 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 1, No. 3, July-September, 2005, pp. 136-141 Original Article The optimal use of granulocyte macrophage colony stimulating factor in radiation induced mucositis in head and neck squamous cell carcinoma. Patni Nidhi, Patni Sanjeev, Bapna Ajay Department of radiation, surgical and medical oncology, Bhagwan Mahaveer Cancer Hospital Code Number: cr05032 Abstract Objective: Evaluation of response of granulocyte macrophage colony stimulating factor (GM-CSF) on acute radiation toxicity profile in head and neck squamous cell carcinoma.Methods and Materials: Thirty three patients with proven stage I or II head & neck carcinoma received conventional external beam radiation therapy. Out of these, six patients received postoperative adjuvant therapy while remaining 27 received definitive RT. Patients were given 100 mcg GM-CSF subcutaneously per day along with radiation after they developed grade 2 mucositis and /or grade 2 dysphagia and / or complained of moderate pain. GM-CSF was administered till there was a subjective relief or objective response. Patients were evaluated for oral ulceration, swallowing status, pain and weight loss. Response to the treatment and patient outcome was assessed. Results: There was a decreased severity of mucositis and dysphagia in the evaluated patients. None of the patients suffered severe pain or required opioids. The mean weight loss was only 1.94%. Minimal side effects were experienced with GM-CSF. Conclusions: GM-CSF reduces the severity of acute side effects of radiation therapy thereby allowing completion of the treatment without interruption. Its remarkable response needs to be evaluated further in large randomized trials. The time of initiation and cessation of GM-CSF during radiation therapy and the required dose needs to be established. Keywords: GM-CSF, Head and neck carcinoma, Radiation mucositis, Acute toxicity INTRODUCTION Head and neck cancers constitute a major oncological problem in the Indian population. These cancers top the list in sitewise distribution. There were 25.1% registered Head and Neck cancer cases in a hospital based cancer registry in 1998. Its frequency was no different from those seen over the years 1984-98 i.e. 27%.[1] Radiation therapy remains the mainstay of treatment in the management of head and neck cancers. It is offered to nearly 75% of all head and neck cancers with either curative or palliative intent, alone or as a part of multimodality approach.[2] Oropharyngeal mucositis is a frequent side effect of radiotherapy for head and neck cancer.[3] It represents an important clinical problem as there is associated severe pain, the need for parenteral nutrition, risk of mucosal infection and subsequent septicemia.[4] By 20-30 Gy, with standard fractionation delivered at 1.8 to 2.0 Gy/day, reddening of mucosa becomes evident. After an additional 10 to 20 Gy, small white areas of pseudomembrane begin to appear. In their early development, these patches tend to be scattered throughout the treatment field. As the treatment continues, the patches begin to coalesce, leading to confluent mucositis.[5] Acute mucositis is the result of hypoplasia of squamous epithelium due to sterilization of mucosal stem cells and inhibition of proliferation of transit cells.[6] Evidence has emerged to suggest that mucositis develops as a series of dynamic interactions that begin in the epithelium but then progress to involve other tissue components. Sonis et al have proposed that this process can be thought of as occuring in five stages or phases:initiation, message generation, signal amplification, ulceration, and healing.[7] The initiation phase involves direct damage to DNA and other cellular components that occurs immediately following exposure to radiation or chemotherapy. These treatments generate reactive oxygen species (ROS), free radicals that can cause DNA strand breaks in the epithelium and submucosa and initiate a cascade of other down stream biological events. In the next stage-upregulation and message generation -transcription factors are activated that affect a number of genes controlling protein synthesis and cell signaling. Signal amplification, the third stage, consists of feedback loops that further increase the number and level of activating signals. Pro inflammatory cytokines, such as tumor necrosis factor alpha (TNF-α), which are secreted following radiation or chemotherapy damage, not only directly result in tissue injury but also further increase the activity of other signaling factors such as NF-kBand mitogen activated protein kinase (MAPK).[8] The net result is an ongoing cycle of amplification of injury that persists well after the initial insult of radiation therapy or chemotherapy. Interestingly, despite all these cellular changes occurring during the initial stages of mucositis, few symptoms are apparent. The fourth stage, ulceration, involves penetration through the epithelium into the submucosa. The ulcerated surface can then be colonized by oral bacteria, producing toxins and additional inflammatory cytokines (from activated macrophages) and angiogenic factors. This ulcerative phase is primarily responsible for the main clinical symptoms of mucositis (pain, inflammation, and loss of function) and is associated with higher costs (increased drug use and hospitalization). The final stage in the pathobiology of mucositis is healing, Epithelial cells, under control of signals secreted by the extracellular matrix, migrate, grow and differentiate to form a wound. These signals are then downregulated to avoid hyperplasia. With the healing process under way, symptoms begin to abate. Severe mucositis may lead to interruption of planned course of radiotherapy. Prolongation of overall time of radiation has an adverse effect on radiocurability of head and neck squamous cell carcinoma.[9],[10],[11] Throughout the last two decades there have been many attempts to identify remedies to prevent or at least ameliorate symptoms of oral mucositis,[12] but none has resulted in satisfactory outcome. Granulocyte-macrophage colony stimulating factor (GM-CSF) has been shown to enhance a number of cellular functions which are essential for wound healing, including activation of neutrophils,monocytes and macrophages, migration of epithelial cells, proliferation of keratinocytes and modulation of fibroblast phenotype.[13],[14],[15] The role of cytokines, like GM-CSF, has been investigated for mucosal protection during cytotoxic chemotherapy also.[16],[17] Administration of IL-1 during fractionated radiotherapy in C3H/K mice showed protection of lip mucosa and tongue from acute radiation reaction.[18],[19] A pilot study showed that GM-CSF administration concurrently with conventional fractionated radiotherapy was feasible without significant toxicity. It showed that the acute side effects of radiotherapy namely mucositis, pain and functional impairment were nil to minimal in head and neck cancers.[20] Also, clinical studies of GM-CSF have found no stimulation of tumor growth.[21] Based on these experiences, we planned to carry out a study to further explore the role of GM-CSF in radiation mucositis in head and neck cancers at our centre. PATIENTS AND METHODS Eligibility Criteria Characteristics of the Patients Thirty three patients were treated with definitive or postoperative adjuvant radiation therapy from Jan 2000 to Dec.2002. There were 8 female and 25 male patients. The median age was 50 years (range 21 to 70 years). According to AJCC staging 9 patients had stage I and 24 had stage II malignancy. Twenty nine patients were found to use tobacco.
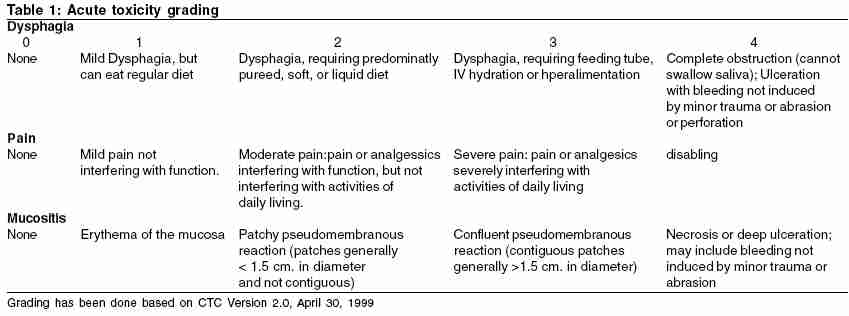
Patients received external beam radiation with two parallel opposed fields using telecobalt gamma rays at 80 cms SSD. Twenty seven patients were treated definitively with teletherapy and six received postoperative adjuvant external beam radiation. The average dose delivered to patients in radical group was 66.7Gy and in adjuvant group was 57.2Gy in conventional fractionation. The patients were treated with shrinking fields after 40Gy and mucositis was analysed all the time in the reduced field of treatment. They received 50 Gy to the whole field, though the spinal cord was shielded at 40 Gy. The treatment volume was then reduced and dose was escalated.The mean field size was 110.9 cm2. None of the patients received concurrent chemotherapy. All patients underwent dental prophylaxis in the form of scaling and fluoride application. Dental cavity filling and extraction were done, where indicated, prior to radiation therapy. Those using artificial dentures were advised not to wear the same during the treatment. Patients were instructed to maintain strict oral hygiene using a soft baby toothbrush and flouride toothpaste. They were counselled against using mouthwashes containing phenol or alchohol, tobacco, alcoholic beverages, very hot and cold food and spicy food. No intraoral tumor ablative procedures, altering the mucosal surfaces, were performed on the subjects. None of the patients had intercurrent ailments or preexisting pathologies that affected mucosal integrity. None of the patients had gap in radiation therapy. Same examiner graded all mucosal reactions, pain and functional impairement. All the patients were treated according to the ethical guidelines followed routinely in the hospital. Administration of GM-CSF The patients were given Injection GM-CSF (Leucomax ®) 100 mcg subcutaneously per day after reconstitution. The sites of injection were rotated. The drug was started when one of the following criteria was observed. a) Patchy fibrinous mucositis. GM-CSF was given for six consecutive days, excluding the days, when radiation was not delivered. When the above signs and symptoms persisted, its administration was prolonged till there was a subjective or objective response. Subjective response was assessed by scoring dysphagia and pain. Grading of mucositis was done based on the objective response. Dysphagia, pain and mucositis were graded according to CTC version 2.0 [Table - 1]. The mean total dose delivered to the patients was 731.2 mcg (20 patients received 600 mcg, 10 patients received 900 mcg and 2 patients received 1200 mcg). Weekly evaluation was done to assess mucosal reaction, pain and dysphagia. RESULTS Acute Toxicity Profile During Radiation Therapy Functional Impairment In the third week of radiation therapy 63.63 % & 36.36% patients developed grade 1 and grade 2 mucositis respectively. It improved with the administration of GM-CSF, as is evident [Table - 3]. Confluent mucositis was seen in three and four patients in the fourth and fifth week of treatment respectively. One patient developed oral candidiasis. She responded to 20 days′ course of oral fluconazole. Pain Weight Response Assessment and Survival on Completion of Radiation Therapy The response was not assessable in 18.1% (6) patients who received postoperative adjuvant radiation therapy. Complete response was seen in 88.88% (24/27) patients who received definitive RT. Twenty eight patients were clinically controlled till May 2003, one patient had progressive disease and died 7 months after completion of radiation, three patients recurred locally, and one patient died of an unrelated cause 13 months after the treatment. Side effects of GM-CSF The side effects of the drug were minimal. Two patients (6%) complained of itching and developed erythema at the site of injection which responded to oral antihistaminics. Discussion Oral mucositis continues to afflict all the patients who receive radiation therapy. Till date, there is not a single agent that is considered to be "gold standard" to prevent or treat oral mucositis.[22] A review published by Andy Trotti et al[23] confirms the high incidence (97%) of mucositis in patients receiving RT in analyses of 33 studies (n = 6181 patients). The rates of grade 3 mucositis was higher in RT altered fractionation (65%) than in RT conventional group (49%), as was the rate of grade 4 mucositis (17 v/s 5%, respectively). RTOG has recently reported severe mucositis in 25% in conventional RT group and 41-47% in accelerated fractionation group.[24] Because of more rapid cellular turnover in mucosa it exhibits the radiation induced damage rapidly.[5] Al-Tikriti et al reported mucosal plaque formation and ulceration in most patients at 3 to 4 weeks after initiation of radiotherapy.[25] EORTC randomized trial of conventional and hyperfractionated radiotherapy in oropharyngeal carcinoma observed 42% grade II and 49% grade III mucositis in 2 Gy fractionation arm.[26] GM-CSF protects neutrophil from apoptosis and prolongs its half -life.[27] It also protects capillary endothelial cells from radiation induced apoptosis.[28] Mammalian cells respond to oxidative stress of radiation by activating genes that encode GM-CSF and Interleukin -1.[29] Secretion of Interleukin -1 is observed at the inflammatory site by the colony stimulating factor.[21] Our trial suggests mucosal protection in all the patients as none of the patients suffered grade IV mucositis inspite of delivering 66.7Gy median dose to 110.9 cm2 tissue. Grade III mucositis was experienced by 9.09% and 12.12 % patients in the forth and fifth week respectively. It was observed that besides mucosal healing, GM-CSF also protects the mucosa from further radiation induced damage as the drug was discontinued during radiation once the patient showed symptomatic and subjective improvement. The patients were able to complete the planned radiation therapy without any interruption. Since the incidence and severity of mucositis was less in our study, there was a decreased incidence of oral pain. The overall incidence of dysphagia was decreased, which resulted in 1.94% mean weight loss. Minimal side effects of the drug were observed in our study. Since the patients were already on NSAIDS, they did not suffer from flu like symptoms. In the literature the quantity of drug used in a patient ranges from 1 to 5 mcg/kg./ day for the complete duration of radiation in I/V, S/C or topical form.[20],[30],[31],[32],[33],[34] In different studies drug was initiated at different days ranging from day 1 to day 11 of radiation therapy [Table - 5]. Large amount of GM-CSF has been used in the above studies and the cost involved has been discussed with concern. In our study we have administered GM-CSF when the patient became symptomatic and / or started developing fibrinous mucositis and not from the beginning or after 20 Gy. In our opinion since the drug is expensive, route of administration is invasive and it has a toxicity profile, though low, it should be used judiciously and in smallest possible dose which benefits the patient. CONCLUSIONS GM-CSF is able to provide subjective response within 24 hours and objective response in less than a week. There is therefore, no need to give it in asymptomatic patients. Larger double blind randomized trials are recommended to find out the optimum dose and timing of initiating and stopping the drug during RT.References
Copyright 2005 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr05032t5.jpg] [cr05032t3.jpg] [cr05032t2.jpg] [cr05032t1.jpg] [cr05032t4.jpg] |
| |||||||||


{kind=link}
![[Table - 5]](/showimage?cr/photo/cr05032t5.jpg){kind=link}