 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
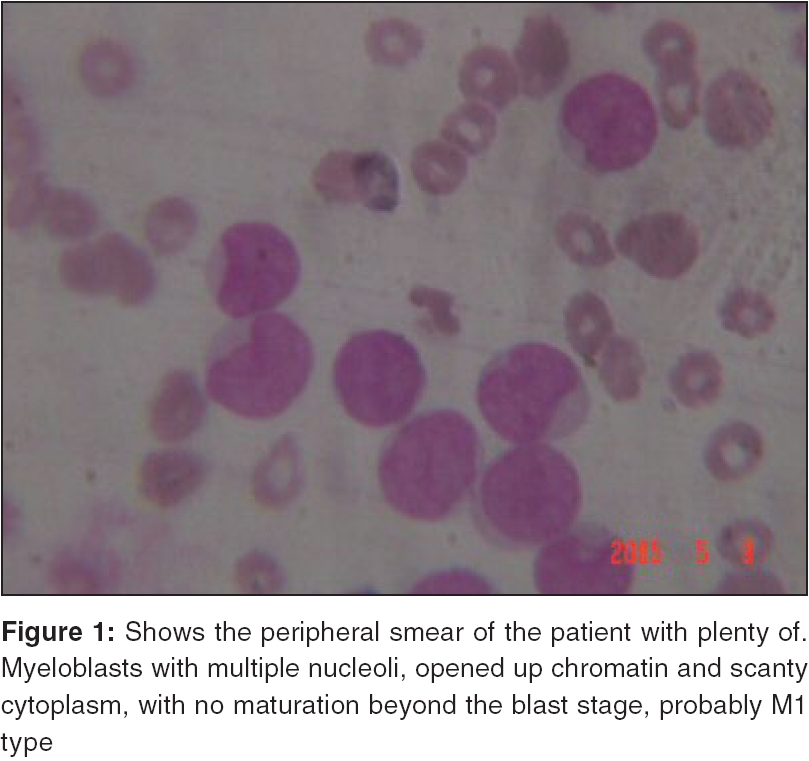
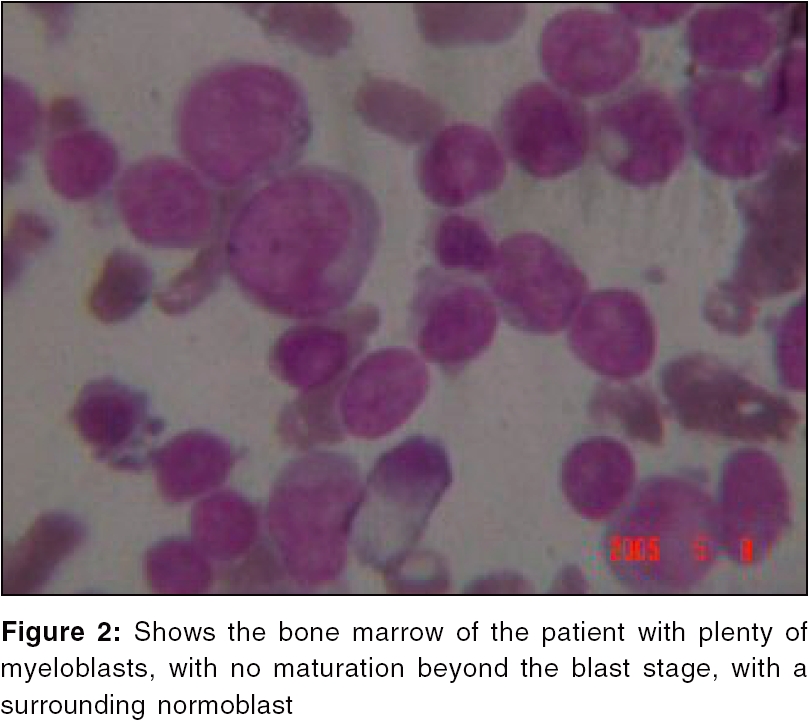
Journal of Cancer Research and Therapeutics, Vol. 2, No. 2, April-June, 2006, pp. 82-84 Brief Communications A typical presentation of acute myeloid leukemia Udayakumar N, Rajendiran C, Muthuselvan R Postgraduate in Internal Medicine, Institute of Internal Medicine, Madras Medical College and Govt. Gen Hospital, Chennai-3 Code Number: cr06020 Abstract A young man who presented with fever, altered sensorium and sudden onset tachypnea, is described. Arterial blood gas analysis, revealed the presence of severe high anion gap metabolic acidosis, with compensatory respiratory alkalosis and normal oxygen saturation. A detailed neurological, nephrological, biochemical and hematological evaluation, revealed the presence of Acute myeloid leukemia, with lactic acidosis and hyponatremia. There are very few reports of presentation of leukemia as lactic acidosis. This case report highlights the need for emergency room physicians, to consider the possibility of lactic acidosis, as one of the causes of high anion gap acidosis and to meticulously investigate the cause of lactic acidosis. We describe a rare clinical instance of lactic acidosis as the presenting manifestation of Acute myeloid leukemia.Keywords: Anion gap, lactic acidosis, myeloid leukemia, hyponatremia. Introduction Lactic acidosis, as the presenting manifestation of Acute myeloid leukemia, is rare.[1],[2] Lactic acidosis is a rare, but potentially fatal complication of Acute leukemia. The terminal phase of Acute leukemia in a 20-year-old man, heralded by lactic acidosis, is described, in order to focus attention on the occurrence of this metabolic disturbance, in the absence of overt manifestations of Acute leukemia. Case vignette Neurological examination revealed a Glasgow coma scale of 6/15. Pupils were midsize, equal and reactive to light. Fundi were normal Respiratory rate was 56/min. Blood pressure was 130/80 mm of Hg and the pulse rate was 120/mt. Plantars were tonic flexor, with normal deep tendon reflexes. There was no evidence of purpuric spots. There was no fruity odour of the breath, or of uremic fetor. Kernigs sign was negative. There was no recent history of drug intake, or of native medications. On investigating, arterial blood gas analysis revealed a pH of 7.05 (normal 7.35-7.45), a Pco2 of 10.7 mm of Hg (normal 35-35 mm of Hg), a po2 of 95 mm of Hg (normal 80-100 mm of Hg), a bicarbonate of 9.3 mmol (normal 24-28 mmol), an oxygen saturation of 96% and an anion gap of 40 mmol (normal 8-14 mmol). Blood glucose was 45 mg/dl, with normal renal parameters. Serum uric acid was 8 mg/dl (normal 2-6 mg/dl). Complete hemogram revealed a hemoglobin level of 8.8 g/dl and a total count of 1,06,000 cells/cu.mm. Peripheral smear revealed immature cells, with more than 50% myeloblasts [Figure - 1]. Platelet count was 60,000 cells/cu.mm. Smear and QBC for malarial parasite was negative. Urine examination for acetone was negative and urine for oxalate crystals was negative. Blood culture repeated twice, was negative. Toxicological analysis of body fluids for methanol, salicylates and ethylene glycol, were negative. Base line serum electrolytes showed a sodium level of 120 meq/l and a potassium level of 4.9 meq/l. Bone marrow examination was done, which revealed more than 50% myeloblasts [Figure - 2]. Computer tomography of the brain was normal. Serum lactate done, showed a value of 8.2 mmol/l (normal value 0.6-1.7 mmol/l). There was no evidence of hemodynamic instability. Cerebrospinal fluid analysis was normal. Chest roentgenogram and electrocardiogram was within normal limits. Treatment and outcome Discussion Hyponatremia and lactic acidosis as the presenting features of Acute myeloid leukemia are rare and these two were the presenting features of leukemia in our patient.[1],[2],[3] Hyponatremia is proposed to be due to inappropriate production of anti-diuretic hormone by the leukemic cells. There has been no well-defined cause for lactic acidosis due to leukemia per se, but probable explanations are due to anaerobic glycolysis by leukemic cells and due to increased blast count with its attendant leukostasis. Lactic acid parallels disease activity, in these cases.[4],[5] Acute Myeloid leukemia (AML) are a heterogeneous group of diseases, characterized by infiltration of the blood, bone marrow and other tissues, by neoplastic cells of the hematopoietic system. The diagnosis of AML is established by the presence of more than 20% myeloblasts in blood and/or bone marrow, according to the World Health Organization (WHO) Classification. Patients with AML, most often present as a consequence of anemia, leukopenia, leukocytosis, or thrombocytopenia. Fatigue is a common initial symptom. Fever and signs of abnormal hemostasis, are also common presenting features. Rarely, patients may present with symptoms from a mass lesion located in the soft tissues, cranial and spinal dura, or other organs. The mass lesion represents a tumor of leukemic cells and is called a granulocytic sarcoma or chloroma. Moreover a subset of AML, Promyelocytic leukemia presents with Disseminated intravascular coagulation, due to expression of Annexin II on the surface of tumor cells, which serves as a receptor for fibrinolytic protein, facilitating plasminogen activation, by associating plasminogen and tissue plasminogen activator on the tumor surface. Lactic acidosis is one of the most common causes of high anion gap metabolic acidosis. Lactate is the end product of anaerobic metabolism of glucose. Lactic acid accumulates, when the production exceeds utilization. The increase of lactate, that is mostly due to L-lactate, may be of two types; type A- secondary to decreased tissue perfusion, due to circulatory insufficiency (shock, circulatory failure), severe anemia, acute hypoxia, carbon monoxide poisoning and aerobic disorders, type B- in the absence of hypotension and hypoxia, due to drugs like Stavudine, salicylates, ethylene glycol, methanol and Isoniazid, renal and hepatic failure and malignancies like leukemia and lymphomas. Our patient had type B lactic acidosis because of normal oxygen saturation on ABG and no evidence of hypotension. In our case, the excessive lactic acidosis was due to increased production of lactic acid by the leukemic cells and leukostasis, together with impaired hepatic metabolization. The diminished hepatic gluconeogenesis is also documented by a hypoglycemia, in our patient. There has been only very few case reports of lactic acidosis in AML and Acidosis, as the presenting manifestation of AML per se, without secondary causes like infection and shock is still rarer. We report here, a rare instance of lactic acidosis and hyponatremia, as the presenting features of AML. Conclusion Lactic acidosis is a rare, but potentially fatal complication of Acute leukemia. The terminal phase of Acute leukemia in a 20-year-old man, heralded by lactic acidosis, is described in order to focus attention on the occurrence of this metabolic disturbance, in the absence of overt manifestations of Acute leukemia. This rare clinical entity of AML with lactic acidosis and hyponatremia, is highlighted.References
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06020f1.jpg] [cr06020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}