 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
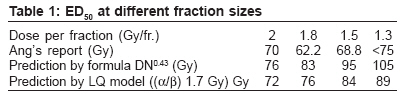
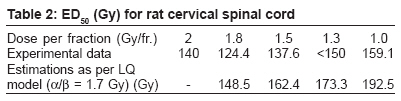
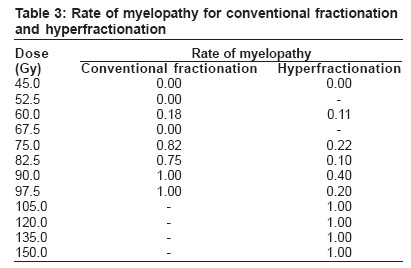
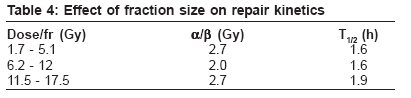
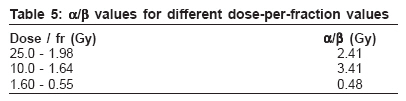
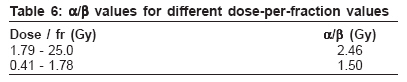
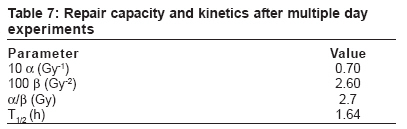
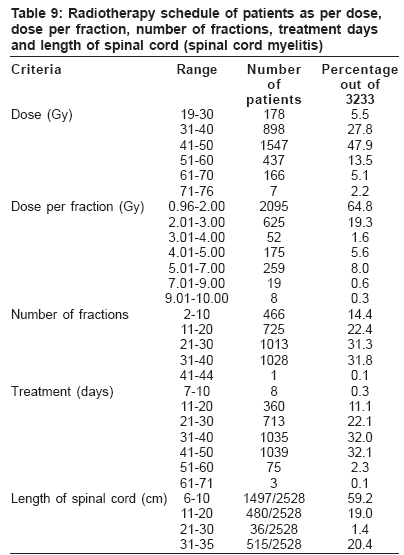
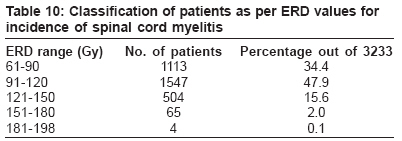
Journal of Cancer Research and Therapeutics, Vol. 2, No. 3, July-September, 2006, pp. 105-118 Original Article Spinal cord response to altered fractionation and re-irradiation: Radiobiological considerations and role of bioeffect models Sanjay S Supe, KM Ganesh, T Naveen*, Samuel Jacob**, BN Sankar*** Department of Radiation Physics, *Radiotherapy, Kidwai Memorial Institute of Oncology, Bangalore, India **Department of Radiation Oncology, Amrita Institute of Medical Sciences, Cochin, India ***Department of Physics, Anna University, Chennai, India For correspondence: Dr. Sanjay S. Supe Department of Radiation Physics, Kidwai Memorial Institute of Oncology, Hosur Road, Bangalore 560 029, Karnataka, India. E-mail: sanjayssupe@gmail.com Code Number: cr06026 ABSTRACT The aim of radiation oncologist is to implement an uncomplicated loco regional control of cancer by radiation therapy. The bioeffect of a physical dose depends on the nature of the tissue, fractionation scheme, dose rate and treatment time. The transformation of absorbed dose into a bioeffect dose is controlled by treatment variables and the radiobiological characteristics of the relevant tissue. Various bioeffect models have been proposed to predict the biological effect of radiotherapy treatments. Dale has proposed extrapolated response dose (ERD) equations for external beam therapy, intracavitary brachytherapy and interstitial brachytherapy. Within the context of the LQ model, the parameter which quantifies the overall biological effect on a given tissue is the biologically effective dose (BED) which is obtained by applying repopulation correction to ERD (Orton,). Thames proposed the total effect (TE) concept based on the incomplete repair LQ model which accounts for the biological effect of a fractionated course of radiotherapy. Spinal cord myelitis limits the dose to tumours in the head and neck, thoracic and upper abdominal regions resulting in reduction of tumour control probability. Radiation myelopathy is one of the most devastating complications of clinical radiotherapy. Treatment techniques that are designed to minimize the risk of spinal cord injury are likely to underdose the tumour consequent failure to control the disease. Since radiation myelopathy results in severe and irreversible morbidity, it is important to establish the tolerance dose of the spinal cord. A number of patients have recently been reported to have developed radiation myelopathy following hyperfractionated accelerated radiotherapy. As the survival rates of patients increase, radiation oncologists are more frequently faced with the problem of treatment of late recurrence or second tumours situated within or close to previously treated site. A rationale for taking a decision in treating in such a condition is even more complex than the original condition and requires knowledge of the kinetics of decay of occult injury of the previous treatment. To test the validity of ERD, clinically reported data of altered fractionation to the spinal cord for 7 patients reported by Wong et al , Saunders et al and Bogaert et al , were analysed, ERD values were calculated and compared with compiled clinical literature data of 3233 patients for the incidence of spinal cord myelitis reported by Cohen and Creditor, Wara et al , Abbatucci et al and Jeremic et al for conventional fractionation. ERD values were estimated with α/β of 2.5 Gy for the conventional and altered fractionation data. To test the validity of TE concept for clinical data of re-irradiation tolerance of the spinal cord, the data of the 22 patients compiled by Nieder et al were used. Clinical data compiled from the literature of Cohen and Creditor, Wara et al , Abbatucci et al and Jeremic et al , were used for comparison. The correlation of ERD with probability of spinal cord myelitis was statistically significant (P<0.001) for conventional data of 3233 patients. The incidence of spinal cord myelitis in the ERD range of 91-130 Gy is 5.3%. The ERD values for 7 clinically reported patients treated with altered fractionation schedule varied from 101 Gy to 155 Gy. To keep the incidence of spinal cord myelitis below 5% probability the ERD value of less than 91 Gy is preferable in clinical settings. TE values were estimated with α/β of 2.5 Gy for the conventional data. TE values for re-irradiation data were estimated with α/β value of 2.5 Gy for first and second course of treatment. TE values were also evaluated with 2.3 Gy for the first course and 1.9 Gy for the second course to account for variable radiosensitivity. Correlation of TE with probability of spinal cord myelitis was statistically significant for the conventional data (P<0.001). The probability of myelitis increased significantly beyond TE values of 209. The incidence of spinal cord myelitis occurred for re-irradiation data and TE1 (2.5) and TE2 (2.5) were beyond 217 for either first course or second course. The occurrence of spinal cord myelitis is found to be more probable when the total TE at 2.5 Gy is above 300. This was in agreement with conventional data where the corresponding probability was above 16.5%. The spinal cord myelitis was observed for the re-irradiation data when TE1 (2.3) or TE2 (1.9) reached a value of 202. The validity of the ERD equation is proved for the prediction of spinal cord myelitis for altered fractionation schedules. Our study also indicates that the TE formula can be meaningfully used for the prediction of re-irradiation tolerance spinal cord as it is based on strong radiobiological foundation. KEY WORDS: Hyperfractionated radiotherapy, hyperfractionation, spinal cord myelitis INTRODUCTION The aim of the radiation oncologist is to implement an uncomplicated loco regional control of cancer by radiation therapy. To achieve this goal, precise knowledge of tumoricidal dose and tolerance doseof various normal tissues is most helpful. The monumental work of Rubin and Cassarett[1] was a major setup in this direction. On the basis of nearly a century of clinical experience, a number of empirical rules have been obtained to aid the radiotherapists in achieving higher therapeutic gain. The bioeffect of a physical dose depends on the nature of the tissue, fractionation scheme, dose rate and treatment time. The translation of absorbed dose into a bioeffect dose is controlled by treatment variables and the radiobiological characteristics of the relevant tissue. Various bioeffect models have been proposed to predict the biological effect of radiotherapy treatments. From time to time, various concepts like nominal standard dose (NSD) (Ellis[2]), cumulative radiation effect (CRE) (Kirk et al [3,4]) and time dose fractionation (TDF) factors (Orton and Ellis,[5] Orton[6]) were put forward to test the equivalence of treatment schedules. The NSD formula, despite its limitations, has provided radiotherapists with an important initial setup in understanding the effects of fractionation on the tolerance of skin and connective tissue. The TDF formula allowed addition of the TDF values for different portions of a course of radiation treatment without knowledge of the full tolerance dose. Hence these concepts were widely accept-ed in spite of their empirical nature. However, doubts have been raised periodically as to the accuracy of prediction of these concepts regarding early and late effects of normal tissues and these concepts are based on connective tissue tolerance. The NSD, CRE and TDF formulas did not adequately describe the delayed effects of irradiation on other tissues (Supe[7]). Nowadays, linear quadratic (LQ) model is being used increasingly to predict the biological effect of fractionated radiotherapy using different parameters for a particular tissue like α/β, µ, K and Td (Barendsen,[8] Dale,[9] Fowler[10]; Orton and Cohen,[11] Orton,[12] Supe[7]). Dale[9] has proposed extrapolated response dose (ERD) equations for external beam therapy, intracavitary brachytherapy and interstitial brachytherapy. Within the context of the LQ model, the parameter that quantifies the overall biological effect on a given tissue is the biologically effective dose (BED) which is obtained by applying repopulation correction to ERD (Orton[12]). At least two BEDs are associated with each treatment; and in principle, two or more treatments may be inter-compared by reference to their respective tumor and late-reacting BED values. The BED concept is also of potential value in deciding how best one can reschedule an interrupted treatment. Thames and Henry[13] proposed the total effect (TE) concept, based on the incomplete repair LQ model, which accounts for the biological effect of a fractionated course of radiotherapy by quantifying two factors, viz, fractionation factor and dosage factor. TE equations for brachytherapy and altered fractionation were proposed and values of incomplete repair factor were tabulated. Due to the anatomical location of the spinal cord, the spinal cord is at risk in a large number of radiotherapy treatments. Radiation spinal cord myelitis limits the dose to tumors in the head and neck, thoracic and upper abdominal regions (Abatucci,[14] Cohen and Creditor,[15] Jeremic et al ,[16] Wara et al [17]), resulting in reduction of tumor control probability. Radiation myelopathy is one of the most devastating complications of clinical radiotherapy. Treatment techniques designed to minimize risk of spinal cord injury are likely to underdose the tumor-consequent failure to control the disease. Since radiation myelopathy results in severe and irreversible morbidity, it is important to establish the tolerance dose to the spinal cord. Establishing the influence of various prognostic factors on normal tissues requires that sufficient number of patients be treated with a wide range of fractionation regimens and that sufficient numbers develop complications. The pooling of clinical data from vast multi-institutional experience characterized by a wide diversity of dose fractionation patterns, extending over decades, yields sufficient number of patients and a wide enough range of variables for correlation of the probability of severe late sequelae. Despite the limitations of retrospective analyses, they provide useful radiobiological parameters of normal tissue responses. In fractionated radiotherapy, the total dose required to induce a certain effect on a tissue generally increases when the size of dose per fraction decreases; this is due to recovery of sublethal damage during interval between irradiation. There is evidence that late reacting normal tissues benefit relatively more from smaller fractions than rapidly proliferating tissues. From studies of normal tissue which have been reported so far, it can be concluded that the dose fractionation response is described accurately by the LQ model over the radiation dose range from large single doses down to dose per fraction of about 2 Gy. Below 2 Gy per fraction, the limited data from literature have been controversial and cast some doubt on the validity as well as the applicability of the LQ model. For late normal tissue damage, the reported values for α/β are quite small, indicating a large capacity for repairing sublethal damage. The introduction of altered fractionation schedules in clinical radiotherapy is an example of how contributions from radiobiological research and clinical observations can lead to the development of novel treatment strategies. The observations that tissues with different turnover kinetics respond differently to changes in dose fractionation and protection of radiotherapy form the basis of attempting to improve outcome by altering radiotherapy schedules. The two basic approaches that offer the prospect of an improvement in the therapeutic ratio between tumor control and late complications are: a) accelerated fractionation, in which the overall time of treatment is significantly reduced and the dose per fraction and total dose are slightly reduced compared to conventional schedule; and b) hyperfractionation, wherein a size of dose per fraction smaller than that employed in a conventional schedule without changing the overall treatment time resulting in increased total dose is used. Although the rationale is different, it is necessary to deliver several treatments per day with both strategies. Information on the rate of repair in various tissues is therefore essential for selecting an appropriate interval between radiation doses in specific situations. In order to accommodate such a requirement in a clinical department, the interval between fractions has been reduced from the conventional 24 h to no more than 3-6 h, depending on the type of treatment schedule employed. These logistic constraints may jeopardise the potential benefit of altered fractionation schedules if they compromise the normal tissue tolerance to a larger extent compared to the extent to which they affect tumor control probability because of incomplete repair between fractions. Whenever radiation therapy is given with curative intent, there is the risk of serious damage to normal tissues. This risk increases with radiation dose, as does the probability of tumor control. Thus the achievable tumor control rate depends on the radiation tolerance of the normal tissue. Unlike acute renewing tissues such as skin, gastrointestinal tract and the hemopoietic system, the late reacting tissues such as lung, spinal cord, heart and bladder have a long latent period. Late effects occur predominantly in slowly proliferating tissues. The spinal cord is a major dose-limiting organ in radiotherapy. Injury to it results in devastating functional deficits manifested over a period of one to several years after treatment. Recently, knowledge of radiobiology as applied to dose fractionation schedules has provided useful guidelines such that radiation oncologists can now limit the spinal cord dose to levels which practically eliminate the occurrence of this complication. Radiation myelopathy is one of the devastating complications of clinical radiotherapy. The spinal cord is therefore one of the major dose-limiting organs in clinical radiotherapy. Indeed, a number of patients have recently been reported to have developed radiation myelopathy following hyperfractionated accelerated radiotherapy (Dische and Saunders,[18] Dische,[19] Jeremic et al [16]). In view of the current interest in hyperfractionation and accelerated fractionation and increasing application of LQ model to clinical radiotherapy, further data are clearly desirable. As the survival rates of patients increase, radiation oncologists are more frequently faced with the problem of treatment of late recurrence or second tumors situated within or close to previously treated site (Ang et al ,[20] Knowles,[21] Lavey et al ,[22] Mason,[23] Supe et al ,[24] Wong et al [25,26]). A rationale for treatment decision in such condition is even more complex than in the original condition and requires knowledge of the kinetics of decay of occult injury from the previous treatment. The radiation oncologist contemplating the re-treatment of a site such as the neck or thorax within which the spinal cord has been previously irradiated is faced with serious medical and legal considerations. Past treatment history such as volume of spinal cord irradiated, total dose, dose per fraction, length of elapsed time since radiation exposure and spinal cord region should guide the decision-making process. Ang et al [20] commented on the lack of evidence for increased tolerance of rat spinal cord with decreasing fraction doses below 2 Gy. Rats were irradiated with 18 MV photons for cervical spinal cord. To assess the effect of small radiation doses, on the spinal cord, four fraction sizes of 1.3 Gy, 1.5 Gy, 1.8 Gy and 2 Gy were used. A constant top-up dose of 15 Gy was given. The overall treatment time was kept between 6 and 8 weeks. The percentage of number of animals in each dose group that developed white matter necrosis was used for constructing dose response curves from which the ED50 values were calculated by probit analysis. The isoeffect doses, as a function of dose per fraction, as predicated by Ellis type isoeffect formula as well as LQ model; and results of Ang’s study are summarized in Table 1. Both the Ellis type formula and the LQ model predict a continuously increasing tolerance dose with decreasing fraction size. A consequence of the present finding would be a cautious use of α/β ratios for predicting isoeffect doses at fraction size smaller than those which experimental and clinical data can predict. Van der Schueren et al [27] showed the influence of reducing the dose per fraction from 2 Gy to 1 Gy on the radiation response of the rat cervical spinal cord. The radiation treatments were carried out with 18 MV photons. A constant top-up dose of 15 Gy was delivered, the total treatment time being 4 6 weeks. The endpoint of the experiments was foreleg paralysis due to demyelination and white matter necrosis. ED50 values were calculated by probit analysis. Experimental ED50 values along with those predicted by LQ model are shown in Table 2. Small but probably significant rise in tolerance of dose was suggested, when the dose per fraction was decreased from 2 Gy to 1 Gy. This rise would however still be much less than what is predicted by the LQ model and that based on the experimental data obtained from fraction sizes larger than 2 Gy. The repair of sublethal radiation damage in the rat spinal cord in hyperfractionation experiments is incomplete for dose per fraction between 2 Gy and 1 Gy. Lavey et al [28] undertook a study to determine the extent to which hyperfractionation may spare the spinal cord as well as increase the latent period for the development of transverse myelitis. Spinal cord of mice was irradiated with a conventionally fractionated regimen of 2 Gy once daily or a hyperfractionated regimen of 1.2 Gy twice daily separated by 8 h. A top-up dose of 15 Gy was given. The spinal cord was not spared by hyperfractionation to the extent predicted by Ellis or LQ model. The threshold dose was higher in the hyperfractionated regimen than in the conventionally fractionated group. The latent period and ED50 were not significantly different between the two regimens. The continuation of the process of sublethal damage repair in the spinal cord beyond 8 h after irradiation may have influenced these results. The slow component of SLD repair should be considered in the design of hyperfractionated or accelerated radiation therapy schedules for clinical use. Data from the mouse and the rat as well as human clinical trials do not support the use of hyperfractionated radiation schedules with short interfraction intervals to deliver higher doses to spinal cord compared to conventional fractionation. Additional work is required to confirm the suggestion that hyperfractionation significantly increases the threshold dose for the induction of radiation myelitis. Niewald et al [29] examined in rats whether the radiation tolerance of spinal cord is enhanced by using hyperfractionated radiotherapy compared to a conventional schedule. Cervical spinal cords of 276 healthy rats were irradiated over 6 weeks hyperfractionally with single doses varying from 0.75 2.5 Gy and up to total doses ranging from 45 150 Gy (66 fractions) and conventionally with single doses of 1.5 4.0 Gy and up to total doses of 45 120 Gy (30 fractions). The rats were examined neurologically and were sacrificed when paralysis of the hind leg occurred. After fixation of myelopathy, the spinal cord was removed and examined histologically. Dose-effect relationship and latency from the beginning of radiotherapy to the onset of paralysis were computed and analyzed using a multivariate logistic regression model. The model fitted the data excellently [Table 3]. There were highly significant results both for the dose level and for the treatment regimen. Latency analysis showed earlier and more intense acute side effects after hyperfractionation, but radiomyelopathy occurred markedly later. These results show that compared to conventional fractionation, a distinctly higher dose of 28% could be applied using hyperfractionated radiotherapy at the 50% level of damage; and a 39% higher dose could be applied at the 5% level of damage. This finding fits well with that of the literature. For experimental purposes, these values seem suitable. The sparing effect of hyperfractionation on spinal cord as predicted by radiobiologists was confirmed. Thus it seems possible to escalate tumor doses using hyperfractionation without enhanced risk to late responding tissues. Ang et al [30] investigated the possible dependency of the kinetics of repair of sublethal damage in rat spinal cord on the fraction size. A wide range of size of dose per fraction (1.5–17.5 Gy) was given with interfraction interval varying from 0.5 to 24 h. A direct method for analysis of quantal response and an incomplete repair model for survival after fractionated exposures with shorter intervals were used to interpret the data [Table 4]. There appeared to be no significant effect of fraction size on the rate of repair. Another feature from the analysis of results is that the α/β determined from the complete repair data (1.7 Gy) is considerably smaller than that estimated from the incomplete repair data (4.3 Gy). Wong et al [31] described results of a series of experiments which were designed to assess the radiation response of the spinal cord at fraction sizes down to 0.55 Gy given once daily. All irradiation was carried out with 100 kV X-rays. For cervical spinal cord, α/β values were evaluated for three ranges of dose-per-fraction as shown in Table 5. The LQ model based on data from large doses per fraction underestimates the sparing effects of small doses per fraction, provided sufficient time is allowed between fractions for repair of sublethal damage. Wong et al [32] commented on the response of rat spinal cord to very small doses per fraction. Rat spinal cord was irradiated with top-up dose of three daily doses of 10.25 Gy, followed by graded single doses or fractionated doses. The endpoint was forelimb paralysis secondary to white matter necrosis confirmed histologically. α/β values were evaluated for two dose-perfraction ranges [Table 6]. The study provided no evidence for an increase in the radiosensitivity of rat spinal cord below 1 Gy down to 0.4 Gy per fraction. Thames et al [33] commented on whether incomplete repair explains the apparent failure of the basic LQ model to predict spinal cord and kidney responses to low-fraction doses. His findings are given Table 7. For the spinal cord, the data could be interpreted by assuming that the repair process with a half time of 1.7 h was incomplete. This half time is negligibly different from the estimate obtained from repair kinetics experiments with larger doses per fraction. The clinical implications could be that multiple-fractions-perday treatment would benefit from use of the largest feasible interfraction interval when late reactions are dose limiting. The sparing effects of hyperfractionation on spinal cord as predicted by radiobiologists could be confirmed by this experiment. Thus it seems possible to escalate tumor doses using hyperfractionation without enhanced risk to spinal cord but with higher probability of tumor cure. Jeremic et al [34] investigated whether thoracic spinal cord dose of 50.4 Gy given via 1.2 Gy per fraction, two fractions per day, carries a risk of developing radiation myelitis during studies using hyperfractionated radiation therapy with and without concurrent chemotherapy. Three hundred patients with stage III non small cell lung cancer were treated on two consecutive phase II studies and among them, 158 patients received 50.4 Gy to a portion of their spinal cord and survived >1 year after the beginning of the therapy. The interfraction interval varied from 4.5 to 6.0 h. Therefore, the influence of potentially contributing factors on the occurrence of radiation myelitis, such as interfraction interval; or those unproven yet, such as cord length or administration of concurrent chemotherapy, could not be determined. Given the continuing interest in hyperfractionated RT and encouraging results obtained in studies in lung cancer, it is clear that further investigation is needed to get more information about risk of developing thoracic radiation myelitis with this cord dose. Dische and Saunders[18] published an interim report on late morbidity for continuous hyperfractionated accelerated radiotherapy (CHART). Two hundred six patients of advanced head and neck cancer received either a total dose of 50.4 Gy at dose per fraction of 1.4 Gy or 54 Gy at dose per fraction of 1.5 Gy (3 fr/day with 6 h interval). Employing an α/β ratio of 2.5, with a dose increment of 1.5 Gy and a total dose of 42 Gy, the LQ equation gives a result of 64.2 alpha damage units and this can be compared with 72 alpha damage units for 40 Gy given in 2 Gy increments. With an increment of small doses and limited total dose of radiation in the CHART regime, there seemed a good reserve of tolerance in the spinal cord. It is of relevance that there are uncertainties as to the existence of further sparing below a dose per fraction of 2 Gy. In general, the impression that late damage with smaller fractions is less than that after conventional radiotherapy is sustained. Two patients who developed myelitis presented with advanced tumors, which responded well. A modification to avoid myelitis is essential as is also the pursuit of CHART as part of the effort to improve tumor control by modification of the programming of radiotherapy. Guttenberger et al [35] introduced a new incomplete repair (IR) model by assuming that repair is complete during long intervals, e.g., overnight intervals of 12 24 h. The model was used to assess the risk of myelopathy resulting from CHART in light of recent experimental data on the rat spinal cord. Computer simulations were carried out using a α/β value of 2 Gy. Model calculations employing incomplete repair model and bi exponential repair kinetics showed that the CHART treatments might result in a higher myelopathy risk than an equal dose given in conventional 2 Gy fractions if the parameters obtained from the animal data hold. From computer simulations, a myelopathy risk of approximately 0.3 1.2% is predicted for the currently employed maximal CHART dose to the spinal cord, i.e., 42 Gy. The CHART experience is not compatible with the new experimental data. Incomplete repair is unlikely to be the sole reason for the unexpected toxicity of CHART. However, the compounding effect of incomplete repair could be minimized by rearranging the modified CHART schedule, which would result in an increase of the tolerance dose by approximately 10%. Wong et al [36] gave a radiobiological interpretation of myelopathy in hyperfractionated accelerated radiotherapy. From 1975 to 1982, 32 patients with a diagnosis of anaplastic carcinoma of the thyroid were entered into a protocol of hyperfractionated accelerated radiotherapy. The tumor dose was 35 40 Gy at 1 Gy per fraction given 4 times a day at 3-hour intervals. Two patients developed radiation myelopathy at 8 and 13 months, total spinal cord doses being 39.9 and 48.3 Gy respectively. The risk of spinal cord damage was much higher than expected. Spinal cord doses for patients with myelopathy were 5 Gy + 35 Gy/ 35 fr/ 11 days, gap 21 days; 5 Gy + 45 Gy/ 45 fr/ 16 days, gap 13 days. Neurological symptoms indicated that the two patients had myelopathy. The neurological symptoms and signs were consistent with the anatomic level of the spinal cord irradiated. The spinal cord doses of the two patients were recalculated using the incomplete repair model described by Thames et al [33] Dose equivalent in alpha damage units was calculated using an α/β ratio of 2, 3 and 4 Gy and repair half time of 1.5, 2 and 3 h. As a consequence of the shortened interfraction interval, incomplete repair model seems to increase the radiation effects in terms of alpha damage units by 7% using a repair half time of 1.5 h and as much as 35% with repair half time of 3 h. When the accepted spinal cord tolerance, i.e., 50 Gy in 2 Gy daily fractions, was compared to the two cases in terms of alpha damage units, even corrected for lack of incomplete repair, case 1, in fact, received a dose well below what is generally accepted to be the tolerance dose for the spinal cord; and case 2 did receive a cord dose approaching cord tolerance - using repair half time of 1.5 h and 2 h respectively. When repair half time of 3 h was used in the calculations, the cord dose exceeded cord tolerance. This repair time is much greater than the values obtained from spinal cord. In the CHART regime at the Mount Vernon Hospital, Middlesex, England, there have been four cases of radiation myelopathy with doses of 46.0, 45.2, 48.3 and 46.6 Gy. All six patients developed radiation myelopathy at spinal cord doses which were considered to be well within spinal cord tolerance. There was no apparent explanation for the spinal cord damage seen. These cases therefore raise serious concerns about the underlying radiobiological model upon which these altered fractionation schemes are based. They concluded that observations of six myelopathy cases in patients treated with hyperfractionated accelerated radiotherapy and recent animal data both suggest limitations of the LQ or IR model and indicate that these models should be used with caution to predict spinal cord tolerance doses for altered fractionation regimens in clinical radiotherapy. Clinical data on the re-treatment tolerances of the spinal cord are sparse and are generally limited to the case reports. Whether the human spinal cord has the ability for long-term recovery from radiation injury is also unclear. To date, decisions regarding re-treatment tolerance of the spinal cord have largely been made empirically. In the experimental literature, there is now accumulating evidence to support the presence of time-dependent long term recovery of radiation damage to the spinal cord, with the rat spinal cord being the most common animal model studied. Early data using split doses and more recent data using fractionated doses have revealed significant long-term recovery of the radiation damage of the spinal cord in the rat, mouse, guinea pig and monkey. Ruifrok et al [37] performed experiments to investigate whether the fractionation sensitivity in the rat spinal cord changes during radiation re-treatment. All rats received first irradiation dose of 15 Gy. A second course of irradiation was given either at one day (control) or 6 months after the first dose with single dose or fractionated treatments with fraction sizes of 3, 4 and 6 Gy. The latent time for development of paresis, ED50 values and α/β values for various dose schedules are given in Table 8. Following irradiation 6 months after the first dose till latent times are shortened by about 1 2 months are compared to latency after control treatments. ED50 values were also higher for re-irradiation at 6 months’ interval. There was no significant difference in the α/β value. After a 6-month interval, the long-term recovery from the first treatment was about 45%. Ruifrok et al [37] investigated in a separate study the dose dependence and time course of long-term recovery in the cervical spinal cord of rats. The single-dose ED50 for white matter mediated paresis was about 21 Gy for 3-week-old as well as adult rats, although latency to paresis development increased from about 90 days in the 3-week-old rats to about 250 days in adult rats. The main component of the long-term recovery takes place during the first month after the initial radiation treatment of 3-week-old rats, while the main recovery is between 2 and 6 months in adult rats. This is in contrast to long-term recovery in adult rats, in which the main recovery took place between 2 and 6 months after the first irradiation. Calculations according to IR model showed that the extra dose that can be given to the cervical spinal cord after a 1 6 month interval in the 3-week-old rat represents a maximum of about 20% of the total biological effect resulting in paresis. In adult rats, the extra dose that can be given to the cervical spinal cord after a 6-month-interval represents about 40% of the total biological effect. These studies show that the time course as well as extent of long term recovery from radiation treatment not only depends on tissue and species but also on age. Wong et al [38] performed experiments to assess the re-irradiation fractionation sensitivity of the rat cervical spinal cord. Animals were given initially three daily fractions of 9 Gy representing 75% of tolerance at the ED level. After an interval of 20 weeks, they were re-irradiated with graded doses of X-rays in single, 2, 5, 10 and 20 daily fractions or a single re-treatment top-up dose of 12.5 Gy (equivalent to 80% of re-treatment tolerance), followed by doses in 1, 2, 4, 10 and 20 daily fractions. The latent periods for forelimb paralysis ranged from 189 to 245 days from the day of initial treatment or 49 to 105 days from the day of re-treatment. For animals retreated with an initial top up dose followed by smaller fractions, the latent times were similar, ranging from 188 to 233 days from the day of initial treatment. Direct fit of the LQ model gave similar α/β values of 3.07 Gy and 3.34 Gy for the re-treatment experiments without and with top up doses. The fractionation sensitivity during re-treatment compares well with that of previously un irradiated animals α/β value of 2.41 Gy for fraction sizes down to 2 Gy/fraction. Following both initial fractionation schedules, the re-treatment ED 50 values were 58% of ERD for both, i.e., 42% of the initial damage was recovered by 20 weeks. Previous radiation damage to a level of 75% tolerance dose does not change the capacity for repair of damage when the spinal cord is re irradiated with fractionated doses of X-ray at 20 weeks. Wong et al ,[25] in a separate study, investigated the influence of the level of initial radiation damage on the long term recovery and re-irradiation tolerance in the rat spinal cord. Rats were irradiated with 0, 10, 20, 30, 36 daily fractions of 2.15 Gy initially. After an interval of 20 weeks, re-treatment was given with graded single doses of X-rays. Latent times to paralysis were inversely proportional to the level of initial injury and re-treatment doses. The re-treatment ED50 were 19.0, 17.0, 15.7, 14.0 and 11.8 Gy. Using the ERD concept and α/β value of 3.0 Gy, the re-treatment ED50 in percentage ERD were 81, 70, 58 and 42 after initial doses of 25, 50, 75 and 90% ERD respectively. The level of initial injury appeared to influence the proportion of residual injury. For initial injury of 25 and 90% ERD, the residual injury was 74 and 65% respectively of the initial damage. For an initial injury of 50 and 75%, the residual injury decreased to 59 and 57% respectively. It is concluded that there was a significant long-term recovery in the rat spinal cord and the level of initial radiation damage influenced both the re-treatment tolerance and the time of expression of injury. Ang et al [39] designed a study to assess the tolerance of cervical spinal cord of Rhesus monkeys to re-irradiation. Control animals received a single course of treatment to a total dose of 70.4, 77.0 or 83.6 Gy in daily fractions of 2.2 Gy. Twelve asymptomatic animals that received 70.4 Gy were irradiated 2 years later to cumulative doses of 83.6, 92.4 or 101.2 Gy. Another group of 15 animals received 44 Gy and 2 years later, they were re-irradiated to cumulative doses of 83.6, 92.4, 101.2 or 110 Gy. The clinical endpoint was myeloparesis. The ED50 values of the single course irradiation were 76.1 ± 1.9 Gy, while the extrapolated ED50 for re-treatment after 44 Gy was > 110 Gy. Substantial recovery of occult injuries induced by initial 44 Gy had occurred within 2 years. The difference between the types of lesions observed after a single course and re-irradiation suggests that vascular injury may recover less efficiently or at a slower rate than white matter damage. Mason et al [23] assessed various factors affecting the tolerance of spinal cord to irradiation using a guinea pig model of lumbar myelopathy. A 3-cm section of lumbar spinal cord of guinea pigs was irradiated with fractionated doses of 4.5 Gy given at 5 fractions per week. Guinea pigs were primed with 9 x 4.5 Gy in 7 days, which is 60% of the ED50 for a continuous course of treatment. After 28 or 40 weeks, animals were re-treated with 6 14 fractions of 4.5 Gy. At 28 or 40 weeks after 9 x 4.5 Gy, only about 8% of the initial injury was remembered. The amount of residual injury was dependent on the initial damage as proportion of the tolerance doses. The spinal cord shows a greater capacity for long term recovery than generally appreciated and re treatment doses clinically prescribed may be lower than necessary. Lavey et al [22] designed an experiment to assess the influence of fraction size and time interval between fractions on the tolerance of spinal cord to high cumulative doses of radiation and the influence of the long-term recovery process on the tolerance of spinal cord to re-irradiation. The spinal cord of mice was irradiated using a conventionally fractionated regimen of 2.2 Gy once daily, a prolonged fractionated regimen of 1.2 Gy once daily, a hyperfractionated regimen of 1.2 Gy twice daily and a single dose of 12 Gy followed by a second dose of 5-20 Gy after 0-190 days. Mice in the multifractionated regimen group were given a single 15 Gy top-up dose 24 h after receiving a cumulative fractionated dose of 24-70 Gy. The residual from a single 12 Gy radiation dose was 17% after 190 days, leaving the re-treatment ED 50 only 10% below the ED50 of previously unirradiated spinal cord. Wong and Hao[40] aimed to assess the influence of the level of initial injury on the long term recovery kinetics of radiation damage in the central nervous system using a rat spinal cord model. The adult spinal cord was initially given two or three daily fractions of 3 Gy or three daily fractions of 10.25 Gy. At day 4 of week 6, 8, 12, 20, 28, 40, 52, animals were re-irradiated with graded single doses of X rays. The endpoint was forelimb paralysis caused by white matter necrosis. Latent time to paralysis increased with increasing time interval between initial treatment and re-irradiation but decreased with increasing size of initial injury. No significant increase in tolerance was observed for re-treatment given within 8 weeks of initial treatment. Significant long term recovery was observed thereafter and it increased with increased time interval to re-treatment. The re-treatment tolerance and radiation damage recovered at different intervals were influenced by the initial dose. Using direct analysis, the recovery kinetics could be well described by introducing a time function consisting of a linear and quadratic time component dependent on initial dose to the LQ model. Tan[41] has reported on a series of re-treatment cases with the spinal cord in both first and second course of treatments. Their treatment for carcinoma of the nasopharynx was 5500 r through two lateral and one anterior facial field to the postnasal space, given over a 6- to 7-week period as five treatments per week. The spinal cord received about 4000 r. In 22 cases, a second full course was given within a few months to 4 years after the first treatment. Three cases of radiation myelopathy occurred, two of which were reported in detail. The intervals between treatments for two reported cases were 8 and 52 months. The survival data of the non myelopathy cases were not reported. To assess the latent time, survival and dose fractionation factors associated with permanent radiation myelopathy following single and multiple courses of radiotherapy to the spinal cord, a retrospective analysis was undertaken of all patients who were registered at the Princess Margaret Hospital between 1955 and 1985 and who developed permanent radiation myelopathy (Wong et al [26]). Twenty four patients developed permanent myelopathy after one course of radiation; and 11 patients, following re-treatment. Latent times for myelopathy following a single course of treatment (18.5 months) were significantly higher than those after re-irradiation (11.4 months). There was not a single incident of myelopathy in patients who received fractionated radiotherapy given once daily to an ERD of 100 Gy2 (equivalent to 50 Gy in 25 daily fractions). Four patients who developed myelopathy after an ERD of <100 Gy2 were all treated on accelerated fractionation protocols. Patients who were re-irradiated received significantly higher dose (ERD 148 Gy2) than those who had a single course of treatment (ERD 121 Gy2). Risk of myelopathy with conventional fractionation was extremely small, multiple fraction per day reduced spinal cord tolerance, latent time to myelopathy decreased following re-treatment and there was possible long term recovery of radiation damage in the human spinal cord. In summary, recovery from initial damage has been well proven. The amount of recovery seems to be influenced by different factors, mainly the initial damage expressed as a percentage of cord tolerance. The interval between the first treatment and re-treatment is probably also important. The real total tolerance of the spinal cord may be about 130% of the tolerance dose for the first treatment as estimated by Kogel.[42] Although the general phenomenon of repair is surely present in humans as compared to animals, some controversies remain in terms of transforming the experimental animal data to the clinic. First, the histological pattern of radiation myelitis in guinea pigs differs from that in humans. Secondly, the repair kinetics is probably different and it is questionable how long it takes to achieve maximal repair and re-tolerance in humans. Schultheiss and Stephens,[43] in their review of permanent radiation myelopathy, conclude: ‘Because of the life span, latency and dose response difference, only general guidelines for clinical application can be offered from the rodent data. These data indicate that substantial recovery of spinal cord tolerance is achieved during a sufficiently long interval after initial radiation therapy. In general, a higher re-treatment dose can be given following lower initial doses and longer intervals between treatments. From the sparse clinical and primate data, it appears that at least 50% recovery of 45 Gy would be obtained 2 years after treatment.’ We must be cautious in the interpretation of clinical reports where there is a low incidence of complication of treatment, for there is always the possibility of technical error, complicating factor and unusual sensitivity. Radiation myelopathy is however one of the most serious occurrences following radiotherapy and even a low incidence associated with a new regime must be carefully considered. The rare myelopathies that do occur at low doses (≤45 Gy) are seen for three reasons: a) Extrinsic factors reduce some individuals’ radiation tolerance b) Tens of thousands of patients are irradiated annually at these doses c) The true dose was larger than estimated. The clinical observations also underscore the importance of obtaining radiobiological data in clinically relevant dose fractionation schemes to confirm or refute predictions from biological models. The ultimate test for the validity of a biological model, however, is ‘the clinical observations.’ More importantly, the final model is the patient undergoing radiotherapy and this experience underlines the need for very careful observation of patients entered into clinical trials of methods to improve the effectiveness of treatment. Normal tissue effects must be observed with the same meticulous care as given to tumor control. It is most important that promising methods for improvement of tumor control must be abandoned because of such problems. Knowledge concerning morbidity gained from the laboratory and the clinic must be applied to its prevention and advance in management must be continued. According to Ang et al ,[39] recent evidence indicates that isoeffect dose for spinal cord may be overestimated for fraction sizes as small as 1 or 2 Gy when calculated for a LQ model fitted to data obtained from fraction sizes larger than 2 Gy. Reasons for this are unknown, but possible interpretations include exhaustion of repair capacity and incomplete repair in experiments designed to study the response to these small doses. Moreover, still further data suggest otherwise; in view of the devastating effect of radiation myelopathy, one must not assume the spinal cord to have a greater tolerance at fraction sizes below 1.8 to 2 Gy. Further experimental data are desirable to confirm the validity of the LQ model at small doses per fraction and to characterize the repair kinetics at small doses per fraction. At present, in clinical protocols of multiple daily fractions, it is essential to space the fractions with as long an interfraction interval as possible. In view of the devastating effect of radiation myelopathy, repair of sublethal damage in the spinal cord or central nervous system cannot be regarded to be complete even after an interfraction interval of 8 h. The repair kinetics in spinal cord is slower than previously anticipated. Therefore, there is no rationale to use interfraction intervals <6 h. The appearance of radiation myelitis in patients receiving accelerated radiotherapy has led to further laboratory experiments, particularly with a view to determine the half time of repair in neural tissue. Experiments suggest that there may be a component of repair in the nervous system beyond 4 h after the irradiation. Such a component must be expected to increase the risk of radiation injury when two or more fractions are given each day. When the half time of repair exceeds 4 h, even an extension of the interval between treatments to 8 h will still leave a considerable element of non repaired damage; and if all treatments are given, as in CHART, over a continuous 12-day period, there will also be an accumulation of non repaired damage at the end of each treatment day. The evidence now available suggests that in accelerated treatment, sparing of late damage in spinal cord with use of hyperfractionation does not occur and that when equal doses are given, it is increased. Mathematical models based upon analysis of laboratory and clinical data are extremely important in advancing our knowledge. It is unfortunate that the standard of practice for listing incidental doses to the spinal cord is determined more by litigation than by clinical judgment. Tumoricidal doses should never be compromised for the purpose of limiting the cord dose to 45 Gy. Limiting the cord dose to 45 Gy in a hyperfractionation schedule forces even greater likelihood of compromising the tumor dose. Many experts have recommended 50 Gy in 2 Gy fractions as an acceptable level of spinal cord dose and this recommendation is probably conservative. Even high doses could be given if the clinical situation requires them and the patient is properly informed of the risk and the consequences of myelopathy. It is not by limiting the spinal cord dose that the incidence of myelopathy should be reduced but rather by determining what factors in the patient’s medical history and physical status make the spinal cord more sensitive than expected. By controlling excessive risk factors, myelopathies can be kept to a minimum and tumor dose can be prescribed to suit the disease. The spinal cord is a major dose-limiting organ in radiotherapy. Injury to it results in devastating functional deficits manifested one to several years after treatment. Recently knowledge of radiobiology as applied to dose fractionation schedules has provided useful guidelines such that radiation oncologists can now limit the spinal cord dose to levels which practically eliminate the occurrence of this complication. If treatment to the spinal cord is too conservative, a less-thanoptimum tumor dose and diminished probability of local tumor control may result. Thus primarily, the question is - Is a higher tumor dose worth it, considering the increased risk of myelopathy in clinical situations? Since radiation myelopathy is the most catastrophic late consequence of radiotherapy, clinicians usually err on the side of conservatism when the spinal cord is within the treatment volume. The present study was undertaken with the following aims: 1) to test the validity of ERD for clinical data of spinal cord myelitis for altered fractionation and 2) to test the validity of TE concept for clinical data of re-irradiation tolerance of the spinal cord. MATERIALS AND METHODS To test the validity of ERD in altered fractionation regimen in the incidence of spinal cord myelitis, the clinical data of time-dose fractionation schedules and incidence of myelitis for 3,233 patients compiled from the data of Cohen and Creditor,[15] Wara et al ,[17] Abbatucci[14] and Jeremic et al [16] were used as the reference for analysis [Table 9]. ERD values for this data were evaluated with Equation 1. Classification of patients as per ERD values for incidence of spinal cord myelitis are presented in Table 10. ERD = 1.25 Nd [1+ d/(α/β)] x-0.13 (1) Altered fractionation data of patients with spinal cord myelitis - as reported by Wong[31] for two patients; as reported by Saunders et al [44] for four patients; and as reported by Bogaert et al [45] for one patient - are compiled in Table 11. ERD values of these data are evaluated with the Equations 2 and 3 for an α/β value of 2.5 Gy, suggested by Orton[11] for spinal cord myelitis,
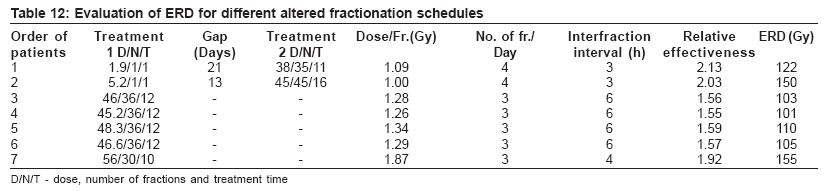
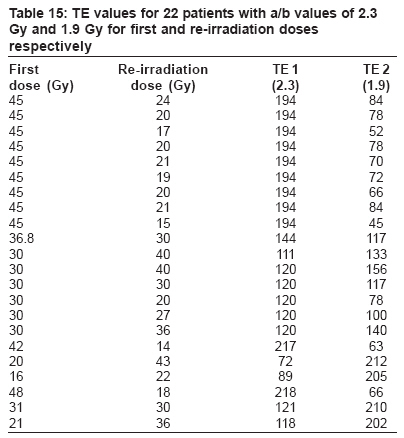
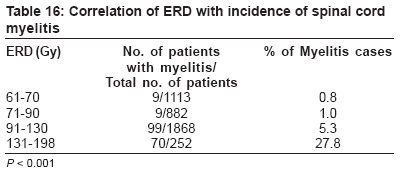
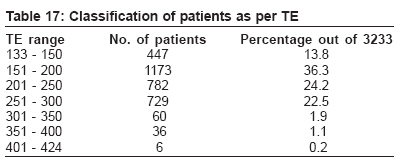
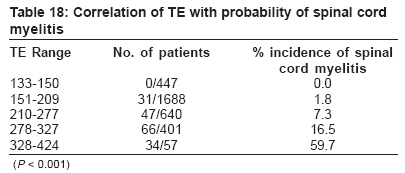
The ERD values are evaluated using either Equation 2 or Equation 3 respectively for 2 fractions / day or 3 fractions / day and using the Equation 1; these are tabulated in Table 12. To test the validity of TE concept for clinical data of re-irradiation tolerance of the spinal cord, the clinical data of time-dose fractionation schedules and incidence of myelitis of 3,233 patients compiled from the data of Cohen and Creditor,[15] Wara et al ,[11] Abbatucci[14] and Jeremic et al [16] as classified in Table 9 are used. From α/β value of 2.5 Gy, as suggested by Orton[11] for spinal cord myelitis, TE values are calculated using Equation 5 for 3,233 patients.
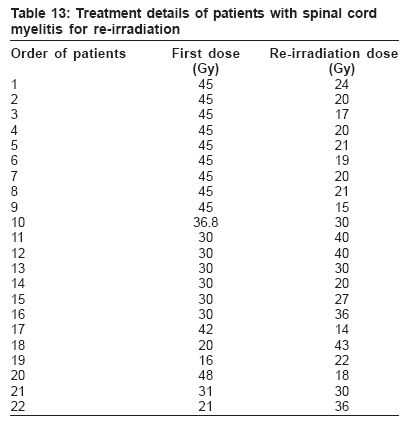
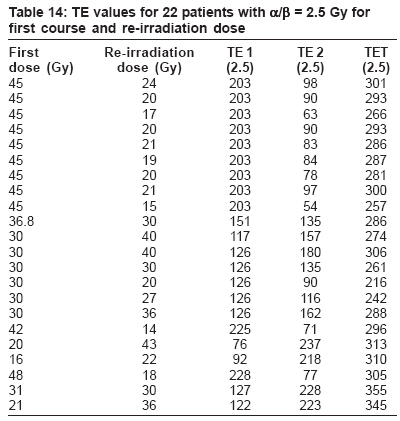
where hm is the incomplete repair factor. In order to check whether the TE concept may be applied for re-irradiated patients too, the combined data of Nieder et al ,[46] as compiled from the works of Jackson and Ball,[47] Bauman et al ,[48] Magrini et al [49] and Wong et al ,[50] were used and TE values were calculated using Equation 5 with an α/β value of 2.5 Gy, as in the case of 3,233 patients. In addition, to account for variable radiosensitivity of the 22 patients to re-irradiation, while calculating TE values, α/β values of 2.3 Gy and 1.9 Gy were used for first course and second course respectively. These two values of α/β were chosen based on the study of irradiation of rat spinal cord (Ruifrok et al [37]). The treatment details of these 22 patients are reported in Table 13 (Nieder et al [46]). The calculated values of TE for the said 22 patients are presented in Table 14 for an α/β value of 2.5 Gy, in which the total TE is indicated as TET (2.5) in the last column; and in Table 15, for an α/β value of 2.3 Gy for first course and 1.9 Gy for the second course. Equation 6 is used for calculation of TE value for patient no. 11, while Equation 5 is used for calculation of TE values for all other patients. The incomplete repair factor hM in Equation 6, with a value of 0.0625 for twice-a-day fraction, takes care of hyperfractionation of patient no. 11. Out of 22 patients reported by Nieder, the first 9 patients in the Table 13 were reported by Jackson and Ball[47] with a first dose of 45 Gy and re-irradiation dose varying from15 to 24 Gy with an approximate interval of 6 to 48 months. While patient no. 10 (reported by Bauman et al [48]) was given a first dose of 45 Gy and a re-irradiation dose of 30 Gy with a gap of 20 months, the patient no.11, reported by the same authors, had his first course of 30 Gy in two hyperfractionations (two fractions per day) and a re-irradiation dose of 40 Gy with a gap of 8 months. Patients numbered 12 to 16, reported by Magrini et al ,[49] had a first dose of 30 Gy and a re-irradiation dose varying from 20 to 40 Gy with a gap of 1 to 3 years. However, patients numbered 17 to 22, reported by Wong et al ,[26] had a first dose varying from 16 to 48 Gy and a re-irradiation dose varying from 14 to 43 Gy with a gap ranging from 4 to 71 months. RESULTS For testing of validity of ERD, the clinical data of 3,233 patients is used as reference to prove the validity of ERD concept and the values were obtained using Equation 1 and the results are classified and presented in Table 10. The ERD values for 3,233 patients varied from 61 to 198 Gy, which for the maximum number of patients lay in the range of 91 to 120 Gy [Table 10]. For reference data, the correlation of ERD with probability of spinal cord myelitis was statistically significant (P < 0.001) [Table 16]. The incidence of spinal cord myelitis is 5.3% in the ERD range of 91-130 Gy. Beyond ERD of 130 Gy, the incidence of spinal cord myelitis increased very sharply to 27.8%. ERD values for altered fractionation are given in Table 12. The ERD values obtained from clinically reported data of seven patients treated with altered fractionation schedules (using Equations 2 and 3) with α/β value of 2.5 Gy for myelitis are presented in Table 12. The ERD values reveal that the minimum value is 101 Gy and the maximum value is 155 Gy. These values when compared with reference data indicated incidence of greater than 5.3% as per ERD for conventional fractionation. Hence these seven patients treated with altered fractionation had spinal cord myelitis, as expected on the basis of comparison of ERD values. To prove the TE concept as prognostic tool for evaluation of re- irradiation tolerance of spinal cord, TE values were evaluated for the compiled data of 3,233 patients as described in Table 9 using Equation 5. The results were classified and tabulated in Table 17. These results were used for comparison with re-irradiation data of 22 clinically reported patients. Maximum number of patients had TE values varying from 151 to 200 (36.3%). Out of 3,233 patients analyzed, the correlation of TE with probability of spinal cord myelitis was statistically significant (P < 0.001). In the TE range of 133 to 150, 447 patients were treated and no incidence of spinal cord myelitis was reported [Table 18]. But the incidence of spinal cord myelitis was significant in the 210-277 TE range, averaging about 7.3% in 640 patients treated. The maximum incidence of spinal cord myelitis - about 59.7% - was reported in 34 patients out of 57 patients treated in the TE range of 328-424. The TE values for the clinically reported 22 patients [Table 14] by Nieder et al [46] for re-irradiation showed that the first course dose varied from 16 to 48 Gy and the re-irradiation dose varied from 14 to 43 Gy with minimal interval of 4 months to a maximum of 57 months. The TE1 (2.5) values varied from 76 to 228 and TE2 (2.5) varied from 63 to 237. The total TE {TET (2.5)} values varied from 216 to 355 and indicated a cut-off of 296. The incidence of spinal cord injury was reported for the last 6 patients in Table 14. The TE values evaluated with α/β value of 2.3 Gy and 1.9 Gy for first treatment and the re-irradiation treatment schedule (to account for variable radiosensitivity) respectively were also tabulated [Table 15] and studied for all the 22 patients mentioned. The TE1 (2.3) values varied from 72 to 218 and the TE2 (1.9) values varied from 45 to 212 for the first and re-irradiation doses respectively and the spinal cord myelitis was observed when TE1 (2.3) or TE2 (1.9) reached a value of 202. DISCUSSION To test the validity of ERD in altered fractionation regimen in the incidence of spinal cord myelitis, the clinical data of time-dose fractionation schedules and incidence of myelitis for 3,233 patients were used as the reference for analysis. As described in ‘Material and Methods’ section, the ERD values for this data were evaluated using Equation 1 and are given in the Table 10. ERD values for altered fractionation data of 7 patients were evaluated using Equations 2 and 3 and are tabulated in Table 12. Validity of ERD concept was tested in this study for spinal cord myelitis with altered fractionation. Because the ERD values of the altered fractionation data were between 101 and 155 Gy, which fall in the range of incidence greater than 5.3% as per the conventional data, the incidence of spinal cord myelitis is justified. The study indicates that the ERD values derived for both conventional literature data of 3,233 patients and the altered fractionation data of 7 patients were in agreement as per the incidence of spinal cord myelitis. Hence the validity of the ERD equation is proved for the prediction of spinal cord myelitis for altered fraction schedules. To keep the incidence of spinal cord myelitis below the acceptable level of 5%, an ERD value of less than 91 Gy is preferable clinically. To prove that the TE concept is a prognostic tool for evaluation of re-irradiation tolerance of spinal cord, TE values were evaluated for the compiled data of 3,233 patients, as described in Table 9, using Equation 5. The results were classified and tabulated in Table 16. These results were used for comparison with re-irradiation data of 22 clinically reported patients, given in Table 13. The TE values for these 22 patients were also calculated taking into account the variable radiosensitivity and are presented in Table 15. The TE concept was applied to re-irradiation data of spinal cord myelitis. The TE1 (2.5) and TE2 (2.5) values were analyzed for the 22 cases and the incidences of spinal cord myelitis were interpreted. It is evident that the incidence of spinal cord myelitis was reported for the TET (2.5) values greater than 296. For patients with spinal cord myelitis, the TET (2.5) values varied from 296 to 355 (last 6 patients in Table 14). Some patients had TET (2.5) greater than 296 (patient 1, 8 and 12 of Table 14) but were not reported with incidence of spinal cord myelitis because their TE1 (2.5) or TE2 (2.5) values had never crossed 218 in either first or re-irradiation course of treatments. The TE1 (2.3) and TE2 (1.9) values calculated to account for variable radiosensitivity from Table 15 also depict the above result. The reported clinical incidence of spinal cord myelitis (last six patients of Table 15) showed that either TE1 (2.3) or TE2 (1.9) was greater than 202. The patients who had not reported with incidence of spinal cord myelitis had TE (2.3) and TE (1.9) values less than 194 (patients 1 to16 of Table 15) The above findings were compared with the compiled literature data of 3,233 patients and the range values of TE were given in Table 17. In Table 18, the incidence of spinal cord myelitis was reported to increase to 7.3% beyond TE values of 209. But the TET (2.5) values from Table 14 show that even if the values were greater than 210, there was no incidence of spinal cord myelitis. This may be due to increased gap of up to 48 months between the first and re-irradiation courses of treatment. Our TET (2.5) findings of 22 patients are in agreement with data of 3,233 conventionally treated patient for the incidence of spinal cord myelitis in the TE (2.5) range of 278-327, which amounts to about 16.5%. This study indicates that the TE formula can be meaningfully used for the prediction of re-irradiation tolerance of spinal cord as it is based on strong radiobiological foundation. Also the study indicates that the total TE values should never cross 209 in order to limit the probability of spinal cord myelitis to less than 5% in the clinical setting. This is well pronounced when α/β values of 2.3 and 1.9 Gy were used to account for variable radiosensitivity for the first and re-irradiation courses respectively. The results of our findings supplemented the findings of other authors and proved the validity of TE concept in the prediction of re-irradiation tolerance of spinal cord. The application of ERD to the clinical data of altered fractionation was valid. Incidences of spinal cord myelitis resulting in studies with altered fractionation were explained on the basis of ERD by comparison with clinical data of conventional fractionation. TE concept was applicable to clinical data of re-irradiation tolerance of spinal cord. The incidences of spinal cord myelitis from re-irradiation instances were justified on the basis of TE by comparison with clinical data of single treatments. ACKNOWLEDGMENTS This article contains materials presented in our earlier four published papers. We would like to thank the editors of these journals for allowing us to use the materials of articles published in their journal. REFERENCES
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06026t17.jpg] [cr06026t15.jpg] [cr06026t18.jpg] [cr06026t13.jpg] [cr06026t2.jpg] [cr06026t4.jpg] [cr06026t9.jpg] [cr06026t11.jpg] [cr06026t16.jpg] [cr06026t7.jpg] [cr06026t6.jpg] [cr06026t5.jpg] [cr06026t12.jpg] [cr06026t10.jpg] [cr06026t8.jpg] [cr06026t14.jpg] [cr06026t1.jpg] [cr06026t3.jpg] |
| |||||||||



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}