 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
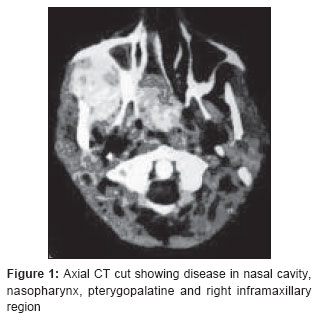
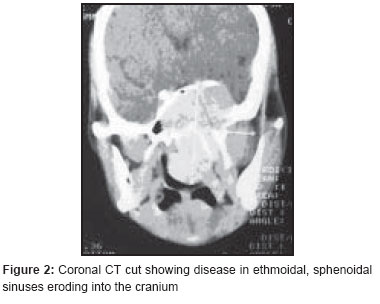
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 100-101 Case Report Nasopharyngeal angiofibroma treated with radiotherapy MG Janaki, S Nirmala, AG Rajeev Department of Radiotherapy, MS Ramaiah Teaching Hospital, Gokul, Bangalore Code Number: cr07025 Abstract Nasopharyngeal angiofibroma is a rare, highly vascular, benign, locally aggressive tumor, affecting boys of adolescent age. The aggressiveness and high vascularity makes surgery and even a biopsy difficult in majority of cases. Although surgery is the treatment of choice in early cases, considerable debate exists regarding the treatment of advanced disease with intracranial extension. Radiotherapy provides a good response and also avoids surgery-associated morbidity. We are herewith reporting a case of nasopharyngeal angiofibroma who showed complete hemostasis and improvement in vision to radiotherapyKeywords: Angiofibroma, nasopharyngeal, radiotherapy Introduction Nasopharyngeal angiofibroma is a rare, benign tumor seen predominantly in adolescent males. It is a typical example of locally aggressive tumor and due to this aggressiveness; it poses a challenge to the treating physician. It is difficult to do a biopsy in majority of the cases due to its high vascular nature. Various treatment modalities like surgery, radiotherapy, embolization, chemotherapy and hormonal therapy are used and each has its own limitations. Radiotherapy is the treatment of choice for patients with intracranial extension. This case is reported due to its rarity and the patient showed a good response in terms of hemostasis and improvement in vision to radiotherapy.Case Report A 15-year young boy presented in August 2004 with history of right sided facial swelling of 18 months duration associated with right sided nasal block, progressive loss of vision in the right eye of three months duration and bleeding and pus discharge from right nostril of 15 days duration. Examination findings included right sided malar fullness, loss of right nasolabial groove, proptosis of the right eye with widened palpebral fissure, a three cm sub mucosal swelling from upper part of right buccal mucosa and a large fleshy red mass covered with mucous discharge from right nostril. Patient also showed right-sided partial optic atrophy on ophthalmoscopy. A computerized tomography (CT) scan with contrast done showed a moderately well delineated brightly enhancing soft tissue mass arising from the soft palate, right nasal cavity, nasopharynx with extension onto the right infratemporal, pterygopalatine and right inframaxillary region. The same mass was extending to the ethmoidal, sphenoidal sinuses eroding into the cranium. A biopsy from the mass in the nasal cavity showed features of an angiofibroma covered with nasopharyngeal epithelium, which was variably lined by stratified squamous epithelium or ciliated columnar cells. The final diagnosis was stage IV nasopharyngeal angiofibroma due to intracranial extension [Figure - 1],[Figure - 2]. In view of the intracranial extension, the patient was not considered for surgical resection and hence radiotherapy was started. External beam radiotherapy was delivered through a wedge pair of anterior and oblique co-planar cobalt beams to a dose of 4600 cGy/ 23 Fr /5Fr/wk/ 31 days after doing a CT simulation. After sixth fraction, the patient developed severe nasal bleed, which lasted for a day and was treated with nasal pack and Foley′s bulb inflation in the nasopharynx. Rest of the therapy schedule was uneventful. Patient was reviewed one month later and he showed a good regression of mass and a gradual improvement of vision in the right eye. Patient is doing well at 22 months and a follow up CT scan is not yet done as the patient is from a distant place. We will do a review CT scan at 24 months. Discussion Nasopharyngeal angiofibroma is a classical example of a slow growing, locally aggressive, histologically benign vascular tumor affecting the adolescent boys. This exclusive occurrence among boys is probably linked to the androgen. The site of origin is thought to be either from the superior aspect of the sphenopalatine foramen or from the pterygo-palatine fossa, in the recess behind the sphenopalatine ganglion at the exit of the pterygoid canal. [1] A clinical triad of unilateral nasal obstruction, recurrent spontaneous epistaxis and nasal drainage is diagnostic of nasopharyngeal angiofibroma. Most often biopsy is not done as it is highly vascular but a biopsy done as in our case confirms the diagnosis. Three classification systems, used to stage nasopharyngeal angiofibroma are Fisch′s, Chandler′s and Radowski′s adaptation of Sessions′ classification are essentially based on the extent of the disease. [2] Various treatment modalities like cryotherapy, sclerosing therapy, hormonal treatment, radiotherapy, [3] chemotherapy, embolization and surgery [4],[5] are used to treat nasopharyngeal angiofibroma. Since it is rarely seen, there are no standard guidelines available in the literature especially for advanced cases. Essentially treatment depends on the physician preference, available expertise and patient preference. Surgery is used to treat nearly two thirds of the patients. Endoscopic removal is also considered for selected cases with preoperative embolization to control bleeding at the time of removal. [6],[7] Radiotherapy offers a very good local control rate, as high as 80-85% with the tumors regressing very slowly over two to three years. [5] In fact, McAfee et al . have reported 91% control with a dose of 30-36 Gy and have not seen any complications of Radiotherapy in a follow up of two to five years. [8] Nasopharyngeal angiofibroma regresses over a long period of two to three years and any lesion that is persisting after 24 months is likely to be a recurrence. [2],[9] A dose of 36-46 Gy is recommended over a period of 4-5 weeks. Endocrine hypo function, cataract formation and second malignancies, the possible side effects of radiation have to be kept in mind [8] and hence radiotherapy needs to be used only when surgery is not possible or in residual and recurrent lesions. State of art radiotherapy in the form of 3DCRT, IMRT and proton therapy may help to reduce the late radiation toxicities. References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07025f2.jpg] [cr07025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}