 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
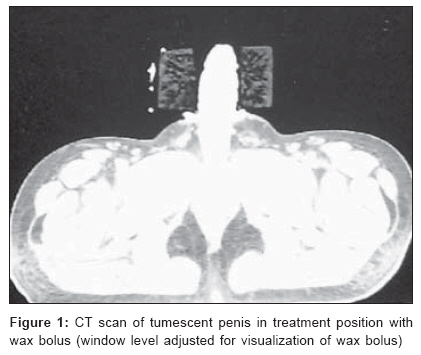
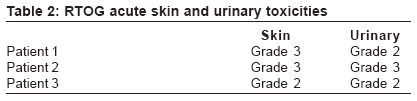
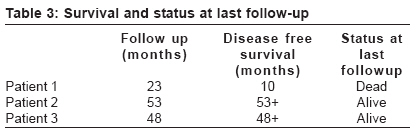
Journal of Cancer Research and Therapeutics, Vol. 2, No. 3, July-September, 2006, pp. 132-135 Original Article A new indication of sildenafil in medicine: Hypoxic cell sensitizer for penile cancer Huilgol NagrajG, Jain Amit Department of Radiation Oncology, Nanavati Hospital, Mumbai Code Number: cr06030 Abstract Purpose: To evaluate the feasibility and results of sildenafil used as radiosensitizer by causing penile vasodilatation and reducing tumor hypoxia in radical radiotherapy for penile cancer.Materials and Methods: Three men with histopathologic diagnosis of squamous carcinoma of penis were treated with radical external radiotherapy with concomitant sildenafil. Acute and late adverse events were noted according to RTOG toxicity criteria. Response to radiotherapy, as well as disease-free and overall survivals, was evaluated. Results: All three patients achieved tumescence, completed the treatment and achieved complete response. One patient had recurrence at 10 months and died of the disease after 23 months from starting the treatment. Other two patients are disease-free and alive at 48 and 53 months respectively. No excess acute or late adverse event was observed. Conclusion: Sildenafil may act as radiosensitizer by causing penile vasodilatation and reducing hypoxia. Larger controlled studies are required to validate the hypothesis. Keywords: Carcinoma penis, hypoxia, radiotherapy, sildenafil Introduction enile carcinoma is an uncommon urogenital cancer. The age-adjusted incidence in India is 2-3 cases per lakh.[1] The traditional treatment of penile cancer has been partial or total amputation of penis with or without inguinal dissection. Radical radiation with external beam radiotherapy or with temporary interstitial implants has been successfully practiced.[2],[3],[4] Hypoxia in the tumor has been shown to impart radioresistance and the tumor's overall oxygenation status has emerged as a strong predictive and prognostic factor of local control after radiotherapy, particularly in squamous carcinomas and soft tissue sarcomas.[5],[6],[7],[8],[9],[10] Manipulation of oxic state to improve sensitivity to ionizing radiation is one of the strategies to obviate the deterrent to a complete response. The meta-analysis by Overgaard et al of 83 randomized trials which compared radiotherapy alone with radiotherapy combined with any modality reducing the hypoxia in the tumor showed improvement in both disease-free survival and overall survival in favor of the addition of hypoxia-targeting modality.[11] In bulky penile cancer, the hypoxic core presents a challenge. Sildenafil is being tried in few other medical conditions after its major success in erectile dysfunction. Its major action is inhibition of enzyme phosphodiesterase type 5 mediated metabolism of cyclic guanosine monophosphate (cGMP), causing cGMP-induced relaxation of arteriolar smooth muscle and vasodilatation. It has been found successful in pulmonary arterial hypertension by causing vasodilatation and reducing hypoxia and is an FDA-approved indication after a large randomized trial.[12] Its efficacy has been demonstrated in Raynaud's phenomenon.[13] Few preclinical and clinical studies have shown a beneficial effect in patients with infertility, which is due to increased genital blood flow and increase in endometrial thickness.[14] Sildenafil increases blood flow to penile structure and can reduce chronic and acute perfusion-related hypoxia. The site-specificity of drug is due to higher concentration of the enzyme phosphodiesterase in penile tissue. The present study was conducted to develop a proof of the following hypothesis: 'Sildenafil-induced increase in perfusion reduces hypoxia, which increases radiation sensitivity.' We performed a pilot study of three patients of penile cancer treated with radical radiotherapy and concomitant sildenafil and here we report our preliminary experience. Materials and Methods Three men with diagnosis of carcinoma of penis were treated with radical radiotherapy and concomitant sildenafil. All three patients had biopsy-proven histopathologic diagnosis of squamous cell carcinoma of penis. Patients underwent thorough clinical examination, ultrasonography of abdomen and pelvis and radiographic examination of chest to evaluate regional and distant metastases. The study had been approved by the hospital's ethics committee. A written informed consent was taken from the patients for the radiotherapy treatment with concomitant sildenafil. Acute and late toxicities were measured according to RTOG toxicity criteria. Patient characteristics The patients were 46, 80 and 35 years old respectively at the time of presentation. The first two patients had lesion on the glans, which was infiltrative- and ulceroinfiltrative-type respectively, while the third patient had an exophytic lesion on the shaft of penis. The grade and American Joint Committee on Cancer (AJCC) staging are as shown in [Table - 1]. Sildenafil Sildenafil was given orally - 50 mg, daily 30 min - before the radiation. It was given 5 days a week along with the radiation. Radiotherapy Patients were treated in supine position with tumescent penis wrapped in water gauze and held in upright position in the central core of a cylindrical 10 x 10 cm wax bolus. Patients were treated with Cobalt 60 gamma rays with bilateral portals normalized at midplane of the wax cylinder. A lead plate was placed beneath the wax cylinder to shield the testes. The inguinal nodes of Patients 1 and 3 were treated with direct anterior portal. Patients 1 and 3 were treated to 60 Gy in 30 daily fractions to penis and 50 Gy in 20 daily fractions to bilateral inguinal nodes. Patient 2 was treated first with 250 cGy per fraction but due to acute reactions, dose was reduced to 200 cGy and he received 54.5 Gy in 23 fractions to penis only. Inguinal nodes were not treated for this patient. Results All three patients achieved adequate tumescence. [Figure - 1] shows a fully tumescent penis in a wax bolus. One of the patients complained of nocturnal erections, which offended his sensibilities. None of the patients developed any other drug-related side effects like chest discomfort, visual disturbance or gastric irritation. All three patients completed the radiotherapy treatment in 39, 35 and 45 days respectively. [Table - 2] shows the acute skin and urinary RTOG adverse events for the three patients. The actual follow-up periods of patients were 23, 53 and 48 months respectively [Table - 3]. Patient 1 developed local recurrence at 10 months from the initiation of treatment. Partial amputation was done as salvage treatment, but later he developed inguinal nodal and pulmonary metastases and succumbed to the disease. The disease-free survival and overall survival for patient 1 were 10 months and 23 months respectively. Other two patients were disease-free at 53 and 48 months respectively. Discussion Tumor hypoxia through altered gene expression and signaling plays an important role in tumor growth, its malignant potential, angiogenesis, invasion and metastases.[15] Reduced apoptosis has also been found as a result of hypoxia.[16] It also imparts resistance to radiotherapy and chemotherapy. Theoretical modeling shows that various regions in the same tumor have different tumor control probability depending on the oxygenation in that particular region.[17] Overall oxygenation status has been established as a strong predictive as well as prognostic factor, particularly in head and neck and cervical squamous carcinomas. The large meta-analysis of 83 randomized trials by Overgaard et al showed that there could be a benefit of addition of a modality targeting the hypoxia to radiotherapy, particularly in squamous carcinomas.[11] One of the mechanisms of hypoxia generation in the tumor is the deficient blood supply relative to the growing tumor mass. As the tumor cells divide, the cells in the inner region move far from the existing blood vessels. Given the limited blood supply and perfusion, these cells get less oxygen and constitute the hypoxic core. This hypoxic core is relatively radioresistant by a factor of 2.5 to 3 - i.e., these cells need 2.5 to 3 times the 'radiation dose required to kill' as needed by the completely oxic cells. Hypoxia in normal tissues (except lung) elicits nitric oxide (NO) mediated vasodilatation. The improved perfusion as a result of the improved blood supply then provides the oxygen requirements, thereby diminishing tissue hypoxia. The physiologic mechanism of erection of the penis involves release of NO in the corpus cavernosum during sexual stimulation. NO then activates the enzyme guanylate cyclase, which results in increased levels of cGMP, causing smooth muscle relaxation in the corpus cavernosum and allowing blood inflow and tumescence. Sildenafil inhibits the enzyme phosphodiesterase, which metabolizes cGMP and thus increased levels of cGMP induce arteriolar smooth muscle relaxation and vasodilatation. Sildenafil induces penile tumescence by improving the blood supply of corpora cavernosa; it is assumed that this increased blood flow, in turn, will reduce the perfusion-limited hypoxia. Sildenafil is rapidly absorbed after oral administration, with maximum plasma levels reaching within 30-120 min. Considering this, sildenafil was given 30 min prior to radiotherapy in our study. In this small study, all patients achieved complete response. Two of the three patients are alive at 48 and 53 months and the other survived for 23 months. The probability of survival for patients with T 2 and T 3 lesion is reported as 50-75%. It is possible that all the three patients in this small series have done well due to radiation-sensitizing potential of sildenafil. Sildenafil-induced vasodilation and perfusion have been found to be effective in Raynaud's phenomenon as well. In a double blind placebo-controlled study of 16 patients,[13] Fries et al showed that Raynaud's phenomenon associated symptoms measured on Raynaud's Condition Score on a scale of 0 to 10 were significantly lower (2.2 as compared to 3, P = 0.38). Capillary perfusion was also measured with laser Doppler anemometer in this study. It was observed that capillary blood flow velocity increased in each individual patient and mean capillary blood flow velocity quadrupled (0.53 versus 0.13 mm/s, P = 0.0004) due to sildenafil-induced vasodilatation. The direct effect of sildenafil on tissue oxygenation has also been studied. Nagdyman et al measured the impact of intravenous sildenafil on cerebral oxygenation with near-infra red spectroscopy in 13 infants after cardiac surgery.[18] A significant increase was observed in oxygenated hemoglobin and total hemoglobin concentration. The mean cerebral tissue oxygenation index improved from 63.4 to 65.7%. In a large series of 105 women with history of multiple in vitro fertilization failures, vaginal sildenafil significantly facilitated the subsequent IVF and successful implantation and improved pregnancy outcomes by increasing the endometrial thickness with its effect of improved blood supply to uterus.[14] These studies showing the effects of sildenafil on increasing the perfusion and tissue oxygenation support our hypothesis of using sildenafil in reducing tumor hypoxia. Sildenafil has not been tried for this indication before. Studies are required to show the effect of sildenafil on oxygenation status within penile carcinoma. Few prospective studies have established the safety of sildenafil.[19] Systemic hypotension is the most common adverse event followed by blurred vision. Its long-term use has been found to cause blindness in some proportion of patients and to increase number of ischemic events in high-risk population. In our study, there was no ischemic event or visual disturbance reported by the patients. By improving blood supply, sildenafil may increase the acute and late local penile tissue toxicity due to its radiosensitizing property. In our study, though, there was no increased acute adverse event with fraction size of 200 cGy. Late toxicities were also not significant. As far as we know, the predictive and prognostic significance of hypoxia in penile cancer has not been studied, probably due to its relatively uncommon incidence. However, the behavior of penile squamous carcinoma can be considered to be similar to other squamous carcinomas - as of head and neck and cervical origin, where hypoxia has been found to impart resistance to radiotherapy and chemotherapy and increase their malignant potential. But application of sildenafil for this indication clearly requires laboratory evidence of prognostically significant tumor hypoxia in penile cancer, its response to sildenafil and validation in controlled prospective clinical trials. Our study is limited due to the small number of patients but nevertheless, it provides a platform for future studies. Co-administration of sildenafil has been shown to be sensible in this small study. The impressive response seen in this small series could be due to sildenafil-induced radiosensitization. One also has obtained a proof of the hypothesis that sildenafil can be a radiation sensitizer in penile cancer. A larger study is required to finally attest the hypothesis. The exact role of sildenafil can be established then only. References
Copyright 2006 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr06030t1.jpg] [cr06030t3.jpg] [cr06030f1.jpg] [cr06030t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}