 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
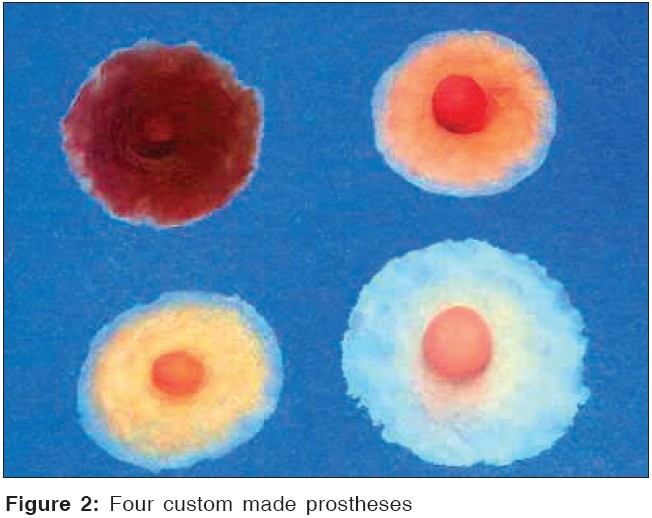
Journal of Cancer Research and Therapeutics, Vol. 1, No. 2, April-June, 2005, pp. 111-113 Brief Communications Custom-made nipple prosthesis: A long-term satisfaction survey Janes Simon Department of surgery, New Cross hospital, Wolverhampton, WV10 0QP Code Number: cr05023 Abstract BACKGROUND: Nipple-areola reconstruction or prosthesis completes the process of breast reconstruction. Although custom made nipple prosthesis (CNP) have been used for almost 10 years, little follow-up data on patient satisfaction is available. We assessed long-term patient satisfaction with CNP. Keywords: Custom nipple prosthesis, Survey, Breast reconstruction Introduction The psychological value of breast reconstruction following mastectomy is well documented, encompassing diminished anxiety[1] and enhanced body image.[2] Nipple-areola reconstruction (NAR) or prosthesis completes this process of breast reconstruction. However, surgical NAR techniques have variable long-term results[3]: up to 11% experience flap necrosis, and one-third of patients require further corrective surgery.[4] Other long-term complications include loss of colour and projection, in addition to scarring at the donor site with some techniques. Mass produced prosthesis were used as an early alternative to surgical NAR, but commercially available nipple prostheses have a uniform appearance, and are produced with little anatomical detail or colour variation [Figure - 1]. In contrast, a custom-made nipple prosthesis (CNP) reproduces the natural skin texture, and can match the size, shape and colour of the original nipple.[3] This approach is thought to provide a more psychologically and cosmetically acceptable prosthesis. Although CNP has been used for almost 10 years, no follow-up data on patient satisfaction is available. We aimed to assess long-term patient satisfaction of our breast cancer patients who underwent CNP. [Figure 2] Materials and Methods Production of a custom made prosthesis Survey Results Of 52 patients who had CNP following breast reconstruction, 29 responded to the questionnaire (56% response rate), median age 56.1 years (IQR 52-61 years). The median time since CNP was 2 years (IQR 0.9-3 years), and 67% felt they had benefited from the prosthesis. 39% wore their CNP regularly, for a median of 8 hours per day (IQR 2-13 hours). The most commonly used method for securing the prosthesis to the skin was Vaseline (11 patients, 38%), two patients used adhesive (7%) and three patients used both Vaseline and adhesive (10%). Most patients were highly satisfied with CNP size, colour and projection, median score 5 (IQR 4-5) for each variable. Comments on CNP were generally positive, and suggested improved psychosocial confidence including: "it made me feel complete"; "it made me feel like a woman"; three women said it allowed them to enjoy swimming again, another felt able to wear a bikini for the first time in 18 months. Only two patients reported problems maintaining suction with the CNP, and another was unable to use the prosthesis because of a skin reaction to the silicone. Patients who were satisfied with their CNP (median age 52.9 years, IQR 45.3-59.2 years), were significantly younger than those who were not satisfied with their CNP (median age 59 years, IQR 54.7-62 years), p = 0.031, Z = -2.16. In addition, patients who had their CNP for less than 3 years were more likely to be satisfied with CNP than those with CNP for = 3 years, 60% vs 18%, p = 0.04. Three patients had subsequent nipple reconstruction, a further 7 (24%) wanted nipple reconstruction. Finally, all respondents thought CNP should be offered at the time of initial surgery. Discussion In this first follow up survey of CNP satisfaction, we have found most patients are highly satisfied with CNP, with highest satisfaction in the first 3 years of CNP use. Patients satisfied with their CNP also tended to be younger, which may be due to enhanced perception of body image in younger women.[2] Our findings are consistent with a previous study that compared characteristics of women who did or did not chose surgical NAR following mastectomy, which found that women choosing NAR were younger and more satisfied with the final result than those who chose not to undergo surgical NAR.[5] It was interesting to note that one-quarter of patients wanted surgical NAR. This, together with the fact that CNP satisfaction was lower after three years of use, suggests it may be worthwhile offering surgical NAR after this time has elapsed. CNP is a quick and inexpensive alternative to surgical nipple reconstruction, with considerable shape and colour advantages over the commercially available varieties [Figure - 1]. The whole process takes 2-3 hours, and can be performed by any maxillofacial laboratory on an outpatient basis. This offers substantial cost benefits in comparison to surgical reconstruction, which involves both theatre and inpatient time. Our results suggest CNP should be more widely available, and offered alongside reconstruction at the time of initial breast cancer surgery if nipple loss is anticipated. References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05023f1.jpg] [cr05023f2.jpg] |
| |||||||||

![[Figure - 1]](/showimage?cr/photo/cr05023f1.jpg){kind=link}
{kind=link}