 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
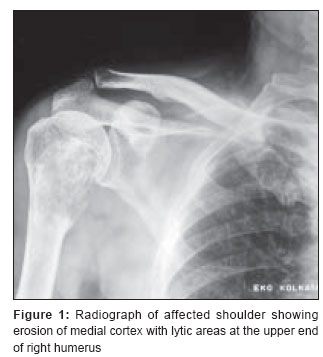
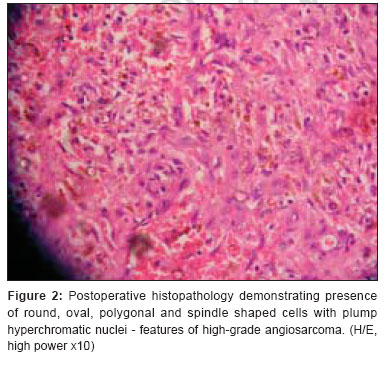
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 96-99 Case Report Post-irradiation angiosarcoma of bone Srabani Mittal, Chanchal Goswami, Nandini Kanoria, Aniruddha Bhattacharya Department of Medical Oncology, B P Poddar Hospital and Medical Research Ltd., Kolkata Code Number: cr07024 Abstract Radiation therapy is extensively used for treatment of malignancies, but angiosarcomas occurring in an irradiated area are uncommon. We report a rare case of high-grade epithelioid angiosarcoma of upper end of right humerus in a 67-year-old male occurring ten years following irradiation for giant cell tumor of the same anatomical site. The patient presented with progressive painful swelling over right shoulder and his X-ray showed erosion of medial cortex with lytic areas at upper end of humerus. He underwent excision of affected part of humerus followed by cemented hemiarthroplasty and bone grafting. After initial histopathological diagnostic dilemma the final report was given as post-radiation angiosarcoma. Disease recurred at the end of one-year follow-up period where upon he underwent wide resection with prosthesis replacement. He received four cycles of combination chemotherapy with doxorubicin and ifosfamide and currently is free of recurrence after six months follow -up.Keywords: Diagnostic challenge, osseous angiosarcoma, post-radiation malignant transformation Introduction Although radiation therapy is extensively used for treatment of malignant conditions, angiosarcomas occurring in an irradiated area are rather uncommon. These aggressive malignant neoplasms of vascular origin account for only 2% of all soft tissue sarcoma. [1] Literature suggests that there is a definite cause-and-effect relationship between irradiation and angiosarcoma. Apart from the direct carcinogenic effect of irradiation, prolonged stimulation for tissue repair resulting from tissue damage secondary to irradiation-induced vascular changes also play an etiologic role in the development of angiosarcomas. [2] Radiation-induced angiosarcomas are generally reported to occur following therapeutic irradiation for carcinoma of breast, cervix, ovary and endometrium. Few rare presentations of the disease include angiosarcoma of larynx, spleen and terminal ileum. However, osseous angiosarcoma secondary to therapeutic irradiation has been described infrequently. Case Report We report a rare case of high-grade epithelioid angiosarcoma of bone in a 67-year-old male, following irradiation for giant cell tumor of upper end of right humerus. In 1994 he received external radiation therapy (46 Gy in 23 fractions) to right shoulder. Axilla was not included in the radiation portal. There was no lymphedema at any time following radiotherapy. Ten years post radiation, the patient presented with painful swelling over right shoulder in April 2004. Radiograph of the affected shoulder showed erosion of medial cortex with lytic areas at the upper end of humerus [Figure - 1]. Fine needle aspiration (FNA) from the lytic areas did not report any malignant cells initially. But with the persistence of pain and progression of swelling over the right shoulder, the FNA slides were further reviewed by three pathological laboratories. Considering the history of radiotherapy for treatment of giant cell tumor, possibility of post-treatment malignant transformation was contemplated and the review diagnosis was given as malignant mesenchymal tumor. The exact size of the bony lesion at the time of diagnosis was not available. The magnetic resonance imaging (MRI) scan revealed a heterogenous exophytic mass involving the upper third of shaft and head of humerus. The deltoid, sub-scapularis and rotator cuff muscles were not infiltrated by the mass. The neurovascular bundle was normal. There was no associated dermal component. Following diagnosis, he underwent excision of the affected head and neck of humerus, with thorough debridement and curettage, followed by cemented hemiarthroplasty and bone grafting. Postoperative histopathology confirmed malignant mesenchymal tumor. With the given background of diagnostic dilemma, the slide was again reviewed by several pathology centers and finally was reported as post-radiation angiosarcoma of right humerus in November 2004 [Figure - 2]. The patient was on routine follow-up till December 2005, when he again noticed a painful swelling over his right shoulder. He was re-explored and per operatively there was a large exophytic growth with hemorrhagic tissue and loosening of the medial graft placed previously. Minimal surgical intervention involving debridement and chemical cauterization was done. Postoperative histopathology showed necrotic and hemorrhagic tissue infiltrated by inflammatory cells and tumor composed of round, oval, polygonal and spindle shaped cells with plump hyperchromatic nuclei. Tumor giant cells with bizarre hyperchromatic nuclei were also present. The diagnosis was reported as recurrence of angiosarcoma. Considering his localized disease status, he underwent wide resection with custom-made titanium prosthesis replacement of proximal right humerus in February 2006. The postoperative biopsy showed presence of malignant epithelioid cells arranged in sheet like pattern with large vesicular nuclei and prominent nucleoli. Immunohistochemistry stained positive for Vimentin and CD 31 with focally positive Von Willibrand factor. The histological and immunohistochemical profile was consistent with diagnosis of high-grade epithelioid angiosarcoma. Following post-operative recovery, the patient was treated with four cycles of combination chemotherapy with Doxorubicin and Ifosfamide. Discussion Radiation-associated angiosarcoma is an infrequent diagnosis. Risk estimates of post-irradiation sarcomas of any histologic subtype range from 0.03 to 0.8%. [3],[4] Studies generally agree that the largest proportion of radiation-associated sarcomas comprises of malignant fibrous histiocytomas and osteosarcomas, with angiosarcoma diagnosed less frequently. Osseous angiosarcomas occur third in frequency after osteosarcoma and fibrosracoma. Two case-series from Memorial Sloan Kettering Cancer Center reported the prevalence of angiosarcoma / lymphangiosarcoma among radiation-associated sarcomas of soft tissue and/or bone to be 15% only. [5],[6] The most frequent primary disease for which radiation is given as therapy appears to be breast cancer, followed by gynecologic cancer. In an extensive review of literature between 1970 and 1996, only 66 cases of angiosarcomas were reported and out of these, 44% occurred after radiation for breast cancer and 21% in irradiated gynecological cancers. 85% of radiation-associated angiosarcoma developed in the cutaneous area. The median age at diagnosis was 65 years and the median latency period from irradiation to diagnosis was 96 months. [7] Radiation associated angiosarcoma developing in unusual sites such as spleen, small bowel, urinary bladder and prostate have also been identified. In a study of 53 cases of post-radiation soft tissue sarcomas at the Armed Forces Institute of Pathology, Laskin and colleagues found only one case of angiosarcoma arising in the chest wall seven years following radiation therapy for mediastinal Hodgkin′s disease. [8] The most widely applied diagnostic criteria for radiation-associated sarcomas are adapted from Cahan′s report of a sarcoma arising in irradiated bone. [9] These criteria are summarized as a histologically proven neoplasm arising in the field of radiation with a latency period ranging from at least 3-5 years following radiation treatment. Our case fulfills these criteria, namely histologically proven angiosarcoma arising in osseous tissue of humerus ten years after external beam irradiation for giant cell tumor. Though presence of chronic lymphedema after radiation therapy is considered as an early warning sign for later development of angiosarcomas, our patient did not have any post-radiation lymphedema. The diagnosis of osseous angiosarcoma by conventional radiographic assessment is not very precise, but it plays an essential role in characterizing lesions and confirming their multiplicity. Similar to the X-ray findings of our case, solitary lesion usually presents as a destructive lytic mass or a mixed lytic-sclerotic pattern and high-grade lesions exhibit features of complete cortical destruction and extension into soft tissue. In addition to plain radiography, CT scan is helpful in confirming the permeative and invasive character of the lesions and allows detection of discrete intra-tumoral mineralization better than other imaging modalities. MRI is considered useful in the characterization of soft tissue extension and involvement of neurovascular structures and joints and is the best method for preoperative staging and for selecting the correct site for biopsy. Whole body bone scan may or may not help in diagnosis and it can be often negative in aggressive destructive lesions. Angiosarcomas are a diagnostic challenge to pathologists. Histologically, these tumors are described as malignant endothelial neoplasms with vasoformative architecture and are characterized by atypical, multilayered or solid endothelial proliferation. [10] Marker studies are helpful in diagnosis of this vascular neoplasm. Angiosarcomas stain positively for factor VIII that helps in differentiating it from Ewing′s sarcoma and anti-CD 31 antibodies are the most specific immunohistochemical marker. We refer to the clinical and histopathological diagnostic predicament in our case in correct identification of the disease. Given the rarity of condition it was unlikely that the diagnosis would be thought of at initial presentation but with the history of irradiation and subsequent development of an enlarging mass in the irradiated field ten years later, post-radiation malignant transformation needed to be considered. The initial diagnostic delay is often known to affect the prognosis. Though the role of chemotherapy remains undefined in treatment of angiosarcoma, our patient is currently free of disease recurrence after six months of completion of combination chemotherapy. Several controversies exist regarding optimal management of the disease and one of them is the use of Interleukins. Intratumoral injection of recombinant interleukin-2 has been shown to be effective for angiosarcoma of the skin. Sasaki et al reported that high-dose rIL-2 treatment suppressed the development of distant metastasis and prolonged survival in a study of 18 patients with angiosarcoma who did not have metastasis before the treatment. [11] Recently, there has been evidence that most post radiation sarcomas show an extensive expression of the KIT protein. Unfortunately we do not have any information pertaining to KIT expression in our case. In a study involving clinical, immunohistochemical and genetic assessment of post-radiation sarcomas, two of 3 angiosarcomas revealed> 80% positive tumor cells, whereas the third had few solitary positive tumor cells. KIT expression was considerably more pronounced in post-radiation sarcomas compared with a group of nonpostradiation, non-GIST sarcomas. [12] Treatment with the KIT inhibitor Imatinib may be considered in cases where radical surgery is not possible, but whether post-radiation sarcomas will respond to KIT inhibition remains to be established. Angiosarcomas are suggested to have the poorest prognosis among soft tissue sarcomas. High-grade angiosarcomas exhibit extremely aggressive behavior with rapid local growth and early disseminated metastasis. Multicentricity does not affect prognosis but metastatic disease at presentation is a consistent factor associated with worsened survival. [13] The distal location of post-radiation sarcoma is a favorable prognostic factor, as it increases the possibility for radical surgery. [14] Furthermore, the inability to achieve microscopically negative margins for patients with angiosarcomas undergoing surgical resection is associated with an unfavorable survival outcome. [15] Radical resection results in a relatively favorable outcome with up to 39% 5-year survival, but may not be feasible. [16] We recommend more attention on proper diagnostic approach and histopathological interpretation as it contributes to early identification and appropriate management of the disease. References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07024f1.jpg] [cr07024f2.jpg] |
| |||||||||

{kind=link}
{kind=link}