 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
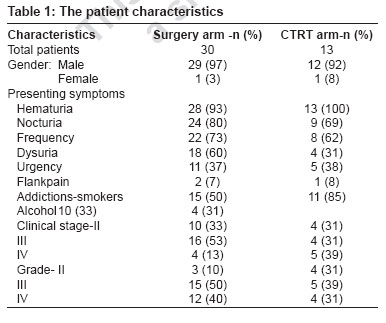
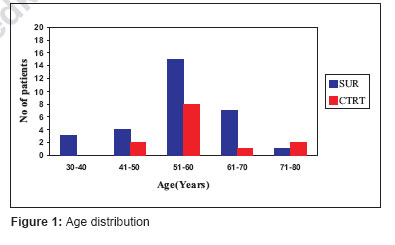
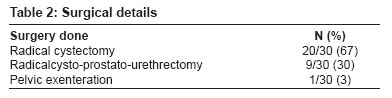
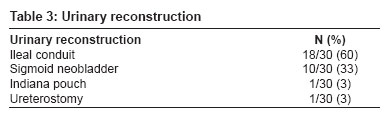
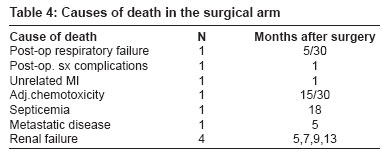
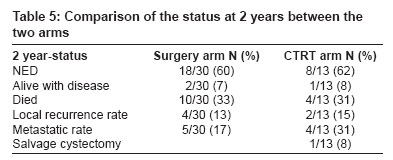
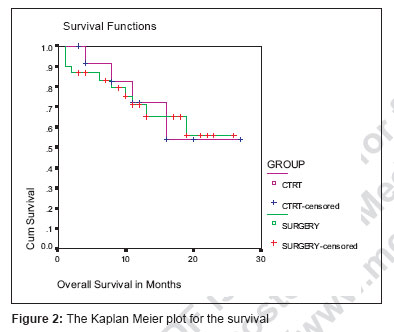
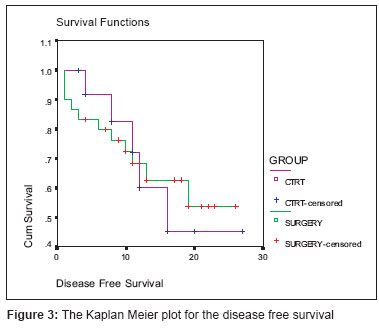
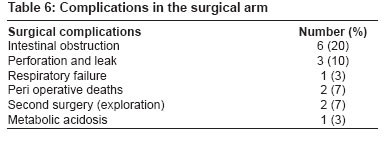
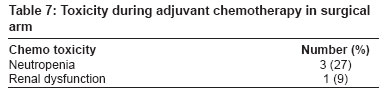
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 81-85 Original Article A prospective study evaluating surgery and chemo radiation in muscle invasive bladder cancer KP Haresh, PK Julka, DN Sharma, GK Rath, R Prabhakar, A Seth Department of Radiotherapy, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi - 110 029 Code Number: cr07021 Abstract Aim : The aim of our study was to compare the two standard treatment approaches in muscle invasive carcinoma of urinary bladder - radical cystectomy and chemo radiation.Materials and Methods : Transitional cell carcinoma (TCC) of bladder of stages, T2 to T4, N0/N1/N2 and MO were included in the study. Patients were allotted to two arms of the study. Arm A consisted of radical cystectomy. Adjuvant CMV chemotherapy was given for T3/T4 or Node positive disease only. Arm B received 2 cycles of neoadjuvant CMV chemo therapy followed by concurrent chemo radiation Results : Forty-four patients were recruited into the study. Thirty patients in the surgical arm and 13 patients in the chemo radiation arm. The actuarial two-year survival rate in surgical arm is 56% while in chemo radiation arm it is 54%. There was no statistically significant difference in disease-free survival also between the two groups. Conclusion : Chemo radiation yielded equivalent survival results with radical cystectomy. So it is worth giving preference to chemo radiation that will give a better quality of life for the patient. Keywords: Chemo radiation, muscle invasive bladder cancer, radical cystectomy Introduction Carcinoma bladder is the second most common urologic malignancy. In the western world, it is the fourth most common cancer in men (after prostate, lung and colorectal) and the eighth most common cancer in women. [1] Presently, radical cystectomy is considered the standard option for muscle invasive cancer of the urinary bladder and achieves excellent local control (90%) with minimal perioperative mortality (< 1%). [2],[3],[4] Surgery alone fails to control that fraction of patients who harbor occult systemic disease at time of diagnosis. Other demerits include loss of sexual function, altered body image, potential for progressive upper urinary tract deterioration and the long-term social and psychological problems inherent with the diversion techniques. Multimodality bladder preserving approach combining transurethral resection (TUR) with chemo radiation with prompt cystectomy in patients with poorly responding tumors offers a valid alternative option with long term survival rates approaching those for radical cystectomy. [5],[6],[7] Nevertheless, a well functioning bladder can be achieved in 60-83% of survivors. [5],[6],[7],[8],[9] However the complexity, cost and morbidity of bladder sparing approaches must be weighed against the improved quality of life when the native bladder is retained. Aims and objectives Materials and Methods Patients included in this study comprise TCC of urinary bladder Stages, T2 to T4, N0/N1/N2, MO. These patients were allotted to either arm A or B. The patient′s preference was given priority while allotting the patients to the two arms of the study. Arm A - Radical cystectomy. Adjuvant CMV chemotherapy was given for T3/T4 or node positive disease only. For T2 and N0 disease no adjuvant treatment was given. In those who received chemotherapy four cycles were given three weekly starting two weeks after surgery. Dose schedule - Inj. Cisplatin - 75 mg/m² D1 IV infusion, Inj. Methotrexate-40 mg/m² D1 IV, Inj. Vinblastine - 6 mg/m² D1, IV, every three weekly. Arm B - Chemo-radiotherapy arm. Patients received two cycles of neoadjuvant CMV chemo therapy three weekly (doses same as in group A) followed by concurrent chemo radiation. Radiotherapy started after two to three weeks depending on the blood count. External beam radiotherapy was delivered to a dose 60 Gy/ 30 fractions / 6 weeks with concurrent inj cisplatin 40 mg/m 2 weekly IV. The initial 40Gy/20 # was delivered by four field box technique to the whole pelvis, while the rest 20Gy/10# was delivered by 3DCRT to the tumor volume (bladder) without any gap between the treatments. Patients were treated on linac/telecobalt machine. Toxicity was recorded using CTC Version 2. Two weeks after the completion of RT, patients underwent cystoscopy, biopsy of any residual lesion and urine cytology. If residual lesions were superficial, they were treated cystoscopically. If large they underwent salvage cystectomy. The projected two-year survival rate was assessed by the Kaplan and Meier method. The actuarial survival was inferred by log-rank test. Levels of significances by P value. Results From January 2002 to December 2004, a total of 44 patients were recruited into the study of which 43 patients are evaluable. 30 patients were recruited in the surgical arm and 13 patients were recruited in the chemo radiation arm. The patient characteristics are shown in the [Table - 1]. Age distribution is shown in [Figure - 1]. The surgical details are given in the [Table - 2], [Table - 3]. The most important thing in this group is that 90% of the sigmoid neo bladder patients had very good function. Survival data at two years The actuarial two-year survival rate in surgical arm is 56% while in chemo radiation arm it is 54%. The log rank test performed showed a significance value of 0.9262, which showed that there is no statistically significant difference in the two-year actuarial survival between the two arms. The Kaplan Meier plot for the survival is shown in [Figure - 2]. Regarding the disease-free survival also there was no statistically significant difference between the two groups. The Kaplan Meier plot is shown in [Figure - 3]. Complications The toxicity pattern of adjuvant chemotherapy in surgical arm in this group is shown in [Table - 7]. Four patients (36%) had significant chemotherapy toxicity. Three of them had grade 3/4 neutropenia, managed conservatively and one of them died. One patient had deranged renal functions after two cycles of chemotherapy. In the chemo radiation arm all patients tolerated neoadjuvant chemotherapy well without any significant CTC Grade III/IV side effects. During concurrent chemo radiation, only two patients developed grade 1 neutropenia after fourth cycle of chemotherapy and in both patients, the sixth cycle was withheld without stopping radiotherapy. No significant bladder or bowel CTC Grade III or IV toxicity was encountered in any patient. Discussion While radical cystectomy cures many cases of bladder cancer, almost 50% develop metastatic disease. Adjuvant chemotherapy has been suggested in these patients in order to reduce the probability of relapse and to improve survival. Dimopoulous et al. [10] reviewed the role of adjuvant chemotherapy. They observed that adjuvant chemotherapy improved disease-free survival, event free survival and overall survival. Unlike organ-confined disease, there is some evidence that those patients with extravesical disease or node positive disease may benefit from adjuvant chemotherapy. Thus in our study we had given adjuvant CMV chemo to patients with T3 and node positive ones. A systematic review and meta-analysis of updated individual patient data of adjuvant chemotherapy by ABC Meta-analysis Collaboration in 2006 [11] showed an overall hazard ratio for survival of 0.75 (95%CI 0.60-0.96, P =0.019) which suggests a 25% relative reduction in the risk of death for chemotherapy compared to that on control. The role of neoadjuvant chemotherapy in bladder cancer is of doubtful value. Five randomized trials have not shown any survival benefit-these include the RTOG89-03, EORTC, CUETO, ABCSG and RMH studies. [10],[12],[13],[14],[15] However the Nordiac Co-operative Bladder cancer study-1 reported a survival benefit of 12% at five years in a subset of patients with stages T3 and T4a. An update of a systematic review and meta-analysis of individual patient data by the ABC meta-analysis collaboration in 2005 [22] found a significant survival benefit associated with platinum-based combination chemotherapy (HR = 0.86, 95% CI 0.77-0.95, P = 0.003), equivalent to a 5% absolute improvement in survival at five years. There was also a significant disease-free survival benefit associated with platinum-based combination chemotherapy (HR = 0.78 95% CI 0.71-0.86, P < 0.0001), equivalent to a 9% absolute improvement at five years. In our study we had opted to give two cycles of neoadjuvant chemo to all patients before chemo radiation with an idea to down stage the tumor and to give a benefit by killing the possible microscopic metastatic disease before venturing for local control. Today there is little scarcity for the literature on radical cystectomy. Different studies have shown a five-year local control rate of 90% with radical cystectomy. The five-year distant metastatic rate ranges from 30 to 50%. [2],[3],[4],[16],[17] The recent chemo radiation series have shown an initial complete response ranging from 60 to 80% and five-year distant metastasis, 34 to 40%. [5],[6],[7],[8],[9],[18],[19],[20],[21] As the follow-up period in this study is short, it is unwise to compare our results with the five-year figures quoted in the literature. One has to really wait for the data to become mature before comparing them directly. If we analyze the survival curves for the two groups, we can see that the curves are neck to neck with no significant difference between the two groups. The survival figures shown in this study were identical with the survival figures in the already published studies. Conclusions The standard treatment option in muscle invasive cancer of urinary bladder is radical cystectomy. The current focus in oncology is shifting from disease control to the quality of life issues and organ preservation. Chemo radiation is an emerging alternative to surgery in the treatment of muscle invasive bladder cancer. However, proper randomized trials are needed to evaluate the superiority of one over the other.References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07021t7.jpg] [cr07021t2.jpg] [cr07021t4.jpg] [cr07021f3.jpg] [cr07021t3.jpg] [cr07021f1.jpg] [cr07021t5.jpg] [cr07021f2.jpg] [cr07021t6.jpg] [cr07021t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}