 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 1, No. 2, April-June, 2005, pp. 103-107 Original Article Magnetic resonance imaging in carcinoma cervix- Does it have a prognostic relevance Sethi TejinderKataria, Bhalla NK, Jena AN, Rawat S, Oberoi R Department of Radiation Oncology, Rajiv Gandhi Cancer
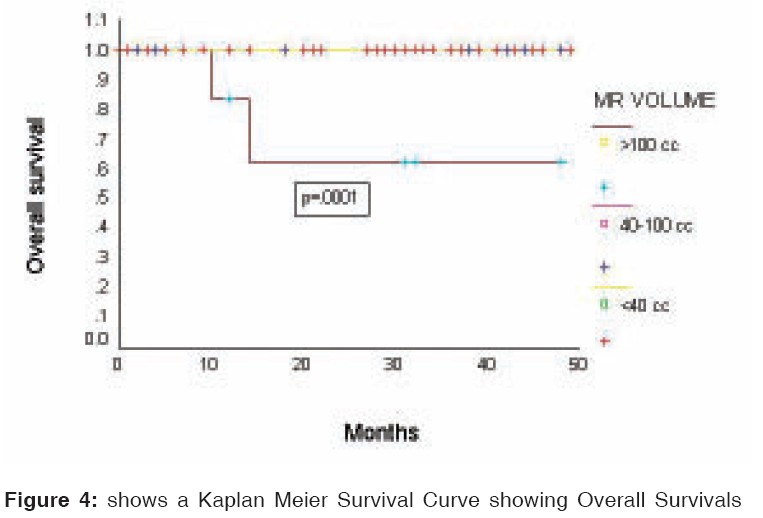
Institute and Research Centre, New Delhi Code Number: cr05021 Abstract PURPOSE: To evaluate the prognostic relevance of tumor size as determined on Magnetic Resonance Imaging (MRI) in cervical cancer.METHODS AND MATERIALS: A total of 70 consecutive patients were included in the study. 15 patients underwent surgery alone (Group A), 27 patients underwent surgery followed by adjuvant radiation (Group B), 14 patients underwent concomitant chemo radiation (Group C), and 14 patients underwent radical radiation alone (Group D). External radiation was delivered followed by intra cavitary brachytherapy. Serial MRI scans were performed in all patients before and after completion of treatment on a 1.0 Tesla MRI scanner. Patients were divided into three groups based upon MR volumes < 40 cc, 40-99 cc and > 100 cc. A correlation between MR volume, FIGO stage, disease free survival (DFS) and overall survival (OS) was done. Disease free and overall survivals were calculated using Kaplan Meier survival curves according to stage, MR volume and treatment protocol. RESULTS: In group I (MR volume < 40 cc), 44% of patients had stage I disease, 47% of patients with stage II and 9% patients had stage III disease. In group II (MR volume 40-99 cc), 35% patients had stage I, 45% had stage II disease and 10% had stage III and IV disease each. In group III (MR volume > 100 cc), 57% patients had stage II, 14% had stage III and 29% patients had stage IV disease. The DFS and OS did not achieve a level of statistical significance when evaluated as per protocol [DFS at p = 0.0685 and OS p = 0.3242], however a statistical significance was seen when DFS and OS were evaluated according to MR volumes [DFS, p = 0.0015 and OS, p = 0.0001]. CONCLUSION: In cervical cancer, the volume of disease as assessed on MRI may be a better prognostic indicator than FIGO staging and needs further evaluation. Keywords: M. R. I., Radiotherapy, Cervical carcinoma INTRODUCTION Carcinoma cervix is the most common cancer of females in the Indian subcontinent [1]. FIGO (International Federation of Gynecology and Obstetrics) staging system is the recommended staging procedure for these cancers. FIGO system allows clinical pelvic examination under anaesthesia and the stage is defined by the extent of disease spread beyond the cervix to the surrounding tissues including parametria, pelvic side walls, vagina, bladder or rectum. Chest x-ray is done to assess the lung metastasis and an intravenous pyelogram to assess hydronephrosis and thereby retroperitoneal lymph node disease. Pelvic lymphnode status and the tumour size is not evaluated to designate stages II - IV. The accuracy of such a clinical method depends largely upon the experience of the examining physician and leads to an intra- and interobserver variation in staging. CT and MRI are valuable imaging techniques in the pretreatment evaluation of cervical cancer allowing direct visualization of the tumour. MRI, however, can better delineate cervical tumour size, location and extension into adjacent structures and lymph node metastasis with its excellent soft-tissue contrast resolution and multiplanar scanning capabilities.[2] MRI provides accurate staging information in 70-90% of the cases.[3] Results of therapy for patients with carcinoma of uterine cervix are most often reported by clinical stage of the tumour. The pretreatment evaluation of prognostic factors helps in decision-making for treatment. Amongst the various prognostic factors, tumour size has emerged as the most important factor to which other morphological risk factors like tumour invasion depth, loco-regional extent and lymph node involvement are related.[3], [4], [5], [6] In patients treated by radical surgery or radiotherapy alone, size of the primary tumour is of prognostic significance irrespective of the clinical stage of the tumour.[7], [8] Recently, some studies have shown that tumour diameter/volume and pelvic lymph node status assessed by MRI significantly correlated with the outcome for patients with uterine cervical cancer treated with irradiation.[5], [6] We conducted a study to assess the prognostic significance of MRI mapped initial tumour volumes on local control in patients of carcinoma cervix treated by surgery alone, surgery with radiation, concurrent chemo-radiotherapy or radiotherapy alone. METHODS AND MATERIALS Patients MRI Protocol n Treatment interventions Follow up Statistics RESULTS The median age at presentation was 51 years (range 21-80 years) and the distribution according to FIGO stages was Stage I, 26 (37%); stage II, 35 (50%); stage III, 7 (10%) and stage IV 4 (5%). Histologically 68 patients had squamous cell carcinoma, one adeno carcinoma and one adeno squamous carcinoma. Based on the MR volumes patients were grouped into Group I (MR volume < 40cc), Group II (MR volume 40 - 100cc) and Group III (MR volume >100cc). Forty three (61.4%) patients were in group I, 20 (28.5%) in Group II and 7 (10%) in group III. In group I, 44% of patients had FIGO stage I disease, 47% had stage II disease and 9% had stage III disease. In group II, 35% patients had stage I, 45% had stage II disease and 10% had stage III and IV disease each. In group III, 57% patients had stage II disease, 14% had stage III and 29% had stage IV disease [Table - 1]. Disease free survival (DFS) and overall survivals (OS) were estimated according to MR volume, FIGO stage, and treatment protocol. According to MR volume the 3 year DFS was 86% in Group I, 87% in Group II and 33% in Group III respectively (p value = 0.0015) [Figure - 3]. 3 year OS was 100% in group I and II each and 62% in Group III respectively (p value = .0001) [Figure - 4]. According to FIGO staging the 3 year DFS was 96% in stage I, 78% in stage II, 63% in stage III and 33% in stage IV respectively (p value = .0094) and 3 year OS were 100% in stage I and II, 80% in stage III and 67% in stage IV respectively (p value = 0.0037). According to treatment protocol, the 3 year DFS for Group A was 92%, for Group B was 83%, for Group C was 92% and for Group D was 52% respectively (p value = .0685). 3 year OS for Group A and B were 100%, for Group C 92% and for Group D 86% respectively (p value = 0.3242). Thus, the disease free survival and overall survival did not achieve a level of statistical significance when evaluated as per protocol (p = .0685 for DFS and 0.3242 for OS), whereas a statistical significance was achieved when DFS and OS were evaluated according to MR volumes (p = 0.0015 for DFS & 0.0001 for OS) as compared to the conventional stage wise evaluation (p = 0.0094 for DFS & 0.0037 for OS). Twelve patients (17.14%) developed recurrence during the follow up, of these, 14% were in Group I, 10% in Group II and 57% in Group III. 5/12 had local recurrence and 7/12 distant metastases. Three patients underwent salvage surgery for local recurrence and one of them patient received salvage chemotherapy to achieve a complete response. Two patients received pelvic radiation and achieved complete response. Seven patients of these twelve patients developed distant metastases and were offered salvage chemotherapy. Two patients died 6 months after completion of RT (lung metastasis), and five patients refused further treatment. "58 patients were alive and on regular follow up every 3 months up to 2 years for a median of 28 months (range 24-36 months). Two patients were lost to follow up." Discussion Clinical pelvic examination is used to estimate primary tumour size and the extent of involvement in cervical cancer prior to treatment. Tumor size has been well established in numerous studies as an important independent predictor of response to radiation, local control and survival in cervical cancer.[7], [8], [9] Recent studies have shown that 3 dimensional quantitative imaging-based method of tumor size assessment using MRI is highly accurate in determining actual tumor size and extent of disease and may be superior to clinical palpation in predicting local tumor control.[3], [6], [10], [11], [12] With its multiplanar capability, distinctive tissue characteristics and exquisite anatomical detail, MRI has been reported to be superior to CT in the evaluation of pelvic anatomy and malignancies of the uterus. On MRI, cervical cancer appears as a high signal intensity mass on T2W (weighted) images, and can be distinguished from the normal low signal intensity cervical stroma.[13], [14] MRI differentiation between tumour and fibrosis can be achieved with high degree of accuracy. Furthermore, the strength of MRI is its ability to directly visualize the tumour therefore allowing measurement of its size. MRI is the most appropriate study for the evaluation of the post irradiation pelvis when searching for suspected residual tumours or recurrence of cervical carcinoma [11]. Typically fibrosis has low signal intensity on both T1W (weighted) and T2W (weighted) images. On the other hand tumour exhibits high signal intensity on T2W images. However, the inflammation and edema associated with acute radiation changes may also demonstrate high signal intensity on T2W (weighted) images, sometime leading to an incorrect diagnosis.[11] Our study indicates that FIGO staging may not be a true representation of the correct volume of disease and therefore, does not provide prognostic insight into the metastatic potential of the disease. Thus, a patient clinically assessed to have FIGO stage I disease may actually have a large volume [Figure - 1] and may require more aggressive treatment to achieve complete response and a patient with FIGO stage III disease may have small volume of disease [Figure - 2] and may actually have a better prognosis. Flueckiger et al. noted that all tumours regressed completely within 6 months of radiotherapy, showing a characteristic drop in relative signal intensity following radiotherapy. This decline was most precipitous during the first 3 months and was almost complete at 6 months.[10] This suggests that it is useful to obtain MRI 3 months after completion of treatment to evaluate the effect of radiation. Several prognostic factors including clinical evaluation (Patients age and Karnofsky Performance status), histological finding (tumour grade) and morphological features such as tumour size, location, depth of stromal invasion, local tumour extension and lymph node metastasis have been shown to affect the therapeutic outcome.[15], [16] In our study, the volume of disease as assessed on MRI was thought to be a better prognostic indicator than FIGO staging. MRI can better delineate cervical tumour size, location and extension into adjacent structures with its superior soft tissue definition and multiplanar scanning capacities.[17] Hricak, et al mentioned that tumor size and response to radiation showed a strong correlation.[6] In their report, a significant relationship was found between tumor size, disease stage and invasion to adjacent tissue and organs. However, in this report, the analysis was focused on tumor response with short follow-up, so survival influence was not mentioned. Mayr, et al also reported size and volume to be strong prognostic factors for local control.[5], [18] The three-dimensional tumor volume was calculated by the summation of all tumor areas and multiplication by the section profile. Using this volumetric technique, they reported that the volume regression rate during treatment would predict local control more accurately than the initial and residual volume. However, in another report,[18] DFS was influenced by both initial tumor size and follow-up examination, but not by regression rate. Toita, et al failed to show a significant influence for volume calculated in the same manner with DFS in their previous report, although tumor size was a significant prognostic factor for DFS.[15] This was chiefly because of their small patient numbers with a nonstage-limiting analysis. In our study the tumour volume was calculated in each case from T2W sagittal images using an in-house software that adds up the volumes for each slice from user marked area on the visualized tumour and taking care of the area due to inter slice gap through interpolation. Our overall patient numbers are not high enough at this time to allow assessment of tumor volume parameter with respect to other prognostic variables. Our data will need further evaluation with larger number of patients. Conclusion The clinical assessment and FIGO staging is not enough to assess the magnitude of disease. Pretreatment MRI determines the actual tumor size, local tumor extension, depth of stromal invasion and lymph node metastasis with its superior soft tissue definition and multiplanar scanning capacities and has been shown to affect the therapeutic outcome. Thus, a patient clinically evaluated to be in an early stage may actually have a worse prognosis due to large volume of disease as seen on MRI and may be optimized for an aggressive treatment plan. The correlation between MR volume, FIGO stage and survivals (disease free and overall survival) suggests that MRI gives a better indication of the volume of disease than FIGO stage. Volumetric study using MRI is thought to be clinically efficacious to estimate clinical results, and we believe this criterion can be meaningfully adapted for its use in better understanding of prognosis and devise an optimal treatment strategy. We also believe that MRI should be included as a routine investigation for staging in the FIGO staging system. References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05021f3.jpg] [cr05021f4.jpg] [cr05021t1.jpg] [cr05021f1.jpg] [cr05021f2.jpg] |
| |||||||||

![[Table - 1]](/showimage?cr/photo/cr05021t1.jpg){kind=link}
![[Figure - 3]](/showimage?cr/photo/cr05021f3.jpg){kind=link}
{kind=link}
![[Figure - 1]](/showimage?cr/photo/cr05021f1.jpg){kind=link}
![[Figure - 2]](/showimage?cr/photo/cr05021f2.jpg){kind=link}