 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
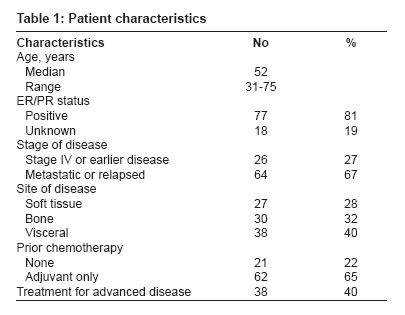
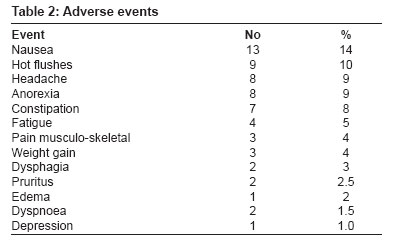
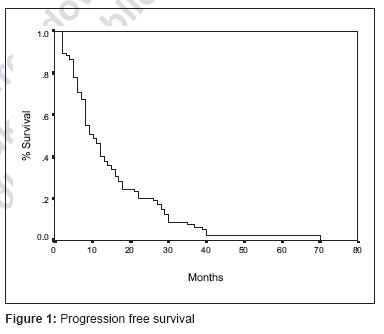
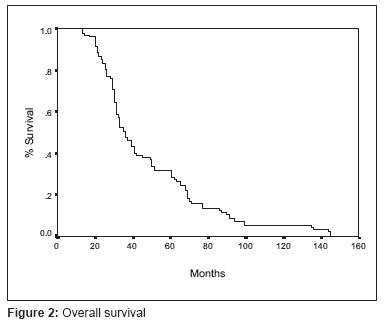
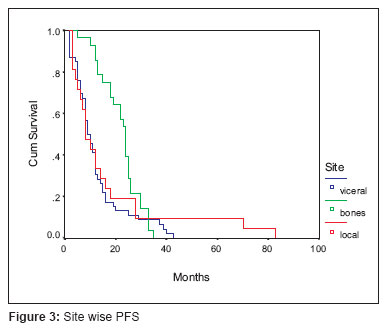
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 71-74 Original Article Results of letrozole in postmenopausal women after tamoxifen treatment for advanced breast cancer BS Yadav, SC Sharma, FD Patel, S Ghoshal, V Kapoor Dept. of Radiotherapy, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012 Code Number: cr07019 Abstract Aim : To analyze overall and progression-free survival after letrozole in postmenopausal women with advanced breast cancer who failed after tamoxifen therapy.Materials and Methods : This is a retrospective analysis of 95 patients with breast cancer who were postmenopausal and had failed after tamoxifen therapy. Dose of letrozole was 2.5 mg daily until disease progressed. Patients had estrogen receptor-and/or progesterone receptor-positive tumors or both receptors were unknown. One complete course of (6cycles) chemotherapy for metastatic disease was allowed. The primary end point was time to progression (TTP). Secondary end points included overall objective response rate (ORR), its duration, time to treatment failure (TTF), overall survival and tolerability. Results : Median TTP was 10 months. ORR was 21% with complete response rate of 9%. Nine patients died of disease during treatment. Median overall survival was 36 months. Median time to response was three months and median duration of response was 13 months. Time to chemotherapy was 13.5 months and TTF was 9.3 months. Treatment failure was seen in 76% of patients. Disease progression was the main cause for treatment failure. Treatment was well-tolerated by all patients. Conclusion : This retrospective analysis shows that letrozole is quite effective as second line therapy in postmenopausal patients with advanced breast cancer who had failed after tamoxifen therapy. Keywords: Letrozole, postmenopausal, tamoxifen and breast cancer Introduction Advanced breast cancer in postmenopausal women remains an incurable disease and so treatment is aimed at palliation and improved quality of life. For more than 20 years, tamoxifen has been the established standard of care for first line therapy in postmenopausal women with advanced breast cancer considered eligible for endocrine therapy. [1] Such therapy is well tolerated than cytotoxic chemotherapy and is at least as effective in stopping of slowing tumor growth. Response rate of between 30% and 45% have been reported for first line therapy with tamoxifen as well as with other hormonal agents such as non-specific aromatase inhibitors aminoglutethimide or progestin, medroxyprogesterone acetate and megestrol acetate. [2],[3] But neither progestin nor aminoglutathimide are superior tamoxifen in efficacy of tolerability. [4],[5],[6] In patients with breast cancer whose tumor progress after tamoxifen can be benefited with selective and potent aromatase inhibitors, such as letrozole, which has also shown superior efficacy and tolerability to megestrol acetate and aminoglutethimide. Response rate for these agents used in second line therapy range from 8% to 24%. [7],[8],[9] Two trials comparing anastrozole with tamoxifen have been reported. The North American study demonstrated superior time to progression (TTP) for anastrozole over tamoxifen, but no benefit in other primary end point objective response rate (ORR). [10] However the larger tamoxifen or anastrozole randomized group efficacy and tolerability trail failed to show any improvement in TTP with anastrozole compared with tamoxifen. [11] Combined analysis of the two trials failed to show any significant difference between tamoxifen and anastrozole groups for any of the major end points. [12] A randomized phase III trial of letrozole versus tamoxifen in postmenopausal women with advanced breast cancer had shown letrozole to be significantly better than tamoxifen in terms of TTP, response rate, rate of clinical benefit and time to treatment failure (TTF). [13] Longer follow-up of the same trail also show superiority of letrozole over tamoxifen. [14] In this retrospective analysis we report results of letrozole as second line therapy in postmenopausal women with advanced breast cancer. Materials and Methods Postmenopausal women with advanced breast cancer or metastatic measurable or assessable disease were given letrozole 2.5 mg daily until the disease progressed. Patients were required to have tumors with ER- positive or PR-positive status or with both receptors unknown. ER/PR positivity was seen in 77(81%) patients and it was unknown in 18(19%) of patients. One complete course (6 cycles) of prior chemotherapy was permitted provided progressive disease was documented. Chemotherapy regimens used were FAC (5-Fu 600 mg/m 2 , adriamycin 60mg/m 2 and cyclophosphamide 600 mg/m 2 ) who had received CMF previously and paclitaxel (175 mg/m 2 ) and epirubicin (80 mg/m 2 ) if previously treated with FAC regimen. All the patients were given tamoxifen till recurrence or metastases. Those patients who had evidence of brain metastasis, bilateral diffuse lymphangitis carcinomatosis of the lung with more than 50% lung involvement, more than one third liver involvement on ultrasonography and or on computed tomography scan, inflammatory breast cancer, concurrent or previous malignant conditions (except for contralateral breast cancer or adequately treated basal cell or squamous cell carcinoma of the skin) were excluded from the analysis. Adjuvant endocrine therapy other than anti- estrogens and prior systemic endocrine treatment for advanced disease was stopped before letrozole therapy. Patients on concomitant anticancer treatments, prolonged systemic corticosteroids and on bisphosphonate therapy for prevention of bone metastases were excluded from the analysis. Bisphosphnates are not routinely used in our institute; they are used in patients with disseminated bone disease. The site where radiation was given was monitored for progression but not for response assessment. Assessment of efficacy and safety Secondary end points included ORR, duration of overall response, TTF, time to response, number of deaths and overall survival. ORR was defined as the proportion or patients who achieved a CR or a PR confirmed by a second evaluation at least one month but generally three months later. TTR was defined between start of therapy and earliest documentation of response. TTF was defined as the interval between start of therapy and earliest date of PD, loss to follow-up death from any cause. Duration of OS was defined as the interval between start of therapy and death for any reason. Safety was assessed through monitoring and recording of all adverse events using the National Cancer Institute common toxicity criteria (version 1.3). Statistical analysis Results A total of 95 postmenopausal women with locally advanced or metastatic breast cancer, who failed on tamoxifen and were started on letrozole 2.5 mg between January, 2001 and November 2004, were analyzed. Patient characteristics are given in [Table - 1]. At the time of analysis 67% patients had metastatic disease 27% had locally advanced disease and 6% had local as well as metastatic disease. Soft tissue lesions were present in 28% of patients, bone metastasis was present in 32% of patients and visceral involvement was seen in 40% of patients. Liver and lung metastasis were seen in 12% and 10.5% of patients respectively. Sixty three percent of patients had received prior chemotherapy. Second line chemotherapy with FAC regimen was given to 29 (30.5%) patients and paclitaxel and epirubicin to nine (9.5%) patients. Palliative external beam radiotherapy was given to 66% of patients at painful sites. Median TTP was 10 month and median overall survival was 36 months. ORR was 36% with CR in 9% of patients. Median time to response was three months and median duration of response was 13 months. Time to chemotherapy was 14.5 months and TTF was 5.3 months. Treatment failure was seen in 76% of patients. Disease progression was the main cause for treatment failure. On further subgroup analysis progression free survival at two years was 39% for patients with bone metastases, 20% for local recurrence and 13% for visceral metastases. This difference was statistically significant ( P =0.017). However over all survival was not different among three groups. Main adverse effects seen were as shown in [Table - 2]. Discussion Five year tamoxifen is still considered the standard approach for postmenopausal or ER/PR positive patients with breast cancer. [15] Longer duration of tamoxifen has not shown to be beneficial and have been associated with increased risk of tamoxifen induced endometrial cancer and thromboembolic episodes. [16] Significant proportion of breast cancer recurrences (40-50%) occur more than five years post surgery. [17] Taken together these observations provided a rationale for the assessment of other agents which demonstrated efficacy in breast cancer such as aromatase inhibitors. Letrozole has already been proven better to tamoxifen as first line therapy in ER/PR positive or postmenopausal women with breast cancer. [14] This retrospective analysis also show letrozole to be quite effective as second line hormonal therapy in postmenopausal patients with locally advanced or metastatic breast cancer who had failed on tamoxifen. Response rates are modest. Median TTP (10 months, [Figure - 1]) and median overall survival (36months, [Figure - 2]) are comparable to that reported in literature. Many of our patients (40%) had visceral metastasis, which is less responsive to hormonal therapy. Still the complete response rate (9%) is similar to that reported in other studies (8-24%). [6],[7],[8],[9] The first reported study of letrozole 2.5 mg and megestrol acetate 160 mg showed letrozole superior for multiple efficacy end points, including ORR, duration of response, duration of clinical benefit, TTF and tolerability. [9] Subgroup analysis showed better progression free survival in the patients with bone metastases [Figure - 3], this may be because disease progresses very slowly in the bones and the other factor is that it responds to hormonal treatment better as compared to soft tissues and visceral disease. It has been seen that local recurrence is also a hallmark for distant metastases that is why these patients do not have better progression free survival. Adverse effects were more or less similar to tamoxifen as shown in [Table - 2]. The therapy was well-tolerated by all patients. None of patients refused for taking the drug due to any of the reported side-effects. As the compliance with the drug is good it is a good alternative for postmenopausal patients with local recurrence and bone metastases, particularly for patients with poor general condition and those who cannot afford costly chemotherapy drugs. It is not toxic as compared to chemotherapy. This fits well in Indian scenario as patients can stay home on the drug, need not travel long distances as for chemotherapy. A limitation of this study is that it is done retrospectively and retrospective data is not always complete. The other limitation is small number of patients. This is first experience from our institution. Conclusion Letrozole shows evidence of clinically relevant benefits and good tolerability profile, hence should be offered as second line hormonal therapy for the treatment of advanced breast cancer. Patients with bony metastases are benefited the most.References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07019t1.jpg] [cr07019f3.jpg] [cr07019f1.jpg] [cr07019t2.jpg] [cr07019f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}