|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 2, No. 4, October-December, 2006, pp. 171-181 Original Article Dose concept of oncological hyperthermia: Heat-equation considering the cell destruction Szasz A, Vincze Gy. Department of Biotechnics, St. Istvan University, Budapest, Hungary; OncoTherm, Budapest Code Number: cr06043 Abstract We shall assume, of course, that the objective of hyperthermia is to destroy the malignant cells. Destruction definitely needs energy. Description and quality assurance of hyperthermia use the Pennes heat equation to describe the processes. However the energy balance of the Pennes-equation does not contain the hyperthermic cell-destruction energy, which is a mandatory factor of the process. We propose a generalization of the Pennes-equation, inducing the entire energy balance. The new paradigm could be a theoretical basis of the till now empirical dose-construction for oncological hyperthermia. The cell destruction is a non-equilibrium thermodynamical process, described by the equations of chemical reactions. The dynamic behavior (time dependence) has to be considered in this approach. We are going to define also a dose concept that can be objectively compared with other oncological methods. We show how such empirical dose as CEM43°C could be based theoretically as well. Keywords: Cell-destruction, dose of hyperthermia, oncothermia, Pennes-equation Introduction The history of hyperthermia is a few thousand years old. The objective of application of oncology is indisputable: to destroy selectively - if possible - the malignant cells, to eliminate the tumor by heat.[1],[2] The most evident appearance of this concept is the highly local invasive, ablation technique. In spite of the intensive publication activity: remarkable positive evidence-based clinical results[3],[4],[5],[6],[7] and comprehensive articles[8],[9],[10],[11] published on the subject, oncological hyperthermia strives against a number of unsolved problems and the lack of recognition.[12],[13] The deep-heat targeting and control of noninvasive transfer of energy constitute a major share of problems. The fundamental means and condition of the treatment quality shall be the adequate measurability and reproducibility. The control possibility is also an indispensable requirement in the process of the treatment of patients. For that very reason the theoretical discussion and strict biophysical examination of the actually used, mainly experimentally introduced, control parameters and dose concepts cannot be left out of serious investigation. It seems to be of vital importance the definition of hyperthermia object function in oncology. The definite objective to eliminate the malignancy needs clear measurable qualitative goals and its dose quantification. Two main qualities are obviously in consideration: the achieved temperature (measured grades) and the absorbed heat (measured in joule). In our present paper we directly propose to use the absorbed energy (heat) to measure the hyperthermia dose. We disagree to regard the actually reached temperature to characterize the process. According to our position the temperature could only be a possible tool to reach the objective, but must not be a goal. In simple theoretical formulation: if the absorbed energy of destruction purpose increases only the temperature then no energy is consumed to destroy the malignancy, to break off the actual chemical bonds. A part of the energy has to expend for the bond-breaking. This energy will not increase the average energy (temperature) of the tissue; it will be missing from the overall temperature control of the system. Other wording of the argument: if the destruction has a demand of energy then this energy will be absent from the internal energy characterized by the temperature. Therefore, the temperature alone is not enough for the description of the processes taking place at hyperthermia. This is the reason why the hyperthermia characterization extends the temperature measurements by its time-average also.[14] The temperature characteristics and their dynamism at the only temperature change was theoretically discussed by Pennes,[15] in 1948. His formulation describes a non-equilibrium heat-flow when the temperature is the only driving force and only the result of the changes in this picture:
where the ρ, ρb, c, cb, κ, w are the relevant parameters: tissue-density, blood-density, tissue-specific-heat, blood-specific-heat and the blood-perfusion-rate, respectively. Tb, Qm and Qs are the blood-temperature, the metabolic-rate and the energy, which is the heat-sink or source, (in our hyperthermia case it is the absorbed from external sources), respectively. The derivatives are performed by time ( t ) and place ( x ). This equation describes correctly the temperature-dependent part of the heat-flow in the tissue excited by outside energy. The equation is applicable only in the case when not any phase transitions or other energy sink exists, so the distortion phenomenon is excluded. However hyperthermia is devoted to destroy the cells, it is not an only temperature process. Besides the temperature development during hyperthermia, three things can happen with the thermally excited cells:
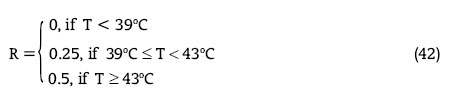
The exact mechanism of the hyperthermia is not known yet, but some widely accepted assumptions could be described. Vascular changes Increase of the temperature causes a general vasodilatation and connected increase of the blood-perfusion in the healthy tissue. At the fever-range temperatures it is the same in the tumors, but in higher temperatures a vasoconstriction happen in certain tumors leading to decreased blood perfusion and suppressed heat conduction,[18],[19],[20] while the trend of vasolidation in the healthy tissues is unchanged, leading to increased blood perfusion and heat conduction in this region.[21] Altered ionic gradients Increased temperatures cause structural alteration in transmembrane proteins causing a change in active membrane transport and membrane capacity[22] leading to substantial changes in potassium, calcium and sodium ion gradients.[23] Moreover, hyperthermia increases biochemical reaction rates[24] and therefore the metabolic rate as well. Often, however, there is not enough oxygen to accommodate the increased metabolic rate resulting in hypoxia[25] and anaerobe metabolism producing lactate[26] and cell destruction by acidosis. Cellular membrane changes It has been long known that hyperthermia can cause softening or melting of the lipid bilayer,[27],[28],[29] it can change lipid-protein interactions[30] and it can denature proteins.[31] All of these events can significantly disrupt a tumor cell′s capacity to divide. The decreasing membrane potential,[32] disrupted cellular function[33],[34] and thermal block of electrically excitable cells[32],[35] could be observed. The osmotic swelling[36],[37] unscratches and could disrupt the cellular membrane. Cellular heat-stress consequences Increased metabolism significantly decreases the cellular ATP stores leading to increased cell destruction.[26] The missing ATP lowers the regular ionic exchange by membrane-pumps, decreasing the pH of the cytoplasm. The decreased ATP-concentration blocks the normal reparation mechanisms of the cell.[38] Increased temperatures can slow down or even block DNA replication;[39],[40] has been hypothesized to have a sensitizing effect of radiotherapy.[41] The hyperthermia induced heat-stress could block essential cellular reactions, recognized in the clinical practice.[42] The heat-stress activates heat-shock-protein synthesis,[43] which anyway exist in high concentration in the malignant cells.[44],[45],[46] This could cause to an effective protection of the cell against apoptosis[47] and can also lead to a multi-drug resistance.[48] Non-thermal effects (mainly electromagnetic field stresses) could also produce chaperone-synthesis.[49],[50] On the other hand, the chaperone HSP70 assists to freeze the actual dynamic equilibrium (the "status-quo") and by expression of the outer-membrane it tries to reestablish the cellular communication in the extra-cellular electrolyte.[51] It is shown that their expression on the cell-membrane gains the apoptotic signals and enhances the immune reactions.[51] HSP participates in the activation of the p53 tumor-suppresser[52] and has been associated with the tumor-suppresser retinoblastoma protein.[53] All the above effects could be temperature-dependent, but energy-consuming also. The individual energy-intake of the above processes will definitely modify the average energy distribution (temperature). Unfortunately, this type of energy-sink is missing from the Pennes bioheat-equation.[15] Pennes created this equation for the examination of blood-stream of human forearm in rest, excluding all the changes which could use energy for something else than the temperature. (He emphasized for the description the equilibrium, fixing the forearm in resting state.) For this purpose Pennes equation is correct and usable, since the internal energy depends exclusively on the temperature, for what numerous model-calculations were provided.[54],[55],[56],[57] To clear the time-dependent transient problems some solutions were published.[58],[59] Some special papers were devoted to modify the Pennes-like equations,[60],[61],[62],[63] but no one had considered the energy taken on the distortion of the actual arrangements. The only temperature investigations (study the average energy), the change of chemical bonds, has no role at all and the energy consumption required for special purposes is not included at all. However, in the case of oncological hyperthermia we have to describe the goal of the treatment: the cellular distortion. Definitely, if the energy could be used only for the chemical changes (distortion of the molecules and restructure the arrangements) then the temperature could remain constant, no energy consumption is made for the average energy-distribution. We have to construct a model resembling better to the reality if we suppose that the internal energy is the state function of not only the temperature T but of other parameters too, which could describe the energy consumption of the structural and chemical changes. The non-thermal parameters have to be measured in-vivo through their measurable consequences (e.g. impedance of the tissue, dielectric constant of the tissue, heat and electric conduction of the tissue, etc.). We are going to refer to these parameters as internal variables of a given cellular composition. Materials and Methods The distortion of the cells and tumor-tissue by hyperthermia is the result of a thermodynamic process. The process is irreversible, so a reaction-diffusion-kinetics is not able to describe it, applying the non-equilibrium thermodynamics is necessary. We are going to describe the principles necessary for the thermodynamical theory of hyperthermia. (i) The state of the examined cancerous tissue can be expressly characterized by the u internal energy (per unit volume) and by the n 1 , nFNx01, n 2 , molar numbers of the intact, the thermally exited and the dead (necrotic or apoptotic way) cell clusters, respectively. For the sake of simplicity, the ionic composition of tissue is considered as constant. (ii) Let us introduce the internal energy of tissue as the state-function of the above state-parameters: u= u (T,n1 , n*,n2 ) [2] (iii) The u internal energy of the tissue fulfils the first-law of thermodynamics:[64]
where Jq is the density of heat flux of thermal conduction, while pe is the heat input of unit volume generated by external actions (in our case, the electric energy heat-input) and the last term is the blood perfusion. This energy-balance is the theoretical basis of the Pennes equation (1) and its various modifications.[65] (iv) We might introduce the s=s(T,n 1 ,n*,n 2 ) state function of entropy, the change of which consists of two parts:
where (v) The external
Carnot-Clausius condition, while for the internal (4) fulfils the Clausius-Duhem inequality:[64]
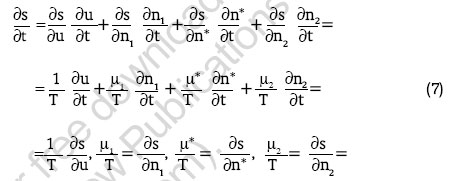
(vi) We apply also the Gibbs- and Maxwell-relations well-known from the stationary thermodynamics:[64]
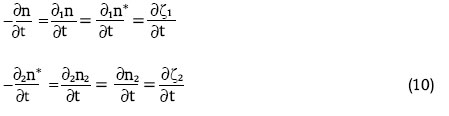
where μ 1, μFNx01, μ 2 are the chemical potentials of the insentient, the excited (by hyperthermia) and the lethally modified (by apoptosis or necrosis) cell-clusters, respectively. For the cell transformation occurring during the hyperthermia process, the intact cells ( A 1 ) have been transformed to their excited ( AFNx01 ) and their lethal (necrotic or apoptotic) ( A 2 ) form. The following formal, reaction equations" could be constructed:
The first equation means that the insentient cancerous cell gets into the A FNx01 excited transient state on the effect of thermal excitation and from this state it might return to its original state as well. The second reaction is the non-reversible cell-death. The κ, κ 1 , κ 2 quantities above the arrows denote the specific reaction rates of processes. The first has a chemical equilibrium, the second hasn′t; it is permanently active till the energy is sufficient for the action. Suppose, the producing AFNx01 is stationer, which happen, if k was much larger than the other two rate-constants, (which is likely in the hyperthermia process). So the production of the excited cells is constantly reproducing the deaths by A 2 ; the decomposition reaction advances with constant velocity. Next, for simplicity, we are going to examine a case like this. Let us define the ζ 1 and ζ 2 generalized reaction coordinates as independent variable. Then, the ∂ζi / ∂t reaction velocities relating to each of the above reactions can be introduced by using the following equations:
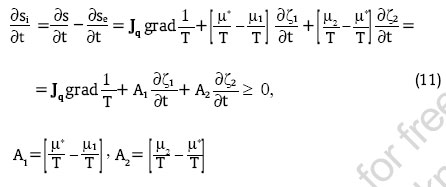
The subscripts 1 and 2 at derivatives denote the process by (8) and (9), respectively. The actual form of entropy production[66] -which is of primary importance in the Onsager non-equilibrium thermodynamics - can be determined from the (3), (4), (5), (7) and (10) equations:
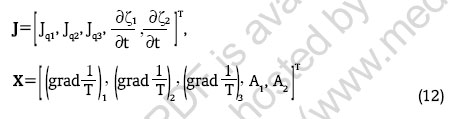
The corresponding affinities are denoted by Ai. Hereby, we have got the entropy production as the bilinear expressions of the
thermodynamical currents ( J ) and dissipative forces ( X ), where T is the symbol of transposition. The expressions of the reaction equations (8) and (9) entropy production (11) allow a process, where there is no heat conduction and the reaction of (8) results in equilibrium, while the (9) does not, namely, the
conditions are valid. (The reaction is performed in isotherm conditions producing constant excited cells in the system.) Instead of the n 1 , nFNx01, n 2 variables, - which are not independent in accordance with (8) and (9), the internal energy and entropy with the independent reaction coordinates have the
caloric state equations. Now, the Gibbs- and Maxwell-relations of (7) are replaced by the following expression:
In order to get the definite form of (14) let us expand the entropy in series and stop at the second term. Then:
Whereas, pursuant to the reaction equation (8) in equilibrium if A 1 =0, thus, from this and from the above relationship we get that
From these we have a unique solution for ζ1 at an arbitrary
With this, the expression of entropy from (16) will be:
Considering that according to the first Maxwell-relation of (15) ∂u = T∂s, we get from the above expression that the partial time-derivative of the internal energy will be as follows:
where ρ is the mass-density, c is the coefficient of specific heat and r 1 , r 2 are the reaction heats of the definite cell transformations of (8) and (9). The material equations of transport processes can be formed by using the Onsager theory. Consequently, the relationship between the thermodynamic forces and currents (12) is linear.[64] In accordance with the Curie theory, only the currents and forces of the same tensor order can interfere,[64] therefore, the Onsager constitutive equations will have the following form:
Here the L mn , (m,n = 1,2) are the Onsager-coefficients, which might also depend on temperature and reaction coordinates. The Onsager theory of the non-equilibrium thermodynamics is not able to bring forward more. The reaction kinetics has to be used for the definition of the form of L mn , (m,n = 1,2). In the interest of a simple discussion we are going to ignore the conduction coefficients of mixed indices, which - in general - can be done as the cross effects are usually weaker than the primary processes. With this, also the coupling of reaction equations will be abolished. We use the
chemical reaction kinetics equation;[67] where R is the universal gas constant. We are going to examine how the above equation can be linearized and, hereby, how it can be harmonized with the Onsager theory. Let us transform the equation as follows:
Then, supposing that the power index of the exponential member is small, let us expand it in series and stop at the second order:
Consequently, the Onsager conduction coefficient has Arrhenius-type temperature dependence, which is well-observed in many experimental works.[68]
In accordance with the above the Onsager material-equations (21), let us consider the
form. Here the conduction coefficients show a dependence again similar to the Arrhenius-law, which has been observed also at hyperthermia.[69],[70] The material-equations (26) can be further concretized if we take the form of entropy (19) and the definition of activities (15) into consideration. Then, we get after some transformations that
Here the τ time constant and ζ 1e equilibrium value of reaction depend on the temperature. Under the excitation the cancerous cells reach an activated level approaching exponentially in a steady-state. The second equation describes the cell-death, which practically means that the cell destruction takes place linearly by decomposition and its temperature dependence is governed by the Arrhenius-law. Results If we substitute the caloric equation (20) and - from (27) - the Fourier-law into the internal energy balance (3) then we have the heat equation valid during the process of hyperthermia:
We have also from (27) the two
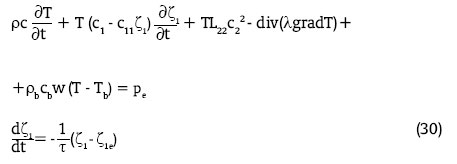
reaction equations. Consequently, if we want to determine the temperature of tissue and the level of cell destruction then we have to solve the system of equations comprising the above three equations, which are coupled because of the coefficients of (29) are temperature dependent. By using the second equation of (29) the equation (28) can be simplified and we get the following equations to be solved:
Discussion The above derived modified system of the Pennes-equation (30) contains already the cell destruction energy, so it provides a full picture about the energy usage. The ζ1 and ζ2 generalized reaction parameters are giving additional terms and an independent equation to the classical, equilibrium Pennes equation. The right way to choose the dose is if we suppose that the relevant quantities are the energy necessary for the cell destruction. This is derived from the expression of entropy production (11). From this, the entropy production resulting from cell destruction is:
And the power dissipation is T-times higher:
The proposed dose can be calculated as the time integral of the power:
If we substitute here the expression of activities from (15) and the kinetic equation (27) we get that the first member is in connection with the activation and the second one with the cell-death.
To make comparison of the dose defined by the entropy with the experimentally used empirical dose at reference CEM43oC, let us examine the form of this dose to the reference temperature of 43oC. In this case the first term of (34) can be calculated in a simple way, so we get:
If we neglect the first term of (35) then - similarly to the CEM43oC empirical dose - we get a dose proportional to the time.
For an other constant temperature this dose has the
form. These two doses are equivalent if
From this, the equivalent treatment-time is:
If the temperature wasn′t constant during the actual therapy (denote its duration by t ), the equivalent treatment time is an integral:
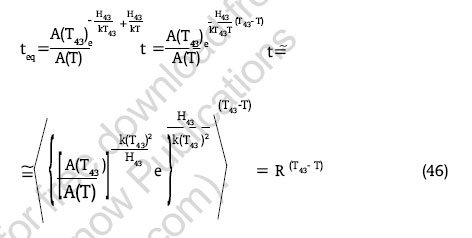
The presently derived thermodynamical dose is connected to the empirical CEM43°C one. Accordingly, if we carry out the treatment under the above conditions at the given temperature then the treatment efficacy can be characterized by the time alone as a dose. In other words: if the temperature is constant and there is no "memory"-effect exists (namely, the system does not change because of the treatment) then the dose can be deduced to the time. The proposed reference temperature is 43°C.[71] (In the English literature this is called CEM43°C). What is the situation in the case of other temperatures?[72] On the basis of experiments carried out on cell cultures - for the comparison with the constant temperature treatment performed on the reference temperature - the following dose function was proposed:[73]
where
This introduction is given from the experimental definitions. ( In-vitro experiments: in the cell culture the same quantity of cell-death shall belong to the given temperature, the dose definition is equivalent.[72] As the base of the measurement is the time, therefore, it basically means the definition of the equivalent time). In this case, practically, the discontinuity kink of Arrhenius-plot has been considered, which results from the different thermo-tolerance. However, we have again three problems:
These conditions could be considered as a "memory effect", because the stimulating force and the real change caused are not simultaneous but of course, are correlating. The solution of the problem is made difficult by the fact that we are not able to find two identical individuals, two identical tumors of the same structure and composition (the tumor is not a homogenous structure), two identical thermo-tolerances etc. The clinical practice can not do anything with these problems. To solve at least the last point, a distribution characteristic had to be introduced instead of the spatial distribution of temperature. This is the temperature for which 90% of temperature values measured in the target is higher, namely, it is the so-called 10th percentile of the measured temperature. Its symbol is T 90 .[81] This is a statistical characteristic which can be specified by using a lot of measuring points under the efficacy of 75% and empirical treatment dose. This is not an adequate matching. By this, we get the definition of CEM43° C T 90 :
Together with its unsubstantial theory, unfortunately, this result correlates slightly with the clinical practice.[82] For the performed experiments the PCR (pathological complete response) has showed 75% correlation with the CEM43°C T 90 in the case of high-grade soft tissue sarcomas treated with thermo-radiotherapy.[82] Large discrepancies could be expected between the empirical dose and PCR in the cases, when the time of the memory effect is not negligible in comparison of the treatment time. To use the in-vivo systems, due to the systemic and other physiological effects this case, the inaccuracy of the empirical dose is unfortunately always valid. The empirical dose-dependence was proven by the canine randomized trial only in low and high dose significance.[83] The redefinition of the thermal dose concept looks as a further step.[84] We have theoretically deduced by very general conditions that the cell destruction reaction rate fulfils the Arrhenius-law. In accordance with this, we are going to show that under certain conditions the Separeto-Dewey empirical formula can be deduced from the Arrhenius-law. Let us start from the isothermal cell destruction of 43°C. Then, the number of destructed cells during t time will be as follows.
Let us take another isothermal treatment of temperature T and examine the section of the same slope of Arrhenius-graph. (Of course, it is quite complicated in the practice as the slope depends on the conditions of pre-treatment.)[76] Let us suppose that for the same degree of cell destruction we need t eq time. As the process is isothermal, we might define the same death rate for the other temperature:[14]
From this we get that
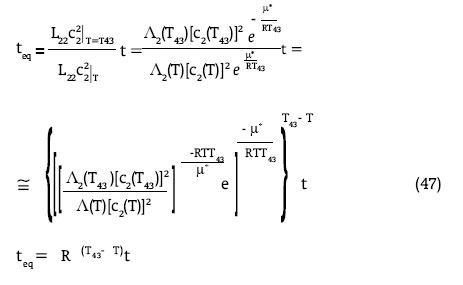
The error of substitution of T temperature with the T 43 absolute temperature corresponding to 43°C equals to ( T 43 - T )/( T 43 )[2]. As this is a very small value, the applied approximation is good. The approximation is not so good if we compare two treatments for which the slope of Arrhenius-graph is different (we should not forget that these in-vitro examinations have not got any in-vivo dynamics). Let us derive the Separeto-Dewey empirical formula from the thermodynamical dose. Start with (39) and considering the Onsager-constants from (26) we get:
This expression is formally corresponding with the equivalent treatment time derived from the empirical dose. So if the energy taken to the activation and distortion is neglected, the energy- and empirical-doses are identical and the parameters have to fulfil the following condition:
This means that the present non-equilibrium thermodynamics describes well the given processes. Also it seems that the present energy dose is more general, it can consider the memory effects of the actual processes and with this fits better to the reality. It is interesting to observe the changes caused by the different factors (pH, low glucose level, thermo-tolerance):[14]
The slope of the lower section of Arrhenius-graph (the section belonging to the higher temperature) will be approximately identical with the slope of the section belonging to the lower temperature. The A proportionality factor changes in the equation (44). In accordance with the above deduction, both effects influence the accuracy of the empirical formula (41). E.g. in the case of thermo-tolerance only one constant will be lower in (42). Regarding the qualitative effect, the jump in the survival graph - which can be observed as a function of treatment time and shows significant deviations for the treatments of different temperatures [85]- will lessen. Additional problem is that in the case of hyperthermia treatment the target temperature is obtained from the solution of Pennes-equation. In this case the temperature distribution is calculated numerically and from this we get the T 90 temperature and the CEM43oC T 90 dose. To verify the temperature the non-invasive MRI measurement is in use,[86],[87] for what presenting the physiological effects (e.g. blood perfusion, heat-tolerance, cell-destruction, etc.) on the applied reference phantoms is problematic. In consequence of the above, the form of the heat-conduction equation (Pennes- or Pennes-like-equation) affects the definition and the definability of the adequate dose. The original Pennes equation does not describe the reality well, does not consider the energy (heat) consumed by the cell-distortion processes. (This cell-disruption however is the main goal of the entire process.) Due to the missing energy, the dose calculated from the Pennes equation is always higher than the reality. The difference between the temperatures calculated from the Pennes equation ( TP) and the temperature derived from our present work could be calculated by perturbation theory as a simples approach. This could be accurate in the case, when the energy intake by the cell-disruption is much less than the overall energy absorption. (Of course this is not an optimal treatment, when most of the energy is not expended to the desired job, but this could be a good approximation of the reality in most of the treatment cases.) Stopping at the first term of the perturbation approximation, the deviation of the real and the Pennes-calculated temperature is:
The difference between the results of the two approximations grows by the relative energy portion of the cellular distortion in the complete energy-intake. If we have a definite high temperature (and the criteriais such a result) then of course we pump the energy much higher than the distortion requests, the temperature in fact only the "non-directly-used" part of the energy-intake. The distinguishing between the "heatable" and "unheatable" patients in reality is the condition that the energy expending to the distortion has to be negligible, ("heatable-patient") so the temperature could be the control parameter instead of the correct energy control. Conclusion Starting by the definition point of the hyperthermia, we considered the energy intake of the cellular distortion during the treatment. The present work proposes to consider the energy expended on the cellular destruction in the frame of the analogue reaction-kinetics. On this base we worked out the non-equilibrium thermodynamic theory of the hyperthermia processes. Results of the above considerations are the generalized Pennes equation and two reaction-equations (one for the activation and one for cellular destruction). Based on the generalized Pennes equitation, we introduced the energy-dose which contains a clinically observable term, the memory effect, namely the effect of the irreversible changes depending on the time, which is characteristically longer (or at least comparable) with the treatment time. We had shown that neglecting the distortion energy, (memory effect) the newly introduced energy-dose and the Separeto-Dewey empirical-dose are identical. This is a control of the new dose-calculation and at the same time shows the reality of the rigorous thermodynamic basis of the empirical-dose as well. By studying the differences between the energy- and empirical-doses, we established that they are near to each other if the energy intake is large enough to neglect the energy of the distortion or the distortion process is so immediate that its time is negligible compared to the treatment time. Considering the definitive task of hyperthermia to destroy the malignant cells, the cell-disruption and the energy expended on this is mandatory in the process. In this regard, our present calculation is important to clarify the quality assurance and all the quality guidelines of oncological hyperthermia. References
Copyright 2006 - Journal of Cancer Research and Therapeutics |
| |||||||||


 [ 3 ]
[ 3 ] 
 denot the entropuy change - the so called entropy production - of the irreversible external and internal processes (e.g. cell destruction, heat-conduction, etc.), respectively. Of course we have to study the entropy changes due to the overall modifications; including the structural-, chemical-, a phase- parameters. Through the change of the entropy, the entire complex process could be controlled.
denot the entropuy change - the so called entropy production - of the irreversible external and internal processes (e.g. cell destruction, heat-conduction, etc.), respectively. Of course we have to study the entropy changes due to the overall modifications; including the structural-, chemical-, a phase- parameters. Through the change of the entropy, the entire complex process could be controlled.