 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
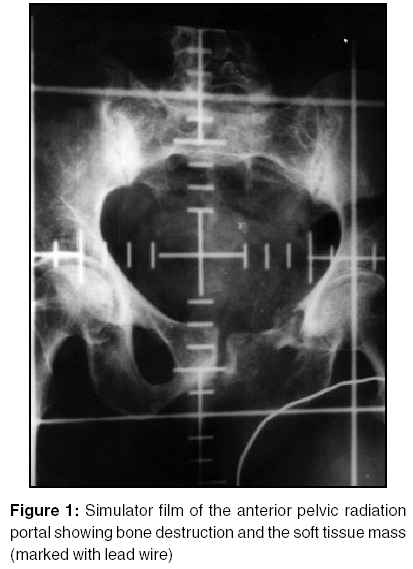
Journal of Cancer Research and Therapeutics, Vol. 1, No. 1, January-March, 2005, pp. 57-59 Case Report Management dilemmas in radiation associated pelvic sarcoma Goel Vineeta, Sarin Rajiv, Shrivastava Shyam Kishore, Desai Sangeeta, Dinshaw Ketayun A. Department of Radiation Oncology, Tata Memorial Hospital, Parel, Mumbai Code Number: cr05013 The rare occurrence of radiation associated sarcoma (RAS) is well known but the therapeutic benefit of initial radiotherapy for most cancers far outweighs the very small (0.03-0.2%) risk of RAS.[1] The vast majority of second primary solid tumours after radiation are sarcomas of bone and soft tissues and occur after a median latent period of 10 years.[2] We present a case of radiation associated osteosarcoma of pelvic bone following radiotherapy for carcinoma cervix. Using this illustrative case we have discussed the therapeutic challenges posed in the management of such patients, clinical dilemmas and the lacunae in the literature for the management of such uncommon and difficult conditions. Case Report A 61 years old lady with FIGO stage IIIB squamous carcinoma of cervix was successfully treated with a combination of external pelvic radiotherapy (antero-posterior fields delivering a dose of 50Gy in 25 fractions) and intracavitary brachytherapy (25Gy to Point A at low dose rate) in 1991. After 8 years, she developed a painful swelling of the left upper thigh. On examination she appeared elderly and her systemic and gynecologic examinations were unremarkable. There was a 10x13 cm hard mass in the upper medial aspect of left thigh. Initial fine needle aspirate of the swelling was reported as metastases from poorly differentiated carcinoma consistent with a known primary in the cervix. Since clinical index of suspicion for RAS was high, a gun biopsy was repeated from the soft tissue swelling. This confirmed high-grade matrix producing pleomorphic tumour. Immunohistochemistry revealed non-reactivity to epithelial markers (cytokeratin and epithelial membrane antigen) and a final diagnosis of osteosarcoma was made. An ill-defined osteolytic lesion involving both superior and inferior rami of pubis and left ischium with a large soft tissue mass was obvious on the X-ray. Chest X-ray and ultrasound of abdomen - pelvis were normal. A x-ray simulator film of the original radiation portal was taken (Figure 1) which confirmed that bony destruction associated with the sarcoma was well within the radiation portal and soft tissue swelling was at the edge of the portal. Considering that the tumour arose within the radiation portal after a latent period of 8 years, a diagnosis of radiation associated sarcoma was made. She was advised further local and lung imaging and the possibility of major curative surgery and the associated loss of limb function and rehabilitation were discussed in detail with her. After much deliberation, she declined further imaging as well as surgery, realizing that this treatment would involve a major amputation, prolonged and difficult rehabilitation and that her overall long term prognosis would still be poor. She was not given palliative chemotherapy or reirradiation in view of her age and the relative ineffectiveness of these modalities when used alone. She received symptomatic medical treatment and after experiencing increasing breathlessness, she died 5 months later, most probably from progressive lung metastases.Discussion Taghian et al have reported the incidence of radiation associated sarcoma [RAS] as 0.035-0.2% of all the patients undergoing radiotherapy.[1] Present criteria for the diagnosis of RAS as proposed by Murray et al[3] are (1) History of radiation exposure and the sarcoma must have arisen in the area included within the 5% isodose line. (2) No evidence of sarcoma before irradiation. (3) Pathological confirmation of sarcoma and it must clearly be different than that of a primary condition.In the largest series of 160 RAS reported from MSKCC,[2] common primary cancer were breast (26%), lymphoma (25)%, and cervix (14%). Radiation induced sarcoma of soft tissues following radiotherapy for cancer of the cervix was first described by Stanford Cade in 1957.[4] Subsequently, 27 more cases of pelvic RAS after radiotherapy for cervical carcinoma have been reported[3],[5],[6],[7] with the most common sites being buttocks, sacral region, pelvic bones and uterus. Osteosarcoma and malignant fibrous histiocytoma are the most common histological types.[7] In most reports, RAS of the bone and soft tissue arising from various sites have been grouped together and we have not come across the details of treatment and rehabilitation outcome of a case similar to ours. While surgery remains the mainstay of treatment for RAS, the resectability rate depends upon the site and size of the RAS and whether it involves bone or soft tissue. In a recent Mayo clinic series of 130 patients with RAS at various sites, the tumor was resectable only in 61(49%) patients.[8] Majority (49/61) of them had to undergo amputation. Though not reported separately, it is quite likely that the resectability rate would have been lower and amputation rate higher for RAS arising in the axial skeleton as compared to the peripheral RAS. In the MSKCC study also complete resection was possible only in 67/118 (56%) patient with localized RAS.[2] The long term survival depends upon the resectability, extent of resection and the tumour size. In the unselected group of 59 patients with various RAS reported from MSKCC in 1985, the median survival was only one year.[9] In a subsequent study report from MSKCC in 1992, the 5 year survival was only 17% for patients with more than 5cm tumour if the resection was incomplete.[2] The influence of the site of RAS on survival was evident in the Mayo clinic study. Even after excluding almost half the patients with unresectable disease, the 5 years survival was 27% for resected axial RAS in contrast to 68% seen in the peripheral sites.[8] This suggests a poor long term survival in patients with large RAS, especially in the axial skeleton where complete resection may not be possible. Chemotherapy now has an established role in the management of de novo osteogenic sarcoma, occurring mostly in children and young adults. However, its use for RAS in elderly patients is not defined. While most reports on RAS focus on the possibility of cure following resection, the quality of life and rehabilitation issues for the vast majority of patients with either unresectable or incompletely resected RAS have not been discussed. As found in the Mayo clinic study, 70% of the resectable patients required amputative surgery. Amputation of the lower extremity requires intensive rehabilitation for these amputees to adapt to their new life style. Such rehabilitation programme requires a multidisciplinary approach including foremost an appropriate, well fitting and comfortable lightweight prosthesis to produce an efficient gait and restore body image. To be able to adapt to the use the prosthesis, patients should be in good general health, have sufficient muscle power and well motivated.[10] This makes the task of rehabilitation difficult in patients with RAS as it often occurs in relatively older people who have survived their first cancer a decade ago and now may not be able to adapt and cope with a new life style. We had discussed with our patient that in all probability she would require major amputative surgery followed by rehabilitation and with this there was small but a definite chance of long term cure. After much deliberation, she declined surgery and instead opted for symptomatic and supportive care. It may be questioned whether it was appropriate on our part not to have persuaded her to undergo surgery or give chemotherapy or palliative reirradiation. Physicians sometime face this dilemma, when a patient refuses to undergo a morbid treatment that has only a small but definite chance of long term cure. While such dilemmas are not very uncommon in the practice of various disciplines of medicine, these issues are rarely discussed in research articles or textbooks or taught in the medical school. The lacunae in the available literature for such uncommon conditions make it more difficult for physicians to make a strong case for or against a morbid treatment. Unfortunately, some physicians do not see this as a dilemma and instinctively tend to influence these reluctant patients by using their persuasion, authority or projecting a more optimistic outcome. In retrospect it would appear that our concurrence with the decision taken by this informed patient was appropriate since she died of metastatic disease within 5 months. Major amputative surgery would have certainly hampered her quality of life without really changing the natural course of the disease. In conclusion, the management of RAS should be individualized taking into account the site of involvement, possibility of complete resection and the impact of surgery on the quality of life. These issues become more pertinent in the pelvic bone RAS of elderly patients, where resectability rates are low, rehabilitation difficult and long term survival poor. In the absence of evidence based treatment recommendation for such uncommon conditions, patient′s expectations and motivation to comply with an intensive rehabilitation programme should be an important determinant in the management decision. References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05013f1.jpg] |
| |||||||||

{kind=link}