 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
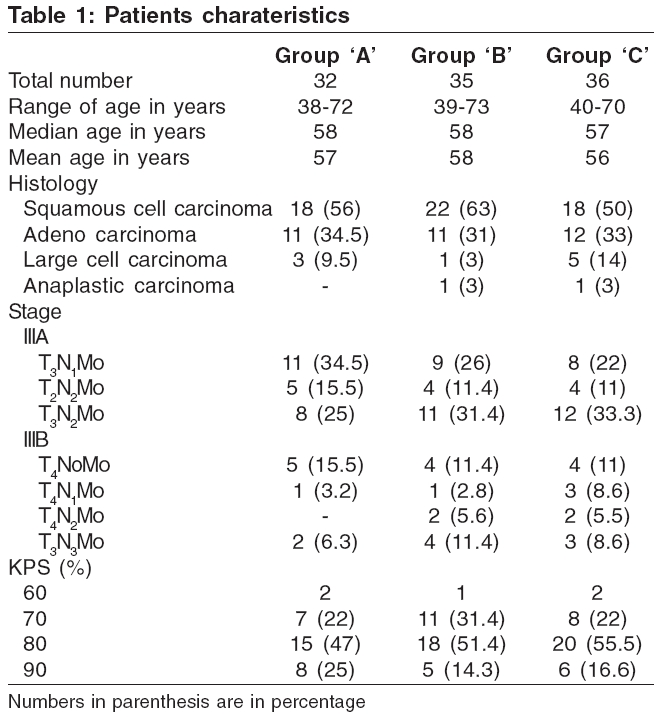
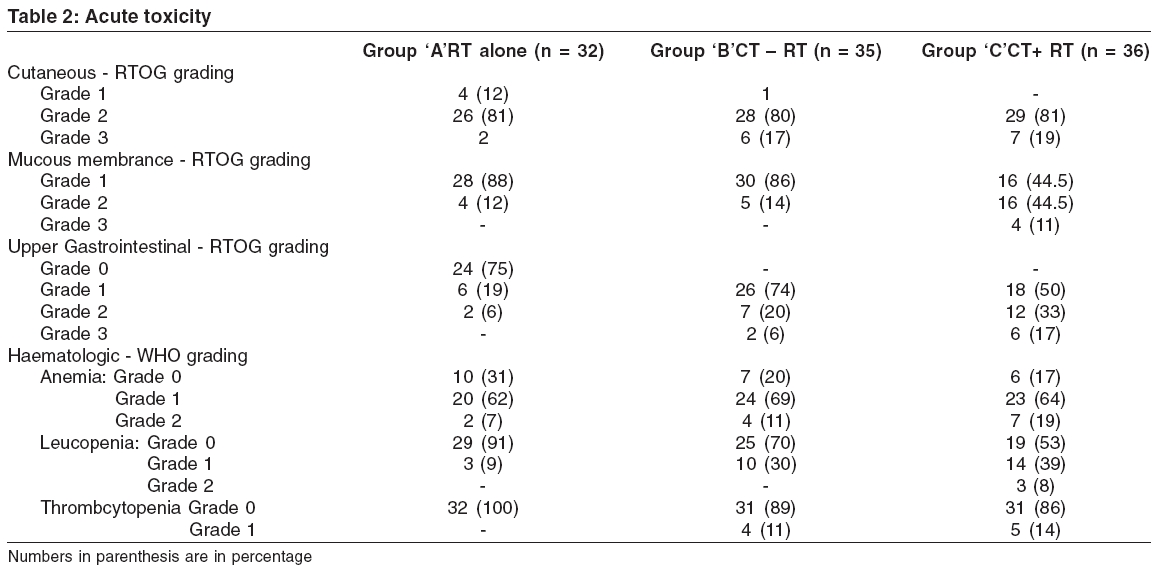
Journal of Cancer Research and Therapeutics, Vol. 2, No. 2, April-June, 2006, pp. 47-51 Original Article A prospective and randomized study of radiotherapy, sequential chemotherapy radiotherapy and concomitant chemo therapy-radiotherapy in unresectable non small cell carcinoma of the lung Dasgupta Anirban, Dasgupta Chandan, Basu Siddhartha, Majumdar Anup Department of Radiotherapy, Institute of Post Graduate Medical Education and Research, Kolkata Code Number: cr06011 Abstract Purpose: Treatment of advanced Non small cell lung cancer (NSCLC) often produces dismal results. Combination of available treatment modalities has reportedly improved the outcome. A prospectively randomized trial was conducted, comparing combined treatment modalities versus radiotherapy alone, in treatment of unresectable NSCLC.Materials and Methods: A total of 103 patients were randomized to three groups. In group 'A', 32 patients received radiotherapy alone (6500 cGy/30 fraction). In group 'B', 35 patients received neoadjuvant chemotherapy (Cisplatin 80 mg/m2 on day 1 and Etoposide 100 mg/m day 1-3 intravenously q3 weeks for 3 cycles), followed by radiotherapy (6000 cGy/30 fractions) and 3 more cycles of Chemotherapy, with the same regimen. In group 'C', 36 patients received radiotherapy (5000 cGy/25 fractions) with concurrent chemotherapy (ciplatin 20 mg/m2 + Etoposide 75 mg/m2 intravenously on day 1-5 and day 22-26), followed by 2 more cycles of chemotherapy,q3 weeks with the same regimen. Results: Initial treatment responses were significantly higher in group 'B' ( P <0.05) and 'C' ( P <0.03), compared to group 'A'. Follow- up observations showed, that addition of chemotherapy brought down distant metastasis's from 62.5% (group 'A') to 48.6% (group 'B') and 44.4% (group 'C'). The median time to tumour progression also improved from 16 months (Group 'A') to 21 months (Group 'B' and 'C'). But 2 year follow up did not show any survival benefit. Acute toxicities were more frequent in group 'B' and 'C', but were manageable. Conclusion: Addition of chemotherapy with radiation in unresectable NSCLC improves response rates, time to tumour progression and disease free survival, though the same effect is not translated in overall survival. Keywords: Non small cell lung cancer, neoadjuvant, concurrent response, disease free survival, metastasis, acute toxicities. Introduction Lung Cancer is one of the most commonly occurring malignancy and the leading cause of cancer related death, worldwide. Non-small cell Lung Cancer (NSCLC) constitutes about more than 80% of all lung cancer cases. Historically, surgery has provided the best chance of cure in resectable (NSCLC). But only 15% of NSCLC patients present with localized disease, the rest have either lymph node metastasis (25%) or distant metastasis (65%), at the time of diagnosis.[1] In early stage (Stage I & II), when the disease has not extended beyond the bronchopulmonary lymph nodes, a complete excision is almost always possible. Whereas in advanced stage (Stage III), the treatment often produced dismal results, in spite of much progression in the field of multimodality therapy. Involvement of bronchopulmonary nodes [N 1 ] in large primary (T3 disease) makes survival poor, even after complete excision (Five year survival rate is 20%). When mediastinal lymph nodes are involved [N 2 disease on wards], survival is even poorer in any stage of primary tumour, with surgery alone.[2] Therefore combined modality treatments have been tried in advanced stages [N 2 disease onwards] of NSCLC, with an expectation of some survival advantage. Surgery, radiotherapy and chemotherapy have been used in varying combinations, in advanced NSCLC. Only radiation of 6000 cGy in conventional fractionation, has shown a two year survival rate of 5-10%.[3] Addition of Cisplatin- based chemotherapy with radiation, shows a 24% improvement in the two year survival rate. Concomitant chemo-radiotherapy also documented an improvement of survival with a five year survival rate of 16%.[4] With these results in back ground, a Phase III randomized trial was designed at our institution, in order to evaluate different combination regimens of Radiotherapy and Chemotherapy, in unresectable NSCLC. Materials and Methods In this randomized trial, a total of 103 patients were randomized to three treatment groups -A, B and C. In group A, patients received Radiotherapy alone. In group B, patients were treated by sequential chemotherapy and radiotherapy. In group C, patients received concurrent radiotherapy and chemotherapy. All patients had measurable or evaluable disease and were diagnosed to have uncresectable NSCLC. Inclusion criteria were, patients up to 75 yrs at diagnosis, Karnofsky′s performance status (KPS) ≥60, absence of distant metastasis, no prior therapy for cancer and no hematological, cardiac, renal, or liver function abnormalities contraindicating combined modality therapy. Prior to therapy, all patients were informed about the randomization and had given written informed consent to participate in the study. The characteristics of the patients in the three randomized groups are seen in [Table - 1]. The distribution of patients prior to therapy, regarding age, stage, and performance status, is near homogenous in the three randomized groups. Treatment After completion of treatment, the patients were assessed clinically and radiologically for treatment response and for evidence of any tumour progression. Then, they were followed up at one month interval, during the first year. Thereafter, follow up examinations were performed at three months interval. Patients who failed to show response with therapy, were given salvage treatment, either with alternative chemotherapy or radiation, as and when needed. Statistical analysis Results Treatment tolerance and toxicity Acute toxicity Initial treatment response The results showed a statistically significant advantage in terms of overall survival, for those patients who were treated with CT → RT in group B ( P < 0.05), as well as those who were treated with CT+RT in group C ( P < 0.03), in comparison to patients who received only radiation in group A. But there was no statistically significant difference in terms of overall survival, between group B & C ( P < 0.52). Follow-up Survival: Survival was calculated from the date on which patients were registered in the cancer OPD, to death, or last follow up available. [Table - 5] showed that 19(59.4%) out of 32 patients in group A, 20(57%) out of 35 patients in group B and 24(66.6%) out of 36 patients in group C, survived after two years of follow up. Comparison of survival by log rank test showed P values of 0.3, 0.47 and 0.57 among the three groups A, B, & C respectively, which were not statistically significant. Distant Metastasis: During the two years follow up period, 20 patients (62.5%) in group A, 17 patients (48.6%) in group B and 16 patients (44.4%) in group C, developed distant metastasis. Brain was found to be the commonest site of distant metastasis. Metastasis in the non- regional lymph nodes, either in cervical group, or in the retroperitoneal group, were the second most common site. Distribution of site wise metastasis is shown in [Table - 6]. Time to tumor progression: Time to tumor progression in group A was 16 months (ranging from 5-20 months). In group B, it was 21 months and in group C it was also 21 months, (ranging from 8 m-22 m). The again clearly indicates, that addition of chemotherapy improves disease free survival. Discussion Therapeutic approach in unresectable NSCLC is widely discussed and a debatable problem. The optimum treatment modality, the intention of treatment and toxicity management, are major issues in the physicians′ mind. Radiation alone, as a treatment modality, was in vogue for a long time. In the RTOG 73-01 study, which had a defining role in effective dose prescription, showed that 6000cGy in conventional fractionation was effective in this disease status. Complete Response (CR) was seen in 25% of patients and with lower doses, CR was recorded as 10-20%. But survival did not improve with higher radiation dose.[3] Further improvement was achieved by means of hyper fractionate radiation therapy schedule and by three dimensional treatment planning, which enabled us to deliver a further higher dose of radiation. Dose escalation from 6000cGy to 6900cGy improved two year survival from 16 to 20% and dose escalation up to 7400cGy by three dimensional treatment planning, enhanced two year survival to 37%.[5] Subsequently, (CHART) Continuous Hyperfractionated Accelerated Radiotherapy showed a two year survival of 34%.[6],[7] Benefits of combined modality therapy, were also observed in different trials. CALGB 8433 study conclusively proved the advantage of addition of chemotherapy to radiotherapy, where they showed doubling of five year survival rate, from 7% in radiation alone group, to 17% in combined modality group.[8] The same trial also observed a median survival of 11 months in the RT alone group and that of 14 months, in the combination therapy group.[8] Trovo et al also documented similar results, with improvement in the five year survival by 16%, by addition of chemotherapy to radiotherapy. Johnson et al showed a reduced rate of distant metastasis by combination therapy, with median survival of 11 month.[10] Le Chevalier et al showed almost identical results.[11] A meta-analysis by Marino et al , showed that Cisplatin- based chemotherapy is associated with a 24% reduction in chance of metastasis, as compared to radiation alone.[4] Concurrent use of chemotherapy with radiotherapy, probably increases their individual effectivity, as one mode may sensitize tumour cell to other one. Many randomized trials[12],[13],[14],[15],[16],[17],[18],[19],[20] compared concurrent chemordiotherapy with sequential chemordiotherapy and radiotherapy alone, where few of them showed a statistically significant survival rate and others did not. Schakke-konning et al showed that concomitant chemoradiotherapy using Cisplatin, is associated with a three year survival rate of 16%, in comparison to that of 2% in the only radiation arm.[12] Reboul F et al observed that concurrent use of three weekly Cisplatinum, along with radiotherapy, had an overall response rate of 84% and a two year survival rate of 42%.[20] In the present trial, sequential chemo-radiotherapy and concomitant chemo-radiotherapy showed overall response rates of 65.7 and 66.7%, respectively, which is modest when compared with Lechavalier et al , where sequential regimen showed a response rate of over 84%. One year follow up in the present trial, also showed a poor local control in all the three groups, 18.8% in group A, 20% in group B and 25% in group C, whereas Schakke - Konning et al[12] showed a three years actuarial local control rate of 53%. Previous studies by Le chavalier et al[11] and Marino et al ,[14] documented that addition of chemotherapy to radiotherapy, could reduce the chance of metastasis by 24%. In this study, we have observed that 62.5% of patients in group A, 48.6% in group B and 44.4% in group C, developed metastasis during a two year follow up. There was about 14-18% reduction in the rate of metastasis, when chemotherapy was added to radiation, which is near similar to previous experiences. However, impact on survival remains below significant level. The only three arm study which showed a significant survival advantage, was that of Schakke-Konning et al . The improved survival of that study was attributed to improved local control. The present trial failed to show any significant effect on long term local control of disease. Poor local control might be an explanation of lower survival in our study. We conclude, that addition of chemotherapy to radiation in the treatment of unresectable NSCLC, significantly improves the initial response and thereby quality of life. Toxicities were more frequent in the combination regimen, but they were manageable. Although our study failed to show any significant survival advantage among the treatment groups, two years follow up observations show that concomitant chemo- radiotherapy has better long term control of disease, lesser chance of distant metastasis and a marginal impact on survival. References
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06011t6.jpg] [cr06011t4.jpg] [cr06011t2.jpg] [cr06011t1.jpg] [cr06011t5.jpg] [cr06011t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}