|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 3, No. 1, January-March, 2007, pp. 56-66 Debate Hyperthermia, a modality in the wings Szasz A Biotechnics Department, St. Istvan University, Budapest Code Number: cn07011 Abstract Hyperthermia is a heat-treatment. It is widely used in various medical fields and has a well-recognized effect in oncology. Its effect is achieved by overheating of the targeted tissues. It is an ancient treatment and a promising physical approach with lack of acceptance by the serious medical use. To accept the method we need strong proofs and stable, reproducible treatment quality, but we are limited by biological, physical/technical and physiological problems. However, the main point - I believe - is the incorrect characterization and unrealistic expectations from this capable method. The temperature concept of the quality assurance guidelines has to be replaced by the heat-dose sensitive characterization, pointing the essence of the hyperthermia method.Keywords: Bio-impedance, heat, hyperthermia-treatment, quality-control, temperature Introduction Heat therapy (hyperthermia) is a traditional healing method. It is a treatment using elevated temperature (significantly higher than the usual body-temperature) for cure. The reasons why it could be applied are various: cure of common cold,[1] help in the rheumatic diseases[2],[3] or application in cosmetics[4] and for numerous other indications. Even the first known, more than 5000 years old, written medical report from the ancient Egypt mentions hyperthermia.[5] However, because of the inadequate techniques, the hyperthermia treatment never became a standard in the oncology practice. Despite its long history, the breakthrough of hyperthermia in oncology has remained a dream to be achieved till now. Hyperthermia today, like many early-stage therapies, lacks adequate treatment experience and long-range, comprehensive statistics that could help us to optimize its use for all indications. Nowadays, the lack of acceptance of the oncological hyperthermia has not only statistical reasons; but the technical solutions are not adequate and the quality assurance, the control and standardization of the method itself have not been yet solved satisfactorily. Nevertheless, we will present a wealth of information about the mechanisms and effects of hyperthermia from the scientific literature and our own experience in the hope of proving hyperthermia's worth for further research. Many of the researchers in the field of oncological hyperthermia share the opinion of the editorial comment of European Journal of Cancer in 2001: the biological effects are impressive, but physically the heat delivery is problematic. The hyperthermia results are contradictory, having doubts of the efficacy. The hectic, indefinite results are repulsive for the medical community. The opinion, to blame the "physics" (means technical insufficiency) for inadequate treatments is general in the field of oncological hyperthermia, formulating: "The biology is with us, the physics are against us".[6] In the latest oncological hyperthermia consensus meeting the physics was less problematic. However, in accordance with the many complex physiological effects a modification was proposed: "The biology and the physics are with us, but the physiology is against us".[7] The present situation apparently supports the above opinions. Is the modern technique indeed unable to meet the demands? My objective in this present work is to show the inconvenient parameterization of the oncological hyperthermia and propose those physical effects, which could make easier the harmony of the disciplines, exploring the heart of the oncological hyperthermia as an interdisciplinary topic. (The interdisciplinary- approach is well-recognized in the modern hyperthermia: a special Interdisciplinary Work-Group was established in Germany[8] with the participation of various leading research centers). The state of oncological hyperthermia today is similar to that of radiology at its infancy. When ionizing radiation was first discovered, many hypothesized its usefulness in oncology, yet its exact dose, contra-indications, limits and the conditions of optimal treatment had not been determined until several decades later. This is a natural process: every beginning shows these "symptoms". However, the baby normally has to leave behind the teething-troubles after a definite period. To remain a baby afterwards is abnormal. I think oncological hyperthermia has to get beyond the babyhood, it has to grow up in more definite manner; it has to cast off the infantile period! My present paper tries to provoke a discussion on the development by addressing the question: what is against hyperthermia? Heat dose is not equal to temperature Hyperthermia by its definition is the overheating of the selected tissues. However, the dosing, the selection and the control have significant technical problems, the control of heat transfer deeply into and within the body is a complex issue. To provide reproducibility and standardization of the whole process is mandatory for any acceptance of hyperthermia as a modern treatment modality. A so-called "success parameter" of the efficiency must be established before reliable treatment protocols can be worked out. There is a considerable discussion over the relevant treatment parameters, controls and their optimization. Discussions are primarily centered on the role of temperature and the effects initialized by temperature. In most of the hyperthermia publications, the reached temperature and the provided heat in the targeted tissues are equally used to control and define the actual treatment. My opinion is that this lax definition and slovenly-applied physics are the key-questions of the problems. Interchange the heat by the temperature is physically incorrect. The temperature and heat are two different and definitely not exchangeable quantities in physics. The heat is a kind of energy, which generally may be characterized by the specific absorption rate (SAR) (integrative approach). Microscopically, this energy is depleted by various mechanisms in the actual heating applications. The heat as a physical quantity is an extensive thermodynamical parameter: the heat energy is proportional to the mass/volume/part of the targeted material. In most of the real cases we pump heat (energy) into the targeted system to change its chemical bonds and/or reactions. Hyperthermia in principle uses this energy to destroy the malignant cells/tissue and to reach the definite aim of the treatment. If the energy transfer is correct, then all the pumped-in energy is devoted to make the job: to change the chemical bonds and to destroy the actual biochemical processes in the malignant tissue. The temperature characterizes this process differently: it is an intensive (average) thermodynamic parameter; it characterizes the actual state irrespective of its mass/volume/part. It is a parameter for the control of the local equilibrium (homeostatic state), does not depend on the mass or volume and it has the same value in every subunit. (Note the basic difference from the heat). Let us see a simple example: the body temperature of healthy humans is fairly constant (deviation is less than ±1oC, approx. 0.3%), while the human energy consumption (heat equivalent) varies in a wide range individually (deviation can be more than 100%), even the same individual could have very hectic energy intake depending on the complex conditions (deviation can be more than 50%), with no change in the body temperature. Without notable change in the temperature we are able to pump the energy (heat), mass, volume, entropy (information), etc. into the body. These processes are characterized by the extensive thermodynamic parameters (heat, mass, volume, etc.) identifying the processes quantitatively. Intensive parameters (like temperature, pressure, chemical potential etc.) distinguish the thermodynamical state, describing the actual quality (momentary equilibrium) of the targeted system. Gradients of these intensive parameters are the driving forces of the flow of the extensive ones. The flow of the extensives changes the equilibrium, so redefines the intensives in the system. Let us study a simple steam engine: the applied energy (heat) heats up the system, raises its temperature. However, the engine starts to work only when the water temperature has reached a definite value. From this moment the temperature remains stable, the engine starts to work and the pumped-in heat is converted to the useful mechanical energies, which is the aim of the engine application. If we stop taking away the mechanical energy (block the engine), but the energy intake remains as it was, then the excess energy starts to raise the temperature. The active use of the energy and the rise in temperature of the steam boiler in these conditions are contradictory. In oncological hyperthermia, the absorption of energy is a complex process. If the malignancy has only a single chemical bond to destroy, then our job would be to deliver the corresponding breaking energy (resonant frequency). Breaking of a definite bond consumes the energy; no temperature change would be created. The temperature rises only when no direct action on the energetic chemical bonds is possible, consequently, an average energizing of the area could solve the breaking without targeting any specified structures. However, when the anyway unknown breaking energy is reached by this average, then the energy is suddenly pumped into this process and till the end of the job no temperature change can be observed. This phenomenon is called phase transition, which is definitely measurable by the heating dynamism. Exactly, the phase transition idea was used to prove the temperature concept of hyperthermia in oncology. There is a cellular phase transition observed around 42.5°C[9] and the dynamic measurement (Arrhenius plot) fits surprisingly accurately to the experimental results.[10],[11] However, the definite phase-transition temperature (Arrhenius kink) changes by the chemotherapies,[12] it strongly depends on the heating dynamism (slow and rapid)[13] and on the pre-heating conditions.[14] These facts contradict any phase-transition concept. Furthermore, there are other observations leading to recent doubts about the deterministic role of the temperature.[15] Interesting also that the thermal enhancement ratio (TER) increases linearly with the activation energy,[12] so the phase-transition concept as an explanation of the step-down heating[14] cannot be valid. Physiology of the target is always present and deeply changes the conditions. This physiologic modification is well shown by measured differences invivo and invitro .[16] The physiological conditions are so effective that the drastically increased forwarded power (from 450 W to 900 W) in fact does not improve the measured temperature and it varies roughly patient by patient.[17] Because of the physiological factors, the heat-treatment success depends on the dynamism of the heat delivery.[13] Furthermore, measurements show that the tumor temperature is not significant by applying pretreatments and/or incubations.[16] The experience in radiotherapies - where the isodose curves can be introduced - is the incorrect adaptation for hyperthermia treatments. Due to the active physiological influence, the isothermal curves are unscientific dreams in the living tissue. From the point of view of heat doses, the tissue is incomparably more inhomogeneous than in the case of the ionizing radiation. The ionizing radiation is energetic enough to neglect the thermodynamic differences in the tissue; however the hyperthermia essentially acts on the thermodynamically relevant parameters. Anyway, the dose in radiology (the gray [ Gy ] (=10 -2 rad ), which is the absorbed energy pro mass (energy-density, [ J/kg ])) is clearly an extensive parameter and corresponds to the heat dose (SAR) applied in hyperthermia. Accordingly, the adequate parallel characterization to radiative dose is the absorbed heat and not the intensive (equilibrium like) temperature. (The intensive temperature in hyperthermia might be parallel to the breaking energy of molecules by ionizing radiation in radiology. It is obvious, that this breaking energy cannot be used because of the large variety of molecules). All the medical treatments are quantitatively characterized by the extensive (never by intensive) thermodynamic parameters. The radiotherapy uses Gy ; the chemotherapy uses the chemo dose, (mass of the active agent pro mass of the target/[body mass/body surface]); surgery uses the volume and/or the mass; etc. From this point of view only the hyperthermia is the exception for the time being: there is not any other medical application, which uses intensive parameter to control any processes! The incompleteness of the intensive parametrization in hyperthermia is well shown also by the necessity to control two other characteristic parameters: the time (The time by power would be the delivered energy; but time by temperature as used in the hyperthermia practice, has no physical meaning) (how long we are able to keep the given temperature, generally defined as a proportion of the actual treatment time) and the information on the temperature distribution (The temperature distribution is basically influenced by the local physiology-determined processes, like the metabolic rate, the blood perfusion and the other conductive and convective processes). (or quantities describing which portion of the tumor was over the given temperature or measurement of the minimum and maximum temperature in the lesion) as well. The doubts are well-supported by the fact that the uniform and high temperature in the tumor (near the physiological threshold of 42oC) caused by extreme whole body hyperthermia (WBH) has not resulted in better results than the locoregional heating with lower temperature average and with very heterogeneous temperature distribution. Application of lower temperatures (mild-WBH) for treatments of longer periods (keeping the dose) also showed surprisingly good efficacy.[18],[19] This finding supports the opinion that the delivered heat dose[20] (absorbed energy) or applied field[21] (electromagnetic influence) may determine the treatment efficacy. It is also important modification that, recently, numerous scientific theories have also started to concentrate on the significance of thermally induced non-thermal effects,[22] such as heat-shock protein (HSP) production.[23] The relevance of tumor temperature, heat dose, nonequilibrium and nonthermal effects is apparent and leads us to the conclusion that clinical outcome cannot be determined purely on the basis of any of these factors alone. Dynamical description The healthy living state is in a dynamic equilibrium (homeostasis). The malignant tissue is not in equilibrium as its progress is permanent. Unfortunately, the temperature as an intensive thermodynamic parameter is not enough for the proper control of such dynamic system [Appendix 1]; even it may mislead the user. Heat put into a system (ΔQ ) plus work done on a system (ΔW ) is equal to the increase in internal energy of the system (ΔU ), (first law of thermodynamics:[24]) ΔU=ΔQ+ΔL (1) Sign Δ means a small change. During this small change the system does not alter (quasi-static approach). In a more rigorous description a differential calculus has to be used. Eq. (1) shows that the internal energy U is determined by the energy exchange. This exchange has various forms, all the available interactions (denote their number by n) has to be calculated. These terms can be easily defined by the pair products of intensive ( Yi) and extensive ( Xi) parameters:
For example some of the terms are:
where T, S, p, V, Φ, e, E, P, H, M, α, s, f, l are the absolute temperature, entropy, pressure, volume, electric potential, electric charge, electric field, electric polarization, magnetic field, magnetization, surface tension, surface area, linear force, length, respectively; while Nj and µj are the number/mass and chemical potential of the various ( k ) particles (molecules, ions, clusters, etc.) in the system. Many other pair interactions (all the energetic terms) may be included in this energy balance. All the pairs have special biological meanings: TΔS is the absorbed heat, pΔV is the work of pressure (volume changes), Φ Δe is the work of the moving electric charges, (E·ΔP) and (H·ΔM) are the work of the electric and magnetic fields, µjΔNj are the terms of the chemical reaction energies of various ( j=1, 2, 3, .,k ) species, αΔs can be the energy of the surface (membrane) changes, fΔ-l could be the work of the muscle-fibers, etc. Only one of the terms, the heat energy has temperature, all the other terms are other kinds of energy consumptions. Definitely, if there are not any structural, chemical, etc. interactions in the system, only the heat is absorbed, than (1) has no ΔL term:
where To is the original body temperature [ Co], c is the specific heat [ J/kg/K ] giving that how much energy is required to heat up 1 kg tissue by 1 K, ρ, V and m are the density [ kg/m 3 ], the mass [ kg ] and the volume [ m 3 ] of the heated tissue, respectively. ÄQ is the delivered energy [ J ] into the heated tissue. This picture could be the basic of the misleading interchange of the heat dose and temperature change; in (5) there are proportional. Do not forget, (5) is only valid if there is not any other interaction than the heat absorption. Of course, this is not the case at all in hyperthermia, where our goal is definitely to change the structure and the bio-chemical constituents. In the study of (5) it is also important, that the time (dynamic effects) is not included in these static considerations. However, if the energy balance is time-dependent (the heat delivery and heat sink have power-like relations, [ J/s ]), then the temperature becomes also time-dependent. The thermodynamical energy balance defines the actual heat exchange:
the energy change in time (δU/δt), its flow in space
is: div(I U )=Σ(δI U /δx i ) and
its sources q U =q e +q m +q b ,
where I U is the energy current density, q e , q m and q b are
the energy source/sink from electric, metabolic and blood perfusion origins,
respectively. The well-known balance equation[25] is: As it is well-known from,[26] the current density of the heat flow is proportional to the temperature gradient (heat diffusion):
By substituting (7) into (6) we obtain the so-called bio-heat (Pennes-) equation[25] which serves for the description of tissue heating and internal energy transport. It has the form of
where T is the temperature of tissue; ρ and c are the mass density and the specific heat of tissue, respectively; λ is the coefficient of thermal conduction; ρb c b v b is the blood perfusion; T b is the blood temperature (this term is in fact a negative value at the loco-regional treatment, namely, it is a cooling term owing to T b < T; while in the whole body treatment it will be positive). The q m term is determined by the metabolic rate ( M ) and the mass density: q m =ρM. The metabolic rate grows by the temperature gain ΔT: q m ~1.1ΔT ;[27] therefore, in the case of 6 ° C increase, the amount of growth will be 1.8-times. The metabolic heat production of tumor depends on the doubling time of its volume,[28] so it is determined by the speed of the development. Defining qe is more complicated because it needs an approximation of the energy absorbed from the electromagnetic fields. In real situation the bio-electromagnetic interactions are more complex and the measurement of the absorbed energy is necessary. The energy absorption is characterized by the specific absorption rate (SAR, [W/kg]), identifying the absorbed energy in unit mass:
where E local is the locally presented electric field in the tissue and σ is the electric conductivity. The solution of the partial differential equation (bio-heat equation) (8) should be reasonably given numerically because of the following arguments:
The unanimity conditions of the bio-heat equation (8) are the initial data and boundary values. The initial data can be easily specified by the actual initial body temperature ( T o ), assuming its homogeneity in the malignant area and its surrounding. (Note: sometimes it is not the case because of the higher tumor temperature because of its increased metabolic rate). However, the boundary conditions (which are essential to solve (8) at least numerically) are more complicated to determine. Three types of boundary conditions may be considered:
These conditions - with the additional problem of knowing the SAR distribution in situ - clearly show that the solution of bio heat equation does not realistic for practical use. However, let us note the actual driving forces in the equation, which are always the temperature changes (gradients in space and time) and no assumption of the homogeneous temperature can be valid. (In the case of homogeneous temperature the bio-heat equation (8) does not exists). A generalized, more rigorous approach supposes that the internal energy as the function of many observable parameters (internal, invivo variables) does not depend only on the temperature.(Ruling out the sole temperature dependence of the bioheat equation modifies the picture of the phantom-calibrated temperature measurements as well). Consequently, the bio-heat equation[29] has to be further developed. The basic ideas of the modification are: (i) State of the studied tissue could be unequivocally characterized
by the volume-specific internal energy (u) and by qi (i=1, . n) additional
internal ( in vivo ) variables. the qi variables: (iii) The internal energy satisfies the energy-conservation (first law of thermodynamics:[25]
p = pe + pb + pm (13) (iv) The entropy function s(u,qi) characterizing the state
has two parts: where (v) The
and the Clausius-Duhem inequality[25] is valid for the second term of (14):
(vi) The Giggs relation from the equilibrium thermodynamics[25] is applicable:
The actual form of the entropy production (as the central point of the Onsager's nonequilibrium thermodynamics) is determined by (12), (14), (15):
(18) is the entropy production expressed by the bilinear expression of the
thermodynamical currents and dissipative forces: where T denotes a transposing. In case of reversible processes, from (18):
Indeed, the two first terms of the entropy-expansion: and due to the reversible processes from (20):
This equation is valid for all the reversible processes, so c i =0 for any of the c coefficients. Hence, from the character of the entropy function using (22) we get the system of equations:
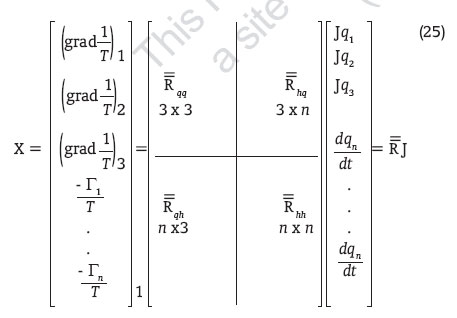
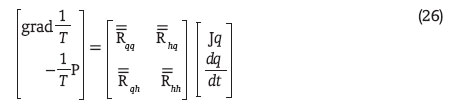
which has to have an univocal solution, which is obviously q i =0 . With this, the only temperature dependence of the entropy for reversible processes is proven, all the other internal variables are zero. However, in general case (including non-reversible realities) from the entropy expression (21): where Let us discuss the material equations. According to the Onsager's theorem,[25] the thermodynamical forces and current densities (expression (19)) are linearly proportional:
where
when using (17) and (24), we get the system of matrix differential equations:
These equations are equivalent with the equations
where
where we supposed that the whole process has started from an equilibrium state (q(0) = 0). It could be shown by applying the Bendixon theorem on the positive definite matrix that the homogeneous solution of the matrix differential equation satisfies the following condition:
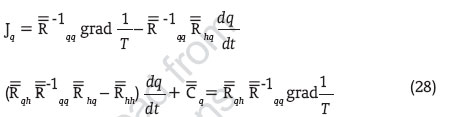
Consequently, (29) shows that the internal variables are functions of the temperature and are functionals of the temperature gradient. This last statement means that all the internal variables depend on the history of the temperature gradient and cannot be regarded as a simple and sole function of the temperature. Hence all the (T, q1,..,qn) thermodynamical variables might be expressed by the temperature and by its gradient but depend on their history prior to the actual studied state. Consequently, the temperature is not enough to characterize the process and the system; its measurement alone is not enough to control the treatment. Substituting (29) into the first equation of (28) we get the material equation expressed by the observable material parameters:
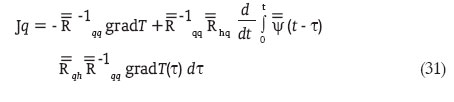
which is in fact the generalization of the Fourier theorem. Let us
suppose that the tissue is isotropic, then instead of
which shows again the history dependence of the temperature gradient. The change of the internal energy according to the Gibbs relation (17)
can be determined from the entropy. Equation (33) clearly shows that the specific heat of the tissue is not enough to determine the internal energy (absorbed heat) dependence on the temperature, consequently, the specification of further material characteristics is necessary. With regard to the equation (29) it is clear that the internal energy depends not only on the temperature, but on the temperature gradient as well, therefore, its characterization is impossible by the temperature alone. If we suppose a stationer (dynamic equilibrium, homeostatis) state at the heating, we get the form (28) of the usual Fourier heat-conduction theorem. (The conduction coefficients are definitely different from the static solution, because the temperature gradient dependence). In this state, according to (33), the change of the internal energy equals to zero. If we substitute these into the energy-conservation equation (2), then the trivially obtained equation is formally identical with the bio-heat equation.[29] So in stationer (equilibrium) case the whole process could be described by the temperature alone of the equation (5), using the well-known methods from the relevant literature. We can automatically raise the question: how we might reach the stationary, equilibrium state? The answer is disappointing: there is no how! Let us simple start from the simplified expression of the absorbed electric power:
where E is the actual electric field strength and σ is the conductivity of the tissue. Due to the expected cellular distortions this last term (as many of the hyperthermia experiments show)[30],[31] depends explicitly on the time. Consequently, in every cases when the (34) electric power is not constant, the source term of (12) internal energy balance depends on time, there is no way to construct any stationary (equilibrium) conditions, so again, the process can not be determined by the temperature alone. So the further developed bioheat equation can be created by substituting (29) into (33) and by substituting the obtained result into the internal energy balance (12). Also the generalized Fourier theorem (32) and the specific heat power (34) have to be substituted into this balance equation. Due to the definite time-dependence, the equations became nonhomogenic; the process cannot be controlled by the temperature alone. In the case where no cellular distortion and/or other cellular/tissue changes take place and only the general temperature rises without other changes, the temperature characterization is definitely correct. However, this process does not cure, simply heats without the expected hyperthermia effects. The problem of the widely and incorrectly applied Pennes bioheat equation[29] is not the fault of the original publication. That was correct regarding the analysis of the tissue's arterial blood temperatures in the resting human forearm. In that case no cellular/tissue changes are expected, the stationer (homeostatic) case trivially exists, even the author emphasizes this equilibrium by the investigated "resting" cases. Have we any reason, why hyperthermia uses intensive thermodynamic parameter (temperature) regarding the quasi-equilibrium of the treatment? No, of course, we have not. It is only the historical "bad habit". This bad characterization is mostly responsible for the contradictory results, for the loss of comparability of the results, for the blame of physics/physiology! Appropriate parameterization According to our view, the hyperthermia (definitely it is heat-dose treatment) is temperature-dependent but not temperature-determined process. The temperature concept is not bad as long as the physiological factors (blood flow/vascularization, metabolism, chaperone-protein production, dissemination, apoptotic action, etc.) are included and the tissue can be regarded as homogeneous, semi-isolated from the surroundings. Unfortunately, these conditions are not common, so sometimes the temperature gives statistically significant, sometimes random results. This is the reason why some trials check the patients before, dividing them on the "heatable" and "notheatable" groups,[32] randomizing for trial only the previous group. For this group the anyway scientifically incorrect and assumed equivalence of the heat dose to the temperature is an acceptable approach. On the other hand, this preselection excludes a large number of patients receiving hyperthermia; however, this treatment could help them as well. The exclusion was made on an insufficient characterization of the method. A relevant characterization of oncological hyperthermia for quality guidelines has to be started from the aims: it is to destroy the malignant cells! This demand contains some more precise requests: act selectively on the malignant cells, block the further proliferation and stop the dissemination of tumor-cells. Distortion could be promptly direct (the cells become necrotic during the treatment) or indirect (tune killing conditions; the cells become necrotic or apoptotic after the treatment). The demands actually do not contain any temperature request. The desired temperature could be a tool to manage the process; but the goal never should be replaced by any actually applied tools. The appropriate characterization has to be a definite adverb of degree: characterizes the process, determines the actual state, measurable and repeatable. Usually we have to measure the state of the actual process and not the status of the tool; so the distortion process it self is the measurable target. The prompt effects during the treatment seem to be easier to measure, it is really a quantitative factor, but to measure the conditions for the effective distortions afterwards needs assumptions. Changes supposed to make some postponed actions (ischemia /hypoxia, stress factors, acidosis, etc.) also measurable in situ . With the temperature concept (using it like an aim and not like tool) the assumption is very simple: the suitably high temperature does all the jobs, the prompt and the postponed effects can be expected, the requested thermal dose is reached in the target. As we see from (3), the temperature dependent term ( TDS ) in the internal energy (DU ) is the only one from many others. The main factor of the real desired action: to have cellular distortion, to have chemical reactions. If the bio-system undergoes chemical reactions, the nontemperature parts of the internal energy become important.[25] A spectacular measurement shows experiment, when the same temperature is reached by conventional and microwave heating and the reaction is significantly different.[22] (For example: at equal 25 oC we may observe fourfold difference in the values). In spite of its inadequate character, the temperature had gradually become the base of the quality assurance and treatment control. I think it is time to change and choose a heat-dose (energy dependent) characterization. There are various possibilities to choose such parameter, but I think, the physiologically and physically well-studied ionic environment offers the best. This environment depends on the metabolic rate, on the chemical reactions and on the structural changes as well. (Sure it is also temperature dependent by these extensives). The ionic density and the structural changes could be well followed by the complex impedance (its imaginary and real parts), which in this meaning is a perfect candidate to control the energy-induced distortion-processes. Electric bio-impedance is a well-known method and a simple electrical measurement technique.[33] It measures the tissue's specific electric field distribution. The measurement uses the special frequency dispersion of the actual tissue. As early as 1940 both the whole-body electrolyte status[34] and the local changes (ECG)[35] were studied by the method. Nowadays, it is widely applied and for breast tumor diagnostics received the FDA approval (4/16/1999). Which effects could be used for characterizing?
The approach using electric impedance for quality assurance is partly comparable with the ion- concentration concept of ionizing-radiation characterization: the old unit measured the ion-pair production, 1 R ( roentgen ) = 2.58FNx0110 -4 C/kg . Recently, scientists have started to realize that hyperthermia-induced temperature gradients (driving force of the dynamic effects) could have significant biological role. A new branch of hyperthermia known as extracellular hyperthermia[66] or electro-hyperthermia[21] has been developed around this concept. Although this new technique recognizes the benefits of increased tissue temperature and its biological consequences, it also argues that nonequilibrium thermal effects are partially responsible for the observed clinical deviations from the purely temperature based treatment theory. Conclusions, perspectives Hyperthermia is an emerging effective treatment method in oncology. It has shown significant improvements in tumor response rates and patient morbidity in combination with other treatment methods, such as surgery, chemotherapy, radiation therapy and gene therapy or applied as a monotherapy. Nevertheless, hyperthermia is still in its infancy. It lacks standards and a scientific consensus about its effects on malignant and healthy tissues and the current techniques used to treat patients vary significantly from the antenna array focused electromagnetic energy delivery methods to nonthermal low-power current applications. In order that hyperthermia shall gain widespread approval and clinical use, the technique requires extensive further research and standardization. For this we need an open mind and to outgrow the dogmatic habits. What / who is against hyperthermia treatments? Nothing / nobody from outside. We are against ourselves constraining the temperature concept over all. The physics, biology and physiology are with us if we make a correct approach. Appendix I Specific values (densities, ρi) can be introduced for any of the extensive values as a basis. (Intensive parameters [like temperature, pressure, etc.] have no density, they characterize the actual state). Practically, the volume based [density pro m 3 ] (ρi(V)) and the mass based [density pro kg] (ρi(m)) ones are in use.
So the internal energy densities from (2) are:
where The well-known continuity equations for every density contain the current density of the flow of actual extensive (j i ) and the source, if any, (q i ).
For the particles/masses we have no source (conservation law) and with the actual speed (v i )
If the diffusion is also included, it acts like a source:
where D is the diffusion constant and Δ is the Laplace operator:
In the irreversible thermodynamic changes (dynamic, dissipative process) the entropy characterizes the direction: the total entropy of the system always increases. (It is the second law of thermodynamics).[24] Consequently, the isolated system always seeks to eliminate the gradients of the intensive parameters (for example the temperature, the pressure, etc. always try to equalize). Introducing the thermodynamic potentials (every intensive is divided by the temperature:
Furthermore, all the driving forces depend on the gradient of the extensive densities (derivative identity):
So, all the extensive parameters tightly interact in the thermodynamic processes, therefore for the description to keep in hand, all the thermodynamic extensives are crucial. References
Copyright 2007 - Journal of Cancer Research and Therapeutics |
| |||||||||













 [
[