 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
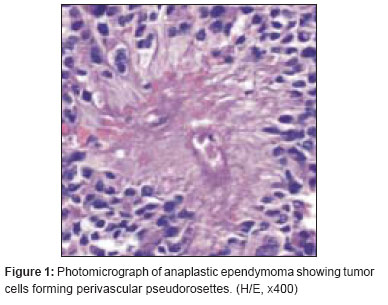
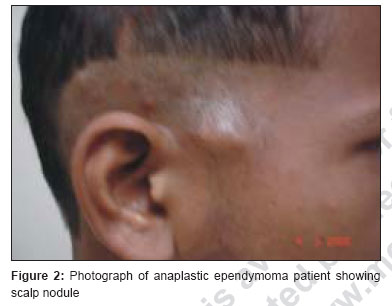
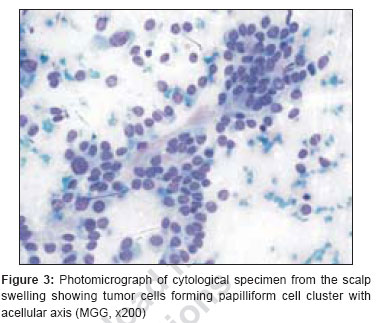
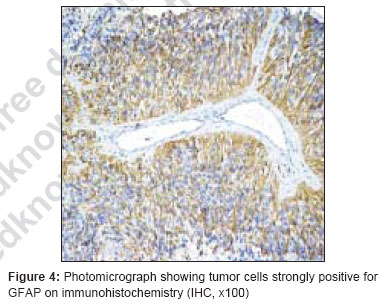
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 102-104 Case Report Extraneural metastases in anaplastic ependymoma Pavan Kumar, Neeraj Rastogi, Manoj Jain, Poonam Chhabra Department of Radiotherapy, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow - 226 014 Code Number: cr07026 Abstract Ependymoma are rare glial neoplasm, it rarely metastasize outside the central nervous system. We present a case of anaplastic ependymoma with extraneural metastases with review of literature. A ten-year-old male child presented with anaplastic ependymoma of choroid plexus and treated with craniospinal radiotherapy in 1998. He had intracranial recurrence in 2004, confirmed by biopsy. He was given adjuvant chemotherapy in form of PCV. At 10 months after completion of chemotherapy, he developed extracranial scalp metastasis and so was treated with palliative local radiation therapy to the scalp metastasis and systemic chemotherapy with oral Etoposide. Scalp metastasis completely disappeared and ataxia improved. After five cycles of chemotherapy, the patient had progression of disease in form of scalp and cervical lymph node metastasis confirmed by fine needle aspiration cytology, biopsy and immunohistochemistry. He was given salvage chemotherapy (carboplatin + ifosfamide + etoposide) at 3-weekly. He had partial response and was still on chemotherapy till May 2007. Keywords: Chemotherapy, ependymoma, radiotherapy Introduction Ependymomas are rare glial neoplasm. They comprise of 5% of all intracranial tumors in adults and 10% in children. [1] Ependymoma usually arise intracranial within infratentorial location or supratentorial brain and less commonly from spinal cord. They mainly relapse at primary and spinal cord, but rarely metastasize outside the central nervous system. Extra neural metastasis occurs mainly in the lung/ pleura, liver and lymph nodes. [2],[3],[4],[5] Here we report a case of anaplastic ependymoma metastasizing to cervical lymph node and scalp.Case Report A ten-year-old male child presented with complaints of progressive loss of vision, headache and vomiting since March 1997. Contrast-enhanced computed tomography (CECT) of brain showed mass in the choroid plexus of the right occipital horn of the lateral ventricle, so he underwent subtotal resection in April 1997. Total surgical excision was abandoned due to intraoperative bleeding. Histopathological examination of the resected tissue showed a tumor with morphology consistent with anaplastic ependymoma. The patient was advised post operative radiotherapy but did not report for radiotherapy. In July 1998, he again complained of headache and vomiting, a repeat CECT of head showed a large calcified residual mass surrounded by cystic area in right occipital horn of lateral ventricle. He was re-explored with right parieto-occipital craniotomy and total excision of choroid plexus mass was done. Histopathological examination revealed the diagnosis of anaplastic clear cell ependymoma. Postoperatively he had no neurological deficit. Patient was treated with craniospinal irradiation with dose of 36Gy in 18 fractions to whole brain followed by a boost of 18 Gy in 12 fractions to a total of 54 Gy in 30 fractions to primary tumour along with 30Gy in 20 fractions to whole of the spinal cord. Radiation was completed in September 1998 and the next five year period was uneventful. He again complained of weakness in right upper and lower limb in February 2004. CECT scan showed a recurrent mass in right parieto-occipital area. Sub total excision of mass was done and histopathology revealed anaplastic ependymoma without clear cell areas [Figure - 1]. On immuno-histochemistry the tumor showed diffuse strong positive immunostaining for glial fibrillary acidic protein (GFAP). After surgery power in right upper and lower limb improved. Adjuvant PCV chemotherapy was planned (Procarbazine 60 mg/m 2 D8-21, Lomustine 100 mg/m 2 D1, Vincristine 1.4 mg/m 2 D1 and D29) at six weekly interval. Patient received seven cycles of chemotherapy up to May 2005 and left further treatment. Patient reported after 10 months in March 2006 with nodular swelling in the pre-auricular area of the right side of scalp [Figure - 2]. The fine needle aspiration cytology from scalp swelling was positive for malignant cells with cytological features consistent with metastatic ependymoma [Figure - 3]. CECT head showed a small enhanced mass lesion in right parieto-occipital area with perifocal edema suggestive of local recurrence Patient was given palliative radiotherapy of 8 Gy in one fractions to the scalp swelling with single agent chemotherapy (oral Etoposide 50 mg/m 2 day 1-21) at 4 weekly. The scalp nodule completely disappeared with improvement in ataxia and gait. After five cycles of chemotherapy, the patient had disease progression in August 2006 with multiple nodules on right side of the scalp, largest measuring 1.2 x 1.2 cm 2 , hard fixed. It was treated again by 8 Gy single fraction. He subsequently developed right upper deep cervical lymphadenopathy and underwent excision biopsy. Histopathological examination confirmed the diagnosis of anaplastic ependymoma metastatic to cervical lymph node. On immunohistochemistry the tumor was positive for EMA, Vimentin and GFAP [Figure - 4]. In view of progression of disease during chemotherapy, palliative chemotheray using ifosfamide (1.8 gm/m 2 d1-5) plus etoposide (100 mg/m 2 d1-5) alternating with carboplatin (AUC 5) plus vincristine (1.4 mg/m 2 ) at three weekly interval was started and patient has partial response without any new lesion for last nine months till May 2007.Discussion Ependymoma mainly relapses at primary site and some times at spinal cord within the central nervous system. It rarely metastasizes outside the central nervous system as extraneural metastasis. Newton et al. [5] reviewed 81 ependymomas at Memorial Sloan-Kettering Cancer Center between 1956 -1989. Only five (6.2%) had extra neural metastasis and the time from diagnosis to development of extra neural metastasis was 0-288 months. In 4/5 cases primary tumor progression was present at the time of metastasis. The sites of metastasis were lung and thoracic lymph node - 2, pleura and peritoneum -2 and liver -1. Dunst et al. , [2] reported a case of ependymoma of left occipital area in which metastasis in cervical lymph nodes appeared along with recurrence at primary and multiple metastases to the spinal canal at four and a half years after surgical resection and craniospinal radiotherapy. Graff et al. , [4] reported a case of spinal ependymoma with extra neural metastasis to pleura, liver, nodes in abdomen and thorax. Rousseau et al. , [6] reported 80 children of ependymoma with five years actuarial survival and event- free survival of 56% and 38%, respectively. There were 34 relapses at 3-72 months after diagnosis. Twenty patients had local failure at the primary site while, 14 had leptomeningeal dissemination without any extraneural metastasis. McLaughlin et al. , [7] reported 41 patients, who received post operative craniospinal radiotherapy between 1966 to 1989. Local recurrence was noticed in 51% at six years while10 year overall and relapse free survival was 51% and 46% respectively. There was no metastasis outside the central nervous system. The tumor site was the only factor that influenced the survival ( P =0.0004).Timmerman et al. , [8] reported that primary tumor site is the predominant sites of failure with one case of extracranial metastasis to the spinal cord without any extraneural metastasis, so it was suggested to intensify the local treatment. The metastasis to and from the central nervous system is low due to unique property of brain and tumour interaction with blood-brain barrier, microglia, matrix protein, cytokines and growth factors. [9] Because of rarity of extraneural metastasis to scalp and cervical lymph node from intracranial ependymoma and lack of any consensus of treatment strategy, the patient was treated by local radiation and salvage chemotherapy to stabilize the disease with possibility to improve the survival. References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07026f4.jpg] [cr07026f3.jpg] [cr07026f2.jpg] [cr07026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}