 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
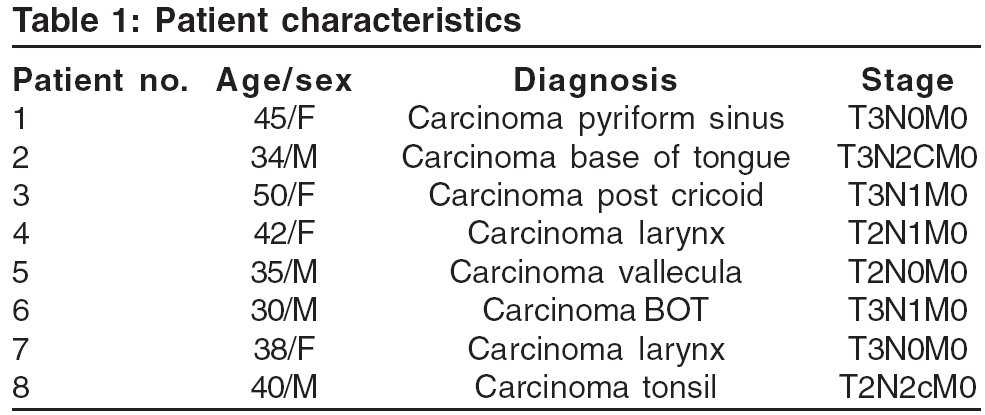
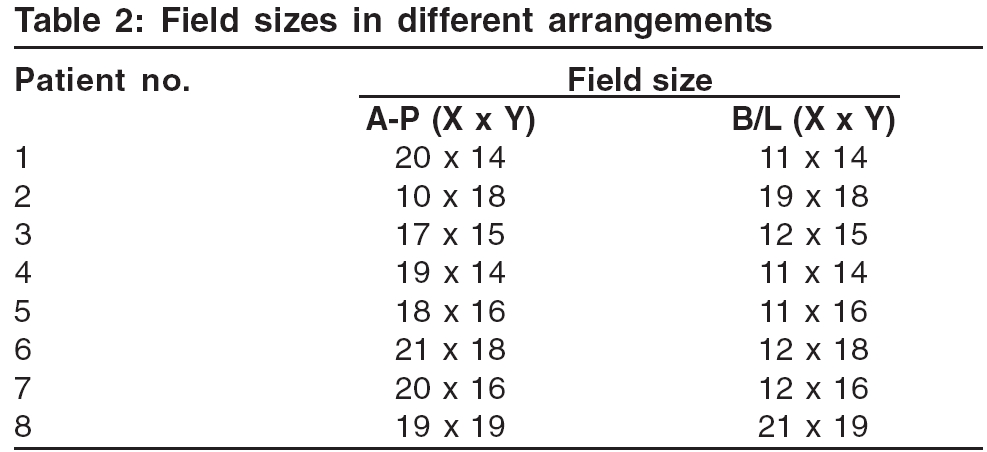
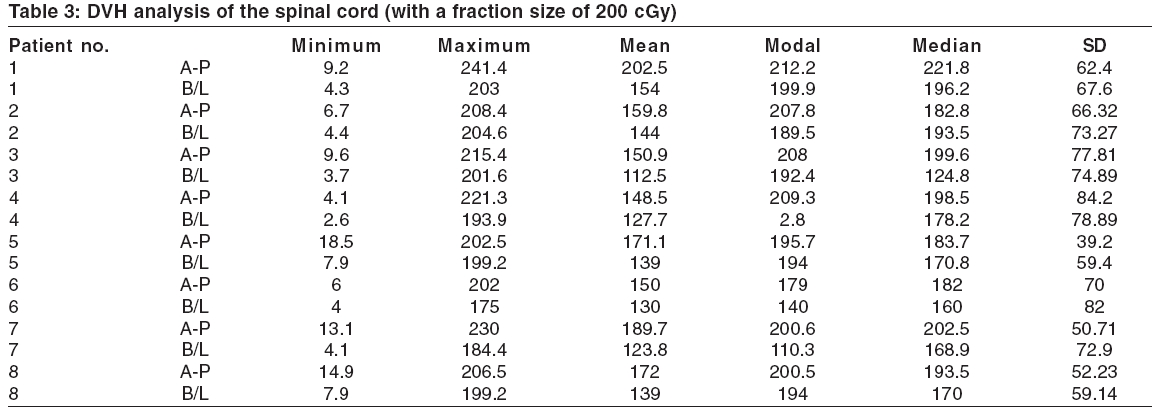
Journal of Cancer Research and Therapeutics, Vol. 2, No. 2, April-June, 2006, pp. 65-67 Original Article Radiation injury to the spinal cord in head and neck cancers: Does field arrangement have a role Anusheel Munshi, Prabhakar Ramachandran, Mohanti BidhuKalyan Department of Radiation Oncology, All India Institute of Medical Sciences, New Delhi Code Number: cr06014 Abstract Study Design: A study of eight cases of head and neck cancers, to see if the cord was getting a higher dose in the antero-posterior (A-P) fields, compared to the bilateral(B/L) fields.Objective: Radiation damage to the spinal cord is a critical issue for the radiation oncologists. This study was conducted to evaluate, if the dose to the spinal cord is higher by the antero-posterior (A-P) fields, compared to the bilateral(B/L) fields. Materials and Methods: Eight cases of head and neck cancer were taken in our study. Two beam arrangements were placed in the treatment planning system, the B/L and the A-P fields. The DVH's for the cord dose were recorded and compared in both plans, with a standard fraction size of 200cGy/fraction. Results: The mean dose to the spinal cord was 168.06cGy in A-P arrangement, while it was 133.75cGy in the B/L arrangement. Conclusion: A-P field arrangement in head and neck malignancies delivers a higher dose to the spinal cord. Therefore, we need to spare the cord at an earlier dose limit. Keywords: Radiation injury, spinal cord, field arrangement. Introduction Radiation myelitis refers exclusively to the syndrome of chronic progressive radiation myelopathy, as defined by Reagan et al .[1] This syndrome usually begins about 9 to 15 months (according to some authors up to 3 years) after the end of irradiation with paresthesias, other sensory disturbances and some-times with later development of bowel and bladder dysfunction.[2] Four clinical syndromes of radiation myelopathy, which have been traditionally described, are acute transient radiation myelopathy, acutely developing paraplegia or quadriplegia, lower motor neuron disease in the upper or lower extremities and chronic progressive radiation myelopathy.[1] Radiation damage to the spinal cord is one of the most dreaded complication in the clinical practice of radiotherapy. Radiation oncologists, consequently are always concerned about the dose to the spinal cord. Factors which have been implicated in radiation tolerance of the cord are total dose, dose per fraction, length (volume) of the spinal cord, irradiated segment of spinal cord and reirradiation of the cord.[3],[4] Unfortunately, we did not find any mention of field arrangement being a risk factor in radiation damage to the cord. The current practice of head and neck cancers in our department involves using a bilateral (B/L) opposed field arrangement, for most cases. However, an opposed anteroposterior (A-P) field arrangement is also often used e.g. in postoperative cases of carcinoma larynx, to give adequate dose to the stoma. The mid-saggital plane dosimetry analysis by Paradolo et al , has indeed shown that the variation in the surface contour can cause alteration in dose delivery.[5] We conducted this study to address the relative influence of field arrangement. Does the spinal cord suffer higher injury in head and neck cases in an A-P field arrangement? Do we therefore, actually need to spare the spine at a lower dose in this arrangement? Materials and Methods Eight consecutive cases of head and neck cancer were prospectively taken in our study. All patients were immobilized in thermoplastic orfit and neck rests were used. All of these patients underwent planning CT′s and the images were transferred to the Eclipse (Varian) planning system. Subsequently, the patients were planned with two different field arrangements. The first was the B/L field arrangement. The beams were placed with the isocentre, in the midline of the patient. All calculations were done for a dose of 200 cGy/fraction. Then the beam arrangement was changed to an A-P arrangement. In both arrangements, the length of the field and the upper and the lower borders remained the same.The field width was appropriately increased to include the bilateral supraclavicular fossae, in the A-P arrangement. For the B/L fields, the isocentre was in the mid-separation, at the point of the beam entry. This was so, because it is not possible to take an average depth for an isocentric field while treating head and neck.(in which case there would be two different isocenters for two different fields). In case of the A-P arrangement, the isocentre was decided in the following manner. Three separations of the patient were taken at the i) upper border ii) center iii) lower border. These were averaged and then divided by a factor of two. The resultant distance was the depth of the isocentre from the anterior surface of the patient. The above method is used in our department in routine treatment of patients, as well. The DVH of the spinal cord was recorded in both cases. The SPSS software (version 10) was used for all statistical analysis. Results Patient characteristics are given in [Table - 1]. There were 4 male and 4 female patients. Only patient no 7 was a postoperative patient. All the other patients were radically treated with radiotherapy. All the neck nodes were less than 3 cm in diameter. [Table - 2] gives the field sizes of the portals in the patients, in both the arranagements. [Table - 3] gives the detailed analysis of the DVH in the two arrangements. With a standard fraction size of 200 cGy/fraction, the average of the mean doses to the cord was 168.06 cGy in A-P arrangement, while it was 133.75 cGy in the B/L arrangement. The mean minimum dose in the A-P arrangement was 10.2 cGy, compared to 4.8 cGy in the B/L arrangement, while the mean maximum doses were 215.9 cGy and 195.1 cGy, respectively. The A-P fields gave a mean modal dose of 201.6 cGy, compared to 152.8 cGy by B/L fields. The average median dose was 195.55 cGy in the A-P arrangement, compared to 170.3 cGy in the B/L arrangement. Discussion The results of our study highlighted cardinal aspects of variation in cord dose with beam arrangement. The antero-posterior plan gave a higher dose to the spinal cord, in all the eight patients. More significant is the fact that in all the assessable parameters, the B/L plan scored over the A-P arrangement for protecting spinal cord. This is not unusual, as the variation in the body surface is more in the A-P field plan, compared to the B/L plan. As a result, there will certainly be portions of the cord which will receive a higher dose in the A-P plan. It is noteworthy however, that even the minimum dose in the antero-posterior plan is higher in all the eight patients. As is evident from our small but decisive study, it can be an important factor in head and neck radiotherapy. The only study available in literature, which has analysed the cord dose in head and neck radiotherapy in relation to the fields used, has been by Paradelo et al . He analysed the problem in cord dose with 3 field (2 bilateral and one anterior) technique. He found out that the cord received 110 -123% of the reference dose in some areas.[5] An increased incidence of myelopathy with high doses per fraction, has been appreciated for over 20 years. A study was done to to determine various treatment parameters influencing the likelihood of developing Lhermitte′s sign. 2901 patients with malignancies of the upper respiratory tract were analysed. Forty patients (3.6%) developed Lhermitte′s sign. An increased risk of developing Lhermitte′s sign was demonstrated for patients who received either > or = 200 cGy per fraction (one fraction per day) or > or = 5000 cGy total dose to the cervical spinal cord.[6] In another study, 12 cases of radiation myelopathies in head and neck cancer patients treated with radiotherapy, were reported.[3] All received a dose of more than 200cGy, per fraction. No patient who received 200cGy/ fraction or less, developed myelopathy. It would be pertinent to note that the A-P arrangement is detrimental to the cord, by two different mechanisms. First, it delivers a higher total dose for a given dose to the tumour. Secondly, in the A-P arrangement, even the dose per fraction is higher and so the risk of late injury increases still further, with this technique. It needs to be mentioned that not only the mean dose, but variables such as the maximum and the modal dose received by the cord, is also important. There are many published reports that indicate how far 45 Gy at 1.8-2.0 Gy per fraction is, from the dose sensitive region of the dose response curve.[2],[3] This in turn suggests that if the fraction size is of less than 200 Gy, the risk of permanent neruological damage is very low, provided the total dose is less than 45-50 Gray. The basic recommendation in textbooks and in protocol designs, is that opposed lateral treatment fields of head and neck cancer must be limited to 45 Gy, to exclude the spinal cord from further direct irradiation.[7]-[9] However, there is no literature on what should be the cut off for an A-P technique. Our study certainly provides data in this important arena. Based on our study, we feel a lower dose limit for spine shielding should be considered for the A-P technique. The cut off dose can be decided after studying a larger set of patients and the DVH′s of the cord, with more anatomical variations. In our limited study, we found that a 20% excess in mean dose and a 10% increase in maximum dose, was received by the cord in A-P technique. We propose, that in case of open field technique, we should spare the cord at least 4.5 to 9 Gy, before the dose limit we choose for the bilateral field technique. While drawing inferences from our study, it is important to note that tissue compensators were not used in the study for patients, for either field arrangement. We emphasise that this variation in the dose to the spinal cord will be highly diminished, if compensators are used in the A-P beam arrangement. In conclusion, we would like to highlight two important findings in our study. First, field arrangement should be considered a risk factor for cord injury in head and neck radiotherapy, when compensators are not used. Secondly, the use of A-P arrangement certainly gives a higher cord dose and it may be wise to go off cord at an earlier dose, compared to the B/L field. References
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06014t3.jpg] [cr06014t2.jpg] [cr06014t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}