 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
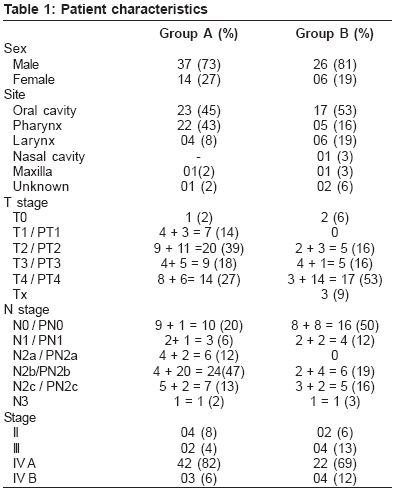
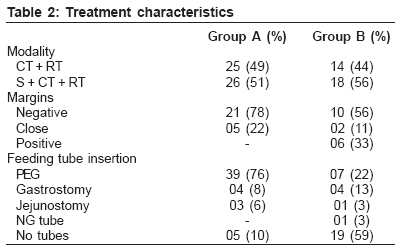
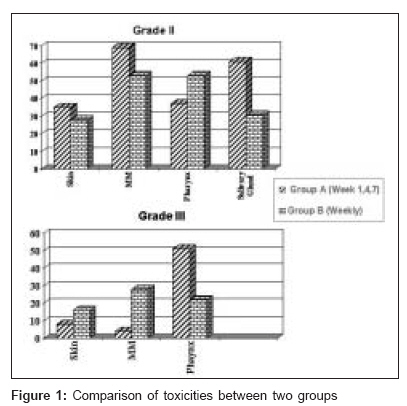
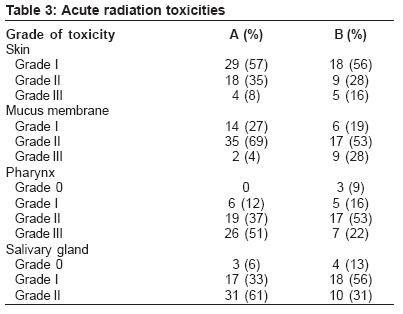
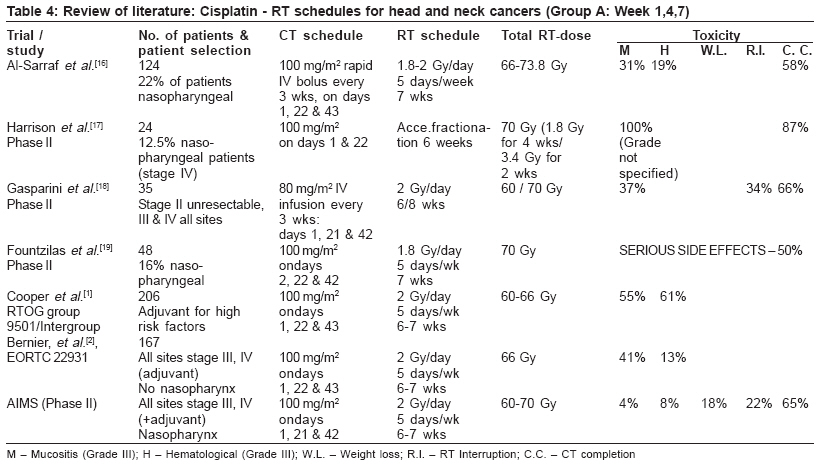
Journal of Cancer Research and Therapeutics, Vol. 2, No. 3, July-September, 2006, pp. 100-104 Original Article Comparison of acute toxicities of two chemotherapy schedules for head and neck cancers Geeta SN, Padmanabhan TK, Samuel J, Pavithran K, Iyer S, Kuriakose MA Department of Radiation Oncology, Amrita Institute of Medical Sciences, Kochi, Kerala Code Number: cr06025 Abstract Background: Chemo-radiotherapy has become the standard of care for loco-regionally advanced head and neck cancers. Platinum based regimens are the most effective. Although benefits are proven with chemo-radiation, acute toxicities are markedly increased. The dose and delivery schedules of Cisplatin have ranged from intermittent higher dose [100 mg/m2] every 3 weeks to low dose [6 mg/m2] daily administration. At present there is no data indicating which regimen is superior.Purpose: To compare acute toxicities of two chemotherapy schedules for head and neck cancers. Materials and Methods: A total of 83 head and neck cancer patients treated with two schedules of concurrent chemo RT were analyzed, retrospectively, for treatment toxicity. In group A [51 patients], chemotherapy [CT] was administered on week 1, 4 and 7 [cisplatin 100 mg/m2] over a period of 2-3 days. In group B [32 patients], CT was delivered weekly [cisplatin 40 mg/m2]. Radiotherapy dose was 7000 cGy in 35 fractions for definitive concurrent chemo-radiation and 6600 cGy in 33 fractions for adjuvant treatment. Results: Group B patients had increased grade III skin and hematological toxicity, where as patients in group A had more pharyngeal toxicity. Treatment interruptions and percentage of weight loss were higher in group B. Weekly CT schedule had higher rate of severe mucositis, which was statistically significant on both univariate [ P =0.005] and multivariate [ P =0.007] analysis. Conclusions: Three weekly CT is less toxic than weekly. Weekly CT can be made more acceptable by reducing the dose and using feeding tubes for nutrition. Keywords: Head and neck cancer, chemo-radiation, toxicity Introduction The addition of chemotherapy (CT) to radiotherapy (RT) has become the standard of care for loco-regionally advanced head and neck cancers. In the postoperative settings, two randomized trials[1],[2] have established level I evidence in favor of chemo-radiation. In unresectable disease, a phase III trial[3] showed significantly improved survival with addition of CT. Meta analysis of CT-RT trials[4] showed the benefit of adding CT to loco-regional therapy for non-metastatic disease. In trials, which used concomitant CT, absolute survival benefit was 8% at 5 years. These trials did not show any significant survival difference between the use of monotherapy and combination therapy. Platinum based regimens were the most effective regimens. The dose and delivery schedules of cisplatin have ranged from intermittent higher dose [100 mg/m 2] every 3 weeks to low dose [6 mg/m 2] daily administration.[5] In theory, high dose CT should prevent the development of distant metastasis by eradicating occult micro-metastases, but which was not evident in clinical studies,[1],[2] where as low dose weekly CT has pure radio sensitizing effect. At present there is no data suggesting which CT schedule is superior in terms of better disease control. Benefit of adding CT to RT comes at the cost of markedly increased acute toxicity, but there is no data on comparison of toxicities of CT schedules. We have compared the acute toxicities of the two CT schedules used for head and neck cancers at our Institute. Materials and Methods A total of 83 patients with histologically proven squamous cell carcinoma of head and neck, treated with two schedules of concurrent chemo RT, either adjuvant or as a primary treatment were analyzed, retrospectively, for a study period between February 2004 to October 2005. All the patients were jointly evaluated by multi-disciplinary team and treatment decisions were taken after discussion in tumor board. CT scan and MRI were done whenever necessary. AJCC Cancer Staging Manual [6th Edition] May 2002 was used for staging. Complete hematological and biochemical profiles were done before starting the treatment. Indications for CT were extra capsular spread, microscopic positive margin, Stage III and IV disease [includes adjuvant and primary], presence of perineural invasion and lymphovascular emboli, multiple positive nodes. The selection of CT schedule was at the discretion of Medical Oncologist. In group A, CT was administered on week 1, 4 and 7 [cisplatin 100 mg/m 2] over a period of two to three days [Three weekly CT]. In group B, CT was delivered weekly [cisplatin 40 mg/m 2, total number of cycles 6]. RT dose was 7000 cGy in 35 fractions for definitive concurrent chemo RT and 6600 cGy in 33 fractions for adjuvant treatment. All the patients underwent computerized tomographic simulation and subsequent 3D planning, with thermoplast immobilization, for the treatment using linear accelerator with either 4 MV or 6 MV photons. Spinal cord was shielded after 4000 cGy and posterior neck was treated with appropriate electron energy. The patients were evaluated every week during the treatment period and there after till the complete clearance of reactions. Toxicity was documented, using RTOG acute toxicity criteria.Results The median age was 55 yrs in group A and 57.5 yrs in group B. The patient characteristic is shown in [Table - 1]. The commonest site was Oral cavity constituting nearly half of the cases in both the groups. In group A, 60% of the patients had nodal disease, where as group B patients had more advanced primary disease. All the patients had histologically proven squamous cell carcinoma. Treatment characteristics are shown in [Table - 2]. In group B, 7 patients received weekly carboplatin because of contra-indication to cisplatin. Ninety percent of group A patients had some form of feeding procedure before starting the treatment. In group B, only 41% of the patients underwent feeding procedure. In three patients, procedures were done during treatment. Treatment toxicity Skin, mucous membrane, pharynx and salivary gland toxicity was compared between two groups [Figure - 1] and [Table - 3] Hematological toxicity Four patients in weekly group and 2 patients in 3 weekly groups had grade III drop in hemoglobin. Grade II neutropenia was 29% and 19% in group A and B respectively. Grade III neutopenia was higher in Group B [16% vs. 8%]. Four patients in group A and 2 patients in group B had grade I thrombocytopenia. One patient treated with weekly CT did not recover from thrombocytopenia and so further CT was abandoned. Treatment interruption and weight loss In Group B, RT treatment interruptions were more as compared to Group A [41% vs. 22%]. Number of interrupted days varied from 3 days to 18 treatment days. Significant weight loss [Defined as weight loss of more than 10 % of initial weight] was more in group B [34% vs. 18%]. Treatment completion Only one patient in group A could not complete planned RT. In group B, 3 patients had incomplete RT. (Of these, one was due to recurrence with progressive disease, another was because of chemotherapy toxicity (severe hyponatremia) and patient's refusal for further treatment). In group A, 18 [36%] patients could not receive third course of CT. In group B, 66% of the patients received 6 cycles of CT. Four patients in this group received less than five cycles. Statistical analysis Association of age, sex, site, surgical procedure , RT dose, and feeding tube insertion were analyzed with respect to toxicity and CT schedule. On both univariate and multivariate analyses, CT schedule had statistical significant association with severity of mucositis (Grade III) [ P = 0.005] and [ P = 0.007] respectively. On multivariate analysis oral cavity site had severe mucositis followed by pharynx {OR=very high}. RT dose more than 66 Gy was associated with significant weight loss {OR = 3.3, P = 0.038}. There was no correlation between treatment toxicities (skin, mucous membrane, weight loss &RT interruption) and feeding procedure. Feeding tube insertion was associated with severe dysphagia (OR=27.15; P = 0.0002). The treatment interruptions were more in stage III &IV (OR=3.32, P = 0.026). Age, sex and surgery did not influence severity of toxicity. The difference in treatment interruptions and loss of weight in both the groups was not statistically significant. Discussion A variety of chemotherapeutic agents have been used concurrently with RT either as monotherapy or combination therapy in the management of advanced head and neck cancer. Single agent cisplatin;[6],[7],[8],[9] fluorouracil;[10],[11] methotrexate;[12] bleomycin[13] and mitomycin,[14] have been used in combination with radiation therapy in several trials. These trials have shown improved response rates. Some of the trials have shown improvement in survival. Although meta-analysis of CT trials has shown no significant difference of survival with either single or combination therapy, studies have been conducted with various combinations of chemotherapeutic drugs based on the response for metastatic and recurrent cancer. Several groups have evaluated cisplatin and 5-FU in combination with radiation and shown improved control but at the cost of increased toxicity.[15] More recently, paclitaxel has been investigated with radiation treatment both as a single agent and in combination with cisplatin. Results are promising but need phase III trials evaluation and again toxicity is the main problem. In adjuvant setting, single agent CT based on platinum is the treatment of choice. So we decided to use single agent platinum based CT for both adjuvant and definitive chemoRT groups. Acute reactions are markedly increased with chemo-radiation and patients need intensive supportive care for management of nutrition and pain. At our Institute, we have involved a team of Pain and palliative care doctors along with radiation oncologists for the management of toxicity and pain. Dietary counseling is done periodically. We compared our two schedules with other studies reported in the literature. In our study, patients treated with 3 weekly regimens, grade III toxicity of skin and mucous membrane is considerably less compared to other studies [Table - 4]. This could be attributed to delivery of CT in divided doses. Huguenin et al . [20] fractionated each cycle in to five doses of 20 mg/m 2 given over five consecutive days. With this approach the severity of systemic toxicity and mucositis was low without affecting the local control. When we compared grade III hematological toxicity, it was 8% in our study, 61 % in RTOG[1] and 13% in EORTC[2] study again reflecting the importance of CT delivery in fractionated doses. The pharyngeal toxicity in our study was comparable with RTOG[1] study [49% vs. 51%] and it was manageable since 90% of these patients had feeding tubes. Sixty four percent of patients completed all 3 cycles of CT in our study, which is comparable with the studies reported in the literature. Number of studies[20],[21] showed that a substantial fraction of patients could not receive the third planned dose of cisplatin and suggested that a cumulative dose of 200 mg/m 2 might be adequate to yield same beneficial effect. Very few studies with weekly CT have documented toxicity. Grade III mucositis was 28% in our study. Serin et al .[22] with 30 mg/m 2 reported 14% of grade III toxicity. Porceddu et al .[23] used single agent platinum as weekly schedule following surgery in 47 patients. They reported confluent mucositis in 40% of the patients. CT completion [6 cycles] in our study was 64%. Glaser et al .[24] reported chemo completion in 87% of patients with 35 mg /m 2. So unlike gynaecological cancers, it appears that dose less than 40 mg is better tolerated by head and neck cancer patients. When we compared weekly and week 1, 4 and 7 schedules of CT, grade III skin, mucous membrane and hematological toxicity were higher in weekly CT. Although statistically not significant, the percentage of patients with significant weight loss was more in this group suggesting the need for feeding procedure for all patients. Also this group had more number of treatment interruptions. Quite a number of studies have shown that treatment interruptions during RT decreases local control and which is also true for altered fractionation schedule[25] but its effect with concurrent CT RT is not clear. The study by University of Michigan Network[26] used protracted chemo RT [every other week] and showed high locoregional control in patients with advanced head and neck cancer and this is being investigated in the current RTOG 97-03 study. In Summary, Week 1, 4 and 7 CT is less toxic than weekly if delivered in fractionated doses. Toxicity may be reduced in weekly CT by reducing the dose. Feeding procedure is recommended for all patients treated with concurrent chemo RT irrespective of schedule. Further evaluation is needed to compare local control and late toxicity of cisplatin in these two groups. Acknowledgement The authors wish to acknowledge Dr. K R Sundaram, for statistical analysis of the data. References
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06025f1.jpg] [cr06025t1.jpg] [cr06025t4.jpg] [cr06025t3.jpg] [cr06025t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}