 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
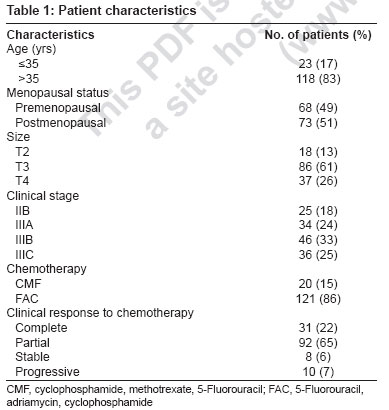
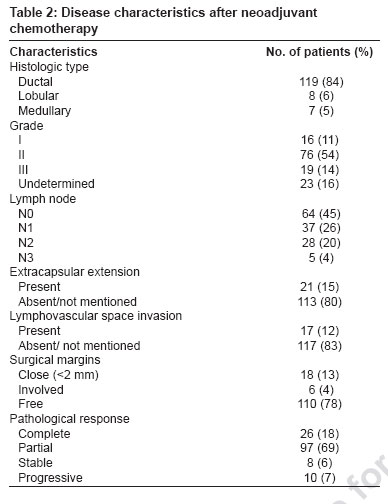
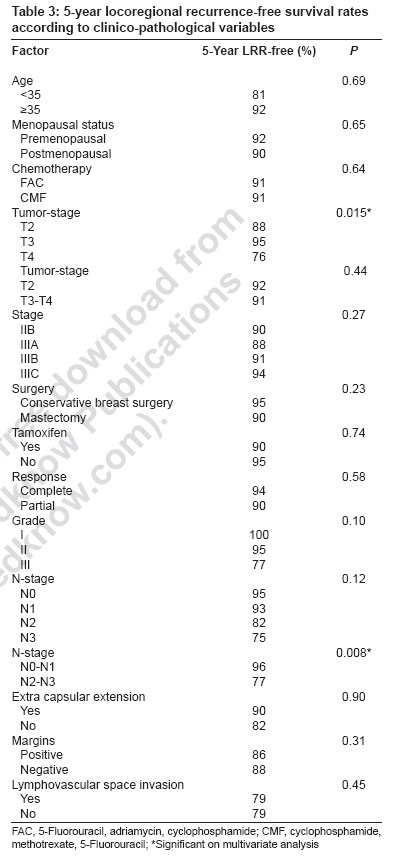
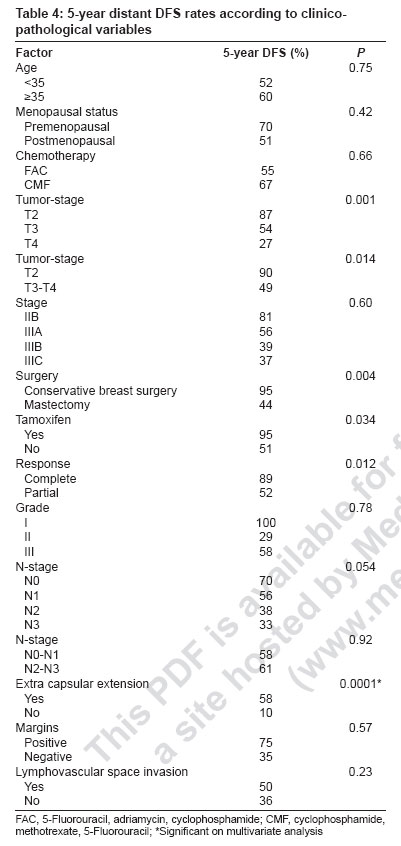
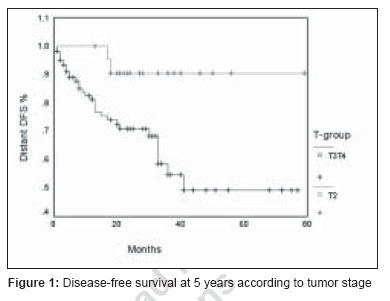
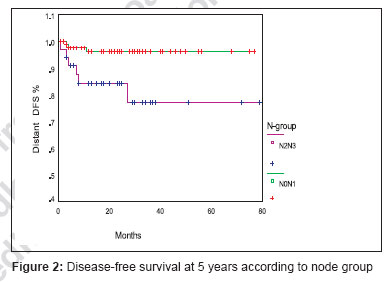
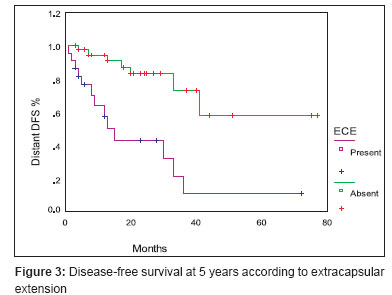
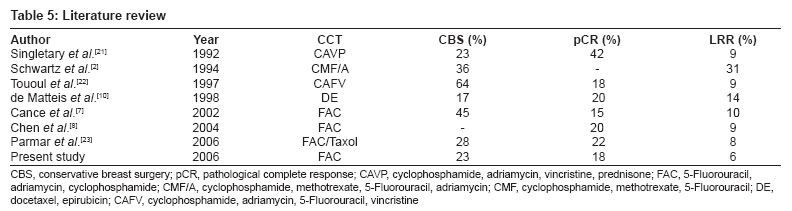
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 75-80 Original Article Patterns of relapse in locally advanced breast cancer treated with neoadjuvant chemotherapy followed by surgery and radiotherapy BS Yadav, SC Sharma, R Singh, G Singh Department of Radiotherapy, Post Graduate Institute of Medical Education and Research, Chandigarh - 160 012 Code Number: cr07020 Abstract Aims : To define the clinical and pathological predictors of locoregional recurrence (LRR) in locally advanced breast cancer (LABC) patients treated with neoadjuvant chemotherapy (NACT).Materials and Methods : We retrospectively reviewed the outcome of 141 patients with stage II to stage III carcinoma breast treated at Department of Radiotherapy, PGIMER, Chandigarh from 1998-2002. Mean age of the patients was 46 years, 49% of patients were premenopausal and 51% were postmenopausal. The tumor stage was T2 in 18%; T3 in 61% and T4 in 26% of the patients. NACT regimen given was FAC (5-fluorouracil, adriamycin and cyclophosphamide) in 85% and CMF (cyclophosphamide, methotrexate and 5-Fu) in 15% patients. Results : After NACT, surgery was possible in 95% patients. Conservative surgery was possible in 23% patients and mastectomy was done in 72% of patients. Pathological complete response (pCR) was seen in 18% patients and pathological partial response (pPR) in 69% of patients. Stable and progressive disease was seen in 6% and 7% of patients respectively. Adjuvant radiation therapy was given to 86% patients. Six percent patients developed progressive disease and 4% of patients did not turn up for radiation. Five year LRR was 6% and relapse free survival (RFS) was 94%. Thirty-two (23%) patients developed distant metastasis resulting in distant metastasis free survival of 77%. The factors that correlated positively with LRR on univariate analysis included tumor stage, stage and pathological nodal stage. However, on multivariate analysis, tumor stage and pathological nodal stage were significant. Factors that correlated for distant relapse were tumor stage, response to chemotherapy, type of surgery, extracapsular extension (ECE) and tamoxifen therapy. On multivariate analysis only ECE was the significant factor that correlated with distant relapse free survival. Conclusion : Thus, tumor stage and pathological nodal stage remains the most important predictor of LRR in LABC. Factors that correlated for distant relapse were tumor stage, response to chemotherapy, type of surgery and ECE and tamoxifen therapy. Keywords: Locally advanced breast cancer, locoregional recurrence, neoadjuvant chemotherapy Introduction Neoadjuvant chemotherapy (NACT) has become standard treatment of locally advanced breast cancer (LABC). NACT is followed by local treatment in the form of surgery and radiotherapy. This modality is presently being used more frequently in patients with operable disease in order to increase the rate of conservative breast surgery (CBS). NACT lead to many advantages. Firstly, objective response of the tumor can be assessed and decision regarding CBS can be made. Secondly, it takes care of distant undetectable microscopic disease. Thirdly, it enables clinician to test the responsiveness of the malignant cells and help to change the chemotherapeutic agents if the tumor appears resistant. [1] The disadvantage of NACT is that it changes the histological extent of disease in 80-90% of cases. Therefore, pathologic indications of radiotherapy may be different than for patients treated with surgery first. [2] Randomized clinical trials have shown NACT and postoperative adjuvant chemotherapy is associated with at least identical recurrence-free and overall survival rates if the same regimen is used in a different sequence. [2],[3],[4] Based on these results, NACT is a reasonable alternative to traditional treatment strategies in patients with LABC. Clinical trial data have documented disease-free and overall survival benefit from NACT in patients who have achieved a pCR. [5] National surgical adjuvant breast and bowel project (NSABP) B-18 trial also suggested improvement in both disease-free and overall survival in patients who have achieved pCR at surgery after NACT. [6] Most common regimen used is FAC [2],[5],[6],[7],[8],[9] but many people are using taxol [10] in combination with anthracyclins. The purpose of this retrospective analysis was to investigate the risk factors for locoregional recurrence (LRR) after NACT for patients with LABC. We also investigated the survival data according to surgical therapy after preoperative chemotherapy. Materials and Methods We retrospectively reviewed the data of 141 patients with LABC (stage II and stage III) treated with NACT followed by surgery and radiotherapy from 1998 to 2002. The patients′ characteristics are reported in [Table - 1]. The mean age at presentation was 46 years (range 25 to 72 years). The pathologic diagnosis was obtained from fine needle aspiration cytology or core biopsy performed before treatment. Eighty four percent of the tumors were infiltrating ductal carcinoma, 6% were lobular carcinoma and 5% were medullary carcinoma. A few patients (13%) with T2 tumor were also included as these had multiple axillary lymph nodes (8%) at presentation a few (5%) with matted ones. Three to four cycles of NACT were administered at three weekly intervals. Two chemotherapy regimes used were, FAC (5-Fu, 600 mg/m 2 , adriamycin, 50 mg/m 2 and cyclophosphamide, 600 mg/m 2 ) in 127 (85%) and CMF (cyclophosphamide, 600 mg/m 2 , methotrexate 40 mg/m 2 and 5-Fu, 600 mg/m 2 ) in 27 (15%) patients. Cost was the limiting factor for choosing CMF. Clinical response to the NACT was assessed by the oncologist and the surgeon according to the WHO criterion. Patients were eligible for breast surgery if the post-chemotherapy tumor was ≤3 cm, but breast volume and expected cosmetic outcome were taken into account. After surgical resection a separate evaluation of pathological responses were classified as follows: pCR-disappearance of tumor and N0 status, pPR-residual tumor. Radiotherapy was administered to all patients with CBS (40Gy/16#/3 weeks). We follow Manchester dose radiotherapy schedule. [11] Patients with positive or close margins were given boost with 192 Ir implant. Dose given was 15Gy. Post mastectomy radiation dose was 35Gy to chest wall and 40Gy/15# to axilla. Axillary node positive patients, perinodal extension and some axillary lymph node negative patients with T3 tumors or when axillary status unknown or when there was incomplete axillary dissection, such patients were also given radiation to axilla and supraclavicular region. Adjuvant chemotherapy was given to all patients. It consisted of three to four cycles of FAC or CMF. A total of six cycles were given. Tamoxifen for five years was given to patients with positive ER/PR status or who were postmenopausal. Locoregional control and survival curves were generated by the Kaplan-Meier method and compared with log Rank test. Locoregional control was defined as any recurrence in the skin or soft tissue over chest wall or a recurrence in the regional lymphatic sites (axilla, internal mammary, infra clavicular and supraclavicular). Multivariate analysis was done using the Cox model for age, histological grade and type, ER status, chemotherapy regime, clinical response, type of surgery, pathological response of a tumor, pathologic lymph node status and perinodal spread. All statistical tests were two-tailed and differences were considered to be statistically significant if P≤0.05. Statistical analysis was performed using SPSS software no. 10 (Statistical Package of Social Science, Chicago, IL). Results Disease characteristics after NACT are listed in [Table - 2]. A complete clinical response was seen in 31 (22%) patients and partial response occurred in 92 (65%) patients. Stable and progressive disease occurred in eight (6%) and nine (6%) patients respectively. After NACT, surgery was possible in 95% of patients. CBS was possible in 26 (23%) patients and mastectomy was done in 84 (72%) patients. In seven patients, the mastectomy was performed during a second operative procedure because the margins of the lumpectomy specimen were involved on pathologic examination. Finally, nine (8%) and four (3.5%) patients treated with CBS had close (< 2 mm) and positive margins, respectively, whereas seven(6.3%) patients in the mastectomy had close margins. Axillary clearance was done in 113 (80%) of patients. Most of the patients (63%) had level-I and level-II axillary dissection. However it was not adequate in most of the patients (71%). Mean number of the nodes dissected were 3(range 1-19). pCR was seen in 26 (18%) patients. On univariate analysis factors that correlated positively with LRR were tumor stage ( P =0.015), stage ( P =0.027) and pathological nodal state ( P =0.008) as shown in [Table - 3]. However, age, premenopausal status, chemotherapy regimen, type of surgery, pCR, histological grade, perinodal spread, margin status or use of tamoxifen was not significant. On multivariate analysis, tumor stage and pathological nodal state remained independent factors associated with LRR. The median follow-up time from the date of registration in outpatient department was 48 months. Eight (6 %) patients developed LRR resulting in five year RFS of 94%. Thirty-seven (26%) patients developed distant metastasis resulting in distant DFS of 77%. Most common site of distant metastasis was lungs (7.7%) followed by bones and liver, 6.3% each and 1.4% to brain. [Table - 4] shows factors that correlate with distant DFS. Distant metastasis occurred in 11% of patients with pCR as compared to 48% in patients with PR. Five year distant DFS for patients with pCR was 89% as compared 52% in patients with PR ( P =0.012). Higher T stage (T4) was associated with higher rate of local as well as distant (51% v 10%) metastasis ( P =0.014). Five year distant DFS in patients with T2 tumors was 90% as compared to 49% in patients with T3 and T4 tumors [Figure - 1]. Higher N-stage was associated with higher rate of LRR. Five-year locoregional RFS was 96% in patients with pathological N0-N1 status as compared to 77% in patients with N2-N3 status ( P =0.008) [Figure - 2]. ECE was also associated with lower distant DFS. Five year distant DFS was 58% in patients who had no ECE as compared to 10% who had ECE ( P =0.0001) [Figure - 3]. Similarly 5 year distant DFS was significantly higher in patients who were given tamoxifen as compared to those who were not on tamoxifen (95% vs. 51%) Discussion The main goal of NACT was to convert inoperable breast tumors to operable tumors. The term inoperable initially included patients with technically unresectable advanced tumors, as well as those with characteristics identified earlier by Haagensen and Stout as indicating an extremely high risk of metastasis and death despite an initial surgical resection (grave signs). [12] The present study demonstrates that NACT can render inoperable disease operable in LABC. This therapy also renders 1/4 th patients to under go CBS. The rates reported in literature ranges from 16% to 80%. Such variation can be due to different study population and different chemotherapeutic regimens used. The observed rates of LRR free and distant metastasis free survival are highly encouraging and compares favorably with those for patients undergoing CBS without NACT. [13],[14],[15] We also noted that T3 or T4 was not associated with increased rates of LRR after CBS and should not be considered a contraindication to CBS as long as appropriate selection criteria are used. CBS rate in the present study is similar to NSABP B-18 for T3 tumor, [6] 23% vs 22%. LRR was 5% in CBS group as compared to 10% in mastectomy group when radiation was given to all patients but it was not statistically significant. This can be because patients who respond well to NACT with CR or good PR were generally considered for BCT. CR to NACT is a good prognostic factor in itself as response to NACT has been found to be associated with better long-term outcome. As these patients belong to good prognosis group they have less local recurrence rate. Mastectomy on the other hand was done on women who had larger tumor sizes and not feasible for BCT or those who do not respond to NACT. This therefore comprises of women who have poor prognostic factors and hence high LRR. A few studies that included patients who were treated with both surgery and radiotherapy have also reported higher local recurrence. A similar study by Parmar et al.[23] from the same country has reported similar results. For example in NSABP B-18 trial, the local recurrence for patients treated with NACT was twice as high for women who were not suited for BCT at diagnosis than those who were candidates for BCT at diagnosis (14.5% vs. 6.9%; P =0.04). [6] Similarly, in the Institut Bergonie series, nine (23%) of 40 patients treated with lumpectomy and radiation experienced LRR. [16] The Institut Curie also reported local recurrence rates of 16% at 5 years and 22% at 10 years for patients who underwent CBS after neoadjuvant chemotherapy. [17] In contrast to these reports, others have found acceptably low rates of LRR. For example, Bonnadonna et al.[18] reported a five year local recurrence rate of 7% after CBS and NACT, which is identical to 6% in the present study. Cance et al.[7] have reported local recurrence rates of 10%. Similarly Chen et al. from MD Anderson Cancer Center [8] analyzed 340 women with breast cancer who were treated with NACT followed by CBS. They observed five-year acturial ipsilateral breast recurrence free rates of 95% and local control of 91% in their study. Patient selection criteria are probably the major factor responsible for the variation in the published rates of LRR. Other factors may be different therapeutic approaches, type of surgery, margins taken and chemotherapeutic drugs used. The limitation of this study is short follow-up and thus LRR reported may have underestimated the lifetime LRR rates. The other limitation is that we were unable to retrospectively determine the percentage of the patients eligible for CBS up front, before receiving NACT. The rates of CBS after NACT in the present study is 23% and is comparable to those reported in the literature (20-25%) for patients with LABC. [9],[19],[20] In the current study, the five-year LRR free survival rates were 95% and 91% for patients treated with CBS and mastectomy respectively. The local recurrence rates reported in the literature vary from 5-16%. In this study, LRR free survival rates were comparable between patients treated with mastectomy and breast conservation. In present study CBS and pCR rates are also comparable to those reported in the literature [Table - 5]. CBS rates are higher in the study reported by Touboul et al.[21] because they have also used preoperative irradiation. Similarly Cance et al.[7] have used dose and time intensified FAC regimen in their patients. Conclusion NACT was the appropriate treatment for patients with locally advanced stage-III and is worthy of consideration in females with stage-IIA or IIB irrespective of tumor size. So NACT should be considered a reasonable alternative treatment for patients with advanced breast cancer. Combined modality therapy based on the NACT represents the standard of care for patients with LABC. NACT contributes to improved operability and enhanced local control and makes breast-conserving surgery possible for many patients without affecting overall survival. The present study also demonstrates that higher tumor stage (T4), higher nodal stage (N2N3) and locally advanced stage are associated with higher rates of locoregional recurrence and distant metastases.References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07020t1.jpg] [cr07020t3.jpg] [cr07020f1.jpg] [cr07020t4.jpg] [cr07020t2.jpg] [cr07020f3.jpg] [cr07020t5.jpg] [cr07020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}