngeal fistulas after total laryngectomy. Laryngoscope 1979;89:671-3. Back to cited text no. 33 [PUBMED] |
| 34. | Parnes SM, Goldstein JC. Closure of pharyngocutaneous fistulae with the rhomboid flap. Laryngoscope 1985;95:224-5. Back to cited text no. 34 [PUBMED] |
| 35. | Rubin JS. Repair of post-laryngectomy pharyngeal fistulae. J Laryngol Otol 1989;103:302-5. Back to cited text no. 35 [PUBMED] |
| 36. | Bootz F, Muller GH. Repair of salivary fistulae after laryngectomy. Clin Otolaryngol 1990;15:299-302. Back to cited text no. 36 [PUBMED] |
| 37. | De Vries EJ, Myers EN, Johnson JT, et al. Jejunal interposition for repair of stricture or fistula after laryngectomy. Ann Otol Rhinol Laryngol 1990;99:496-598. Back to cited text no. 37 |
| 38. | Kimura Y, Tojima H, Nakamura T, Harada K, Koike Y. Deltopectoral flap for one-stage reconstruction of pharyngocutaneous fistulae following total laryngectomy. Acta Otolaryngol Suppl 1994;511:175-8. Back to cited text no. 38 [PUBMED] |
| 39. | Cunha-Gomes D, Kavarana NM. The surgical treatment of post-laryngectomy pharyngocutaneous fistulae. Acta Chir Plast 2001;43:115-8. Back to cited text no. 39 [PUBMED] |
| 40. | Peat BG, Boyd JB, Gullane PJ. Massive pharyngocutaneous fistulae: Salvage with two-layer flap closure. Ann Plast Surg 1992;29:153-6. Back to cited text no. 40 [PUBMED] |
| 41. | Seikaly H, Park P. Gastroesophageal reflux prophylaxis decreases the incidence of pharyngocutaneous fistula after total laryngectomy. Laryngoscope 1995;105:1220-2. Back to cited text no. 41 |
| 42. | Rodriguez-Cuevas S, Labastida S, Gutierrez F, Granados F. Oral feeding after total laryngectomy for endolaryngeal cancer. Eur Arch Otorhinolaryngol 1995;252:130-2. Back to cited text no. 42 [PUBMED] |
| 43. | Soylu L, Kiroglu M, Aydogan B, Cetik F, Kiroglu F, Akcali C, Ozsahinoglu C. Pharyngocutaneous fistula following laryngectomy. Head Neck 1998;20:22-5. Back to cited text no. 43 [PUBMED] [FULLTEXT] |
| 44. | Cavalot AL, Gervasio CF, Nazionale G, Albera R, Bussi M, Staffieri A, Ferrero V, Cortesina G. Pharyngocutaneous fistula as a complication of total laryngectomy: Review of the literature and analysis of case records. Otolaryngol Head Neck Surg 2000;123:587-92. Back to cited text no. 44 [PUBMED] [FULLTEXT] |
| 45. | Virtaniemi JA, Kumpulainen EJ, Hirvikoski PP, Johansson RT, Kosma VM. The incidence and etiology of postlaryngectomy pharyngocutaneous fistulae. Head Neck 2001;23:29-33. Back to cited text no. 45 [PUBMED] [FULLTEXT] |
| 46. | Grau C, Johansen LV, Hansen HS, Andersen E, Godballe C, Andersen LJ, et al. Salvage laryngectomy and pharyngocutaneous fistulae after primary radiotherapy for head and neck cancer: A national survey from DAHANCA. Head Neck 2003;25:711-6. Back to cited text no. 46 [PUBMED] [FULLTEXT] |
| 47. | Johansen LV, Overgaard J, Elbrond AO. Pharyngocutaneous fistulae after laryngectomy. Cancer 1988;61:673-8. Back to cited text no. 47 |
| 48. | Briant TDR. Spontaneous pharyngeal fistula and wound infection following laryngectomy. Laryngoscope 1975;85:829-34. Back to cited text no. 48 |
| 49. | Dedo HH, Alonso WA, Ogura JH. Incidence, predisposing factors and outcome of pharyngo-cutaneous fistulae complicating head and neck cancer surgery. Ann Otol Rhinol Laryngol 1975;84:833-40. Back to cited text no. 49 |
| 50. | Violaris N, Bridger M. Prophylactic antibiotics and post laryngectomy pharyngo-cutaneous fistulae. J Laryngol Otol 1990;104:225-8. Back to cited text no. 50 [PUBMED] |
| 51. | Shah AK, Ingle MV, Shah KL. Some thoughts on prevention of post-operative salivary fistula. J Postgrad Med 1985;31:95-7. Back to cited text no. 51 [PUBMED] [FULLTEXT] |
| 52. | Davidson J, Briant D, Gullane P, Keane T, Rawlinson E. The role of surgery following radiotherapy failure for advanced laryngopharyngeal cancer. Arch Otolaryngol Head Neck Surg 1994;120:269-76. Back to cited text no. 52 [PUBMED] |
| 53. | Markou KD, Vlachtsis KC, Nikolaou AC, Petridis DG, Kouloulas AI, Daniilidis IC. Incidence and predisposing factors of pharyngocutaneous fistula formation after total laryngectomy. Is there a relationship with tumor recurrence? Eur Arch Otorhinolaryngol 2004;261:61-7. Back to cited text no. 53 [PUBMED] [FULLTEXT] |
| 54. | Friedman M, Venkatesan TK, Yakovlev A, et al. Early detection and treatment of postoperative pharyngocutaneous fistula. Otolaryngol Head Neck Surg 1999;121:378-80. Back to cited text no. 54 [PUBMED] [FULLTEXT] |
| 55. | Aydogan LB, Kiroglu M, Tuncer U, Soylu L. The wound amylase concentration in the prediction of pharyngocutaneous fistula. Otolaryngol Head Neck Surg 2003;129:414-6. Back to cited text no. 55 [PUBMED] [FULLTEXT] |
| 56. | Fielder CP, Morton RP. Wound amylase estimation and the prediction of pharyngocutaneous fistulae. Clin Otolaryngol 1989;14:101-5. Back to cited text no. 56 [PUBMED] |
| 57. | Larsen LR, Schuller DE. Wound amylase levels as an early indicator of orocutaneous fistulae. Laryngoscope 1984;94:1302-6. Back to cited text no. 57 [PUBMED] |
| 58. | Smith TJ, Burrage KJ, Ganguly P, Kirby S, Drover C. Prevention of postlaryngectomy pharyngocutaneous fistula: The Memorial University experience. Otolaryngol 2003;32:222-5. Back to cited text no. 58 [PUBMED] [FULLTEXT] |
| 59. | Righini C, Lequeux T, Cuisnier O, Morel N, Reyt E. The pectoralis myofascial flap in pharyngolaryngeal surgery after radiotherapy. Eur Arch Otorhinolaryngol 2004. [Epub ahead of print] Back to cited text no. 59 |
| 60. | Innes AJ, Windle-Taylor PC, Harrison DFN. The role of metronidazole in the prevention of fistulae following total laryngectomy. Clin Oncol 1980;6:71-7. Back to cited text no. 60 |
| 61. | Giordano AM, Cohen J, Adams G. Pharyngocutaneous fistula after laryngeal surgery: The role of the barium swallow. Otolaryngol Head Neck Surg 1984;92:19-23. Back to cited text no. 61 |
| 62. | De Jong PC, Struben WH. Pharyngeal fistulae after laryngectomy. J Laryngol Otol 1970;84:897-903. Back to cited text no. 62 [PUBMED] |
Copyright 2005 - Journal of Cancer Research and Therapeutics
The following images related to this document are available:
Photo images
[cr05012t2.jpg]
[cr05012t3.jpg]
[cr05012t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}