 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
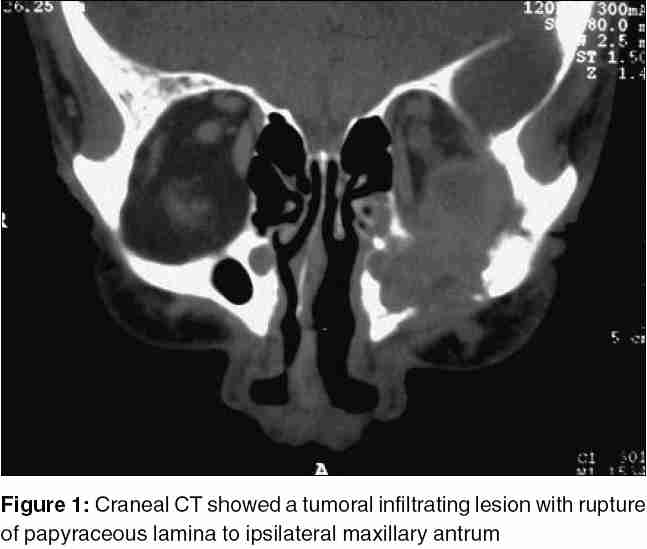
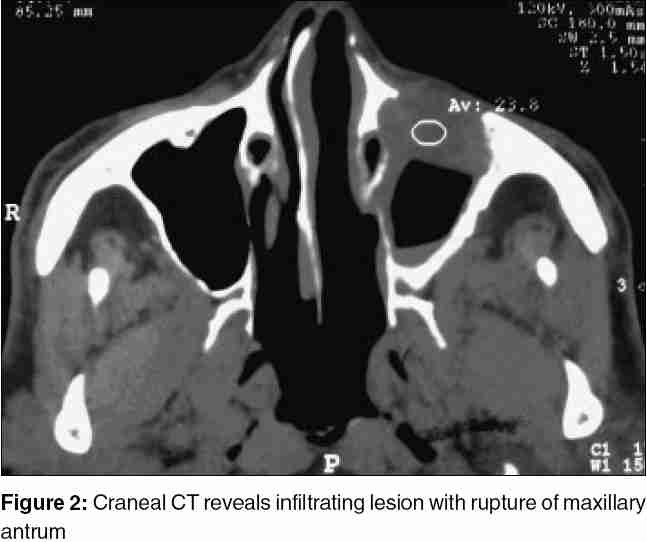
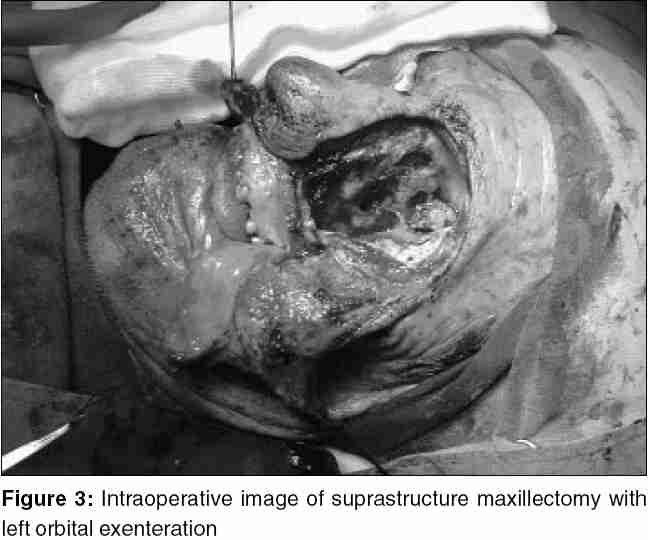
Journal of Cancer Research and Therapeutics, Vol. 1, No. 3, July-September, 2005, pp. 132-135 Review Articles Supraestructure maxillectomy and orbital exenteration for treatment of basal cell carcinoma of inferior eyelid: Case report and review. Villalón-López José Sebastián, Valle-Mejía Carlos Arturo, Patiño-Lara Antonio, Moreno-Pérez Bertha Alicia, Muñoz-López Jorge Alejo, Alcantar-Andrade Antonio Surgical Oncology Department, Hospital de Especialidades Centro Médico Nacional de León, Gto., Instituto Mexicano del Seguro Social, Colonia los Paraísos, León, Gto., México. Code Number: cr05031 Abstract Basal cell carcinoma (BCC) is the most frequent type of skin cancer in humans, with cumulative exposure to ultraviolet radiation (UVR) as important risk factor for development of the illness as such as severe solar burns during childhood or adolescence. BCC is mainly located on sun exposed sites, being head and neck the areas of more incidence; although nose, eyelids and periorbitary tissue are unfavorable due to cosmetic results that BCC involves. Tumors can be classified as: nodular, superficial, micronodular, morphea variety, infiltrating, pigmented, metatypic and fibroepithelioma of Pinkus. Several treatment options as surgical and non-surgical are available. The goal of treatment is complete excision of the tumor with preservation of surrounding structures in a way aesthetically acceptable. Mohs' micrographic surgery is the standard treatment for all non-melanoma skin cancer. Orbital exenteration is also used for treatment of malignancies of ocular tissues, mainly squamous cell carcinoma, sebaceous cell carcinoma and BCC. The tissue beneath the surgical site can be left for second-intention granulation or covered with a cutaneous implant of partial thickness. The case of a 77 year-old patient is presented with BCC of inferior eyelid of 14 years duration, formerly managed with radiotherapy and, due to recurrent illness and invasion to the maxillary antrum; he needed supraestructure maxillectomy with left orbital exenteration. Keywords: Basal Cell Carcinoma, Orbital Exenteration, Supraestructure Maxillectomy CASE REPORT A 77-year-old man was seen in the clinic with a positive history of smoking and drinking habits. 14 years earlier, this patient initially noticed a raised maculate papule, becoming slowly as an evident tumor in his left inferior eyelid, occasionally hemorrhagic. The patient was treated with some topical treatments without a response. This lesion turned onto an infiltrating ulcer from the eyelid to ocular globe. A biopsy from the lesion was taken with histopathology report of an infiltrating basal cell carcinoma. Due to the extension of this lesion, the patient received radiotherapy with a dose of 60Gy, fractioned on 30 sessions and with an increase of 10Gy. Later on, patient was followed without evidence of tumoral activity for 8 months, but a relapse has detected by the presence of a raised, ulcerated hemorrhagic lesion on malar region which was analyzed by biopsy with a histopathology report of keratolytic basal cell carcinoma with dermis infiltration. Cranial tomography showed a tumoral infiltrating lesion with destruction of orbital inferior wall [Figure - 1], and infiltration from papyraceous lamina to ipsilateral maxillary antrum [Figure - 2]. A suprastructure maxillectomy with left orbital exenteration was performed without complications [Figure - 3]. Surgical histopathology report showed free of tumor surgical margins. Final histopathology report showed a keratolytic basal cell carcinoma, 3cm width, with bone and soft tissues infiltrated, perineural permeation and desmoplasic fibrosis, tumoral necrosis and plurifocal superficial mucosal infiltration of the maxillary antrum, ptisis bulbi [Figure - 4]. 8 Months after the procedure, patient still alive and remained without symptoms of tumoral activity. DISCUSSION Basal cell carcinoma (BCC) is the most frequent type of skin cancer in humans,[1],[2] with almost 90,000 new cases diagnosed in US every year, with cumulative exposure to ultraviolet radiation (UVR) as important risk factor for development of the illness as such as severe solar burns during childhood or adolescence, although other factor have been named such as type 1 and 2 Fritzpatrick′s skin, red-haired people, childhood freckles, familiar history of skin cancer and less common in AIDS and transplanted patients.[2]In a case series of 703 eyelid malignant tumors treated by Oncology Service in the National Medical Center "Siglo XXI" of the Mexican Social Security Institute from 1986 to 2000, 596 (84.7%) were classified as BCC[3]. BCC is mainly located on sun exposed sites, being head and neck the areas of more incidence; although nose, eyelids and periorbitary tissue are unfavorable due to cosmetic results that BCC involves.[1], [2], [3], [4] Histological types of BCC has been associated with different results and prognosis. Tumours can be classified as: nodular, superficial, micronodular, morpheic variety, infiltrating, pigmented, metatypic and fibroepithelioma of Pinkus.[5] Nodular variant is the most frequent form of BCC, addressing more than 50% of lesions, being superficial or ulcerated and often is visualized on actinic damaged skin; this lesion often shows a slow growth and is best-known as Jacobi′s ulcer or ulcus rodens . Superficial BCC appears as a plaque or as an erythematous squamous papule often found on the trunk, arms and legs; and occasionally seen in sunlight-exposed areas such as head and neck. Micronodular variant presents as firm plaques not well defined indurated related to an increase in relapse of the tumor. Morpheic variety (also known as sclerotic, fibroid or desmoplasic) occurs in more than 50% of all BCC. Tends to be more aggressive, sometimes infiltrating deeper in muscle or fat tissue. Clinically resembles a scar or a little patch. There are no preferential sites of location and these lesions rarely bleed or get ulcerated. Infiltrating type of BCC is linked to morpheic or nodular variants. Pigmented type is often seen in black-skin people and even is wrong classified as a melanoma, seborreic keratoses or melanocytic benign nevus. Metatypic BCC shows clinical signs of BCC and squamous cell carcinoma (SCC) as well, tends to be more aggressive than other BCC forms and it could grow and extend as SCC does, with a great presence of metastasis. Fibroepithelioma of Pinkus, described by Hermann Pinkus Szuchmacher in 1953, often appears in lumbar area and resembles a fibroepithelial polypus or seborreic keratoses.[2],[3],[5],[9] Several treatment options such as surgical and non-surgical, are available.[2],[7],[8] The goal of treatment is complete excision of the tumor with preservation of surrounding structures in a way aesthetically acceptable[7]. Mohs′ micrographic surgery (MMS) is the standard treatment for all non-melanoma skin cancer.[7],[8],[9],[10],[11] Topical chemotherapy agents such as 5-Fluoruracil (5-FU) has been used for treatment of in situ and superficially extended BCC and SCC. The major value of this type of chemotherapy is for actinic keratoses. Other chemotherapy drugs used in BCC and SCC treatment with limited results are methotrexate, 5-mercaptouracil, nitrogened mustard, actinomycin D, intravenous cisplatin or intralesional bleomycin.[7],[8] Agent Imiquimod (AldaraÒ) is a synthetic immune system response modifier, and applied locally, has been shown a very good response in BCC treatment, more often in superficial lesions and tumors from 0.5 to 2.0 cm2 width, excluding those tumors with faster growth or face H-zone tumors.[7],[8],[12] Some vitamin-A derived retinoid such as topic isotretinoin has proved effectiveness in decrease of solar keratoses and could help in the prevention of cancer progression. Intralesional injection of Interferon (IFN), specially 2-a and 2-b, show positive effects in BCC and SCC treatment, due to malignant cell growth inhibition via immune cell response stimulation. Cyclo-oxygenase-2 (COX-2) overexposure has been related with some neoplasm such as colon and mammary cancer as well as skin tumors. COX-2 inhibitors, particularly celecoxib, have a therapeutic role in skin cancer chemoprevention, although further placebo-controlled randomized trials are needed in order to conclude this issue.[7],[8] In a clinical trial by Kwan et al,[9] from a sixty-one sample of patients with BCC diagnosis and treated with radiotherapy, a 4-year local disease control was achieved in 86%, finding no evidence of factors affecting locoregional control. Median-time of relapse was 40.5 months and relapses were locally situated in all cases. The 8 cases of relapse, 4 were rescued with surgery; 2 more received a new radiotherapy course and one patient rejected treatment. None of the patients developed distance metastasis and no one died by this cancer. Similar results were obtained by Seegenschmiedt et al in 99 patients with 127 BCC lesions situated on head and neck areas treated with radiotherapy, using orthovoltage equipment, with a 36 ± 21 months following. Complete improvement from tumor was achieved by month 3 after the treatment in 99% of the cases. Cosmetic results ranged from good to excellent in 98% and just 2 cases developed local relapse at 6 and 20 months after radiotherapy.[10] In a trial conducted by Malhotra et al, 1295 patients were treated with MMC, finding nodulocystic (39.5%) and infiltrating (34.8%) as the main histological variants. Also, they found as the most common periocular area the medial edge (48.4%), lower eyelid (47.6%) and superior eyelid (3.9%). 32% of the tumors (415/1289), were recurrent BCC′s and just 1% (n=12) of the cases exhibited perineural invasion.[11] In other study from the same authors, 819 patients with periocular BCC treated with MMC showed a relapse index of 2% (7/346), being the principal relapse factors previous relapse, infiltrating (n=5) and superficial (n=2) variants and female gender (6/7). Principal anatomic sites of relapse were medial edge (n=5) and inferior eyelid (n=2).[12] Orbital exenteration is used for treatment of malignancies of ocular tissues, mainly SCC, sebaceous cell carcinoma and basal cell carcinoma. Other tumors treated by this mean are melanoma, cystic adenoid carcinoma and uveal carcinoma with extra scleral invasion. The tissue beneath the surgical site can be left for second-intention granulation or covered with a cutaneous implant of partial thickness.[15] In a case-series of 34 patients undergoing orbital excision, Simon found 26.5% (n=9) of SCC cases, 17.6% (n=6) of BCC and 14.7% (n=5) of conjunctival, orbital and eyelid melanoma as histological diagnosis before surgery. Less frequent histological diagnosis were choroid melanoma, sebaceous cell carcinoma, cystic adenoid carcinoma, osteosarcoma, benign mixed tumors, adenocarcinoma and mucormycosis. In 7 cases (20.6%) an extended procedure was needed, including maxillectomy, etmoidectomy or zigomatic bone resection. Only in 4 patients (11.8%) undergoing subtotal exenteration, a patch covering postsurgical defect was not needed.[15] References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05031f4.jpg] [cr05031f2.jpg] [cr05031f1.jpg] [cr05031f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}