 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
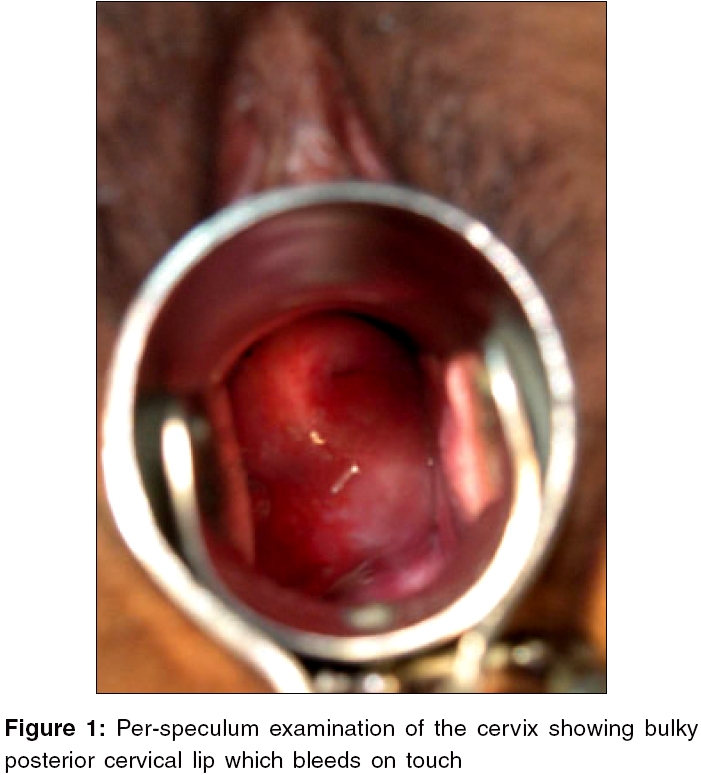
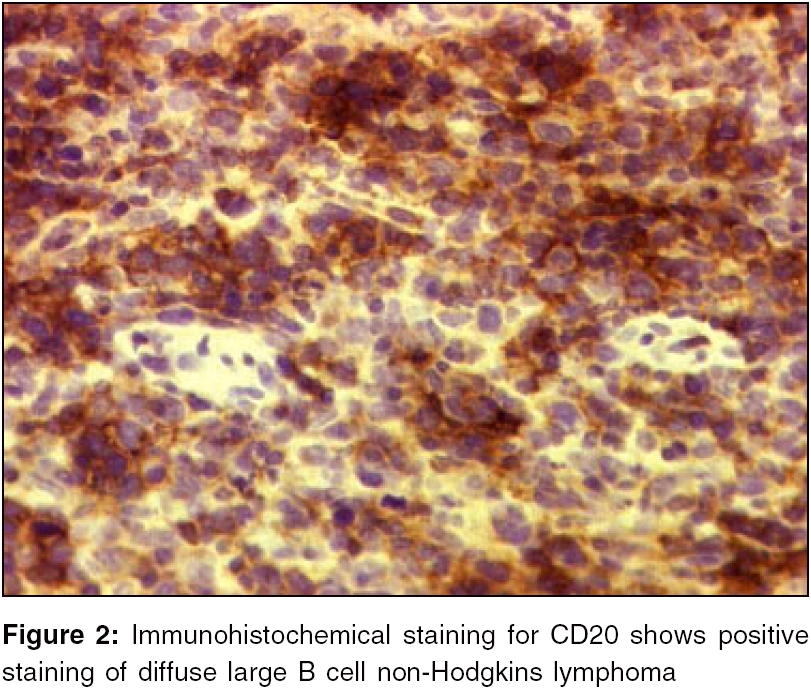
Journal of Cancer Research and Therapeutics, Vol. 2, No. 2, April-June, 2006, pp. 72-73 Case Report Cervical lymphoma presenting as irregular vaginal bleeding Sudeep Gupta, Amita Maheshwari*, Girdhar S Bhati***, Sangeeta Desai**, Hemant B Tongaonkar* Departments of Medical Oncology, *Gynecologic Oncology Service, Surgical Oncology, **Pathology, Tata Memorial Hospital, Parel, Mumbai - 400 012; ***Mahatma Gandhi Hospital, Jodhpur, Rajasthan, India Code Number: cr06016 Abstract Non-Hodgkin lymphoma (NHL) causes many deaths worldwide and its incidence is increasing. They commonly occur in middle-aged and elderly people and are disseminated at diagnosis. The patients usually present with lymphadenopathy, fever, night sweats and weight loss. We report an interesting case of NHL in a 35 year old female, who primarily presented with irregular bleeding per vaginum.Keywords: Cervix, lymphoma, vaginal bleeding. Introduction Irregular vaginal bleeding is a common symptom of many gynecological disorders, but an extremely rare presentation in non-Hodgkins lymphoma (NHL). The latter usually presents with lymphadenopathy, hepato-splenomegaly, fever, night sweats and weight loss. We report an interesting case of NHL, who primarily presented with irregular bleeding per vaginum. Case report A 35-year-old pre-menopausal female presented with irregular vaginal bleeding of two years and a whitish discharge of three months duration. Her previous menstrual cycles were regular. There was no history of fever, night sweats, or weight loss. On general physical examination, there was mild pallor. There was no lymphadenopathy or hepato-splenomegaly and the other systemic examination was normal. Per vaginal examination revealed bulky posterior cervical lip [Figure - 1], which bled on touch. Other pelvic viscera were normal. The haemoglobin was 9.9 gm/dl, WBC count was 7 x 10 9/L and platelet count was 197 x 10 9/L. Her biochemical investigations, tumor markers (CA-125, CEA and CA-19.9) and chest X-ray were normal. Computerized tomography of the abdomen and pelvis showed pre and para-aortic lymphadenopathy, focal hepatic lesions and bulky cervix. Biopsy of the cervix, taken from the posterior lip, revealed cervical stromal infiltration by pleomorphic round cells, suggestive of a high grade malignant tumour. Immunohistochemically, the tumour cells were positive for LCA and CD20 [Figure - 2] and negative for CD10, CD3, CD30, myeloperoxidase, Tdt, cytokeratin, epithelial membrane antigen, CEA, chromogranin and neuron-specific enolase, diagnostic of non-Hodgkins lymphoma, of diffuse large B cell type. Bone marrow biopsy revealed involvement by the lymphoma. The final diagnosis was non-Hodgkin′s lymphoma, stage IVAE (extranodal), by the Ann Arbor staging system. The patient was started on a third generation lymphoma protocol (MCP-842), that included Cyclophosphamide, Vincristine, Doxorubicin, Methotrexate and Cytosine arabinoside. She attained complete remission after three courses of this regimen, including resolution of the cervical and bone marrow involvement. The patient received 8 courses of this regimen, followed by standard dose involved field radiation therapy (45 Gy in 25 fractions) to the cervix. She is in complete remission, at a follow-up of 2 years. Discussion Diffuse large B-cell lymphoma is the most common subtype of NHL. It can occasionally present in extranodal sites like gastro-intestinal tract, thyroid, skin, female genital organs etc.[1] About 33% of NHL arise in tissues other than the lymph nodes, spleen, Waldeyer′s ring and thymus and these are referred to as primary extranodal NHL.[2] In our case, cervix was involved as part of the generalized disease. Our patient had a very unusual presentation with bleeding and discharge per vaginum, while the usual symptoms of lymphoma like fever, weight loss and peripheral lymphadenopathy, were absent. In this patient, cervical biopsy proved to be diagnostic; recourse to radiologically guided or open biopsy of the retroperitoneal nodes, was not required. One clue to the diagnosis of NHL, was the presence of extensive retroperitoneal lymphadenopathy. Patients with advanced-stage diffuse large B-cell lymphoma are primarily treated with chemotherapy. Radiotherapy is considered, if there is bulky disease at presentation.[3] At our centre, radiation is also given to all patients who have an extranodal site of involvement, at the end of the planned course of chemotherapy. Recent trials have shown the superiority of dose intensified regimens over the standard CHOP chemotherapy, for aggressive NHL.[4] At our centre, a similar dose-intensive regimen called MCP-842, has been in use in patients with high grade lymphomas and this was also used to treat this patient. In conclusion, gynaecologists should be aware of this diagnosis in patients presenting with abnormal vaginal bleeding. The diagnosis of extranodal involvement of female genital organs by NHL, should be suspected in patients who have these symptoms, along with extensive lymphadenopathy. References
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06016f2.jpg] [cr06016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}