 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
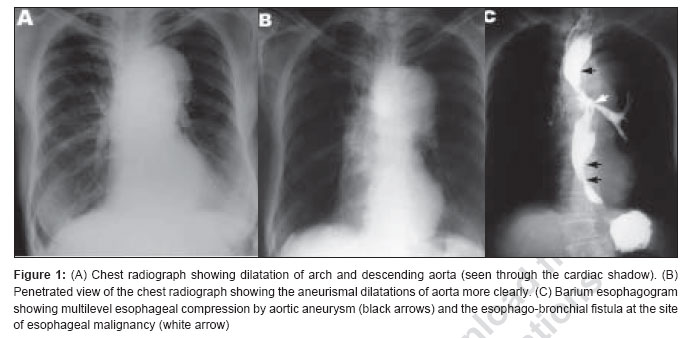
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 108-110 Case Report Multifactorial dyspahgia complicated by esophago-bronchial fistula Julie Sebastian, VS Kirankumar, Joseph M Pappachan, Sue Ann Zachariah, TR Radha, P Sujathan Department of Medicine, Kottayam Medical College, Kerala Code Number: cr07028 Abstract Dysphagia in an elderly patient necessitates urgent clinical evaluation to exclude the possibility of an underlying esophageal malignancy. Atherosclerotic aortic aneurysms are common in old age, but dysphagia aortica resulting from compression of the esophagus by an aortic aneurysm is a rare cause for dysphagia. Development of a malignant esophago-airway fistula can occur from a variety of tumors, the most common of which is esophageal cancer. A case of longstanding dysphagia resulting from dysphagia aortica later developing an esophageal malignancy complicated by esophago-bronchial fistula is outlined in this unique case report.Keywords: Dysphagia aortica, esophago-airway fistulae, esophago-bronchial fistula and esophageal cancer Introduction Dysphagia is an alarming symptom in the elderly, necessitating urgent clinical evaluation. Dysphagia aortica, which results from compression of the esophagus by an aortic aneurysm, is an unusual cause for dysphagia. [1] Malignancy of the esophagus should be ruled out in all elderly individuals presenting with dysphagia. Fistulation into the tracheobronchial tree in adults result mostly from malignancy and esophageal cancer is the commonest tumor encountered in such patients. [2] This report outlines a case of dysphagia aortica that later presented with esophageal cancer complicated by an esophago-bronchial fistula.Case Report A 66-year-old woman was admitted for evaluation of progressive dysphagia and loss of weight over the past four months and bouts of cough on intake of food and breathlessness for the past two weeks. She had mild dysphagia for solid food in the previous four years that had been diagnosed elsewhere (by endoscopy, barium study CT-thorax and esophageal manometry) to be dysphagia aortica resulting from an aortic aneurysm, for which no active treatment had been recommended. At that time, she had been advised soft semisolid and liquid diet, regular follow-up and repeated esophagoscopy after one year, but had not done so because her symptoms had been static in the previous years. She had 30-pack years history of smoking but had stopped that habit four years earlier, when the aneurysm had been diagnosed. Her high blood pressure, detected at the time of diagnosis of the aneurysm, had been well-controlled with lisinopril 10 mg daily. She was emaciated and asthenic. Blood pressure was 160/100 mm of Hg and pulse rate was 94 beats/minute. She was afebrile. Prominent aortic pulsations were noticed in the epigastrium. Examination of the respiratory system revealed crackles in the infrascapular and axillary areas of the chest on the left side. Her hematological and biochemical investigations were unremarkable. Chest radiograph revealed dilatation of the arch and the descending aorta [Figure - 1]A and B and left lower lobe pneumonitis. Electrocardiography showed evidence of left ventricular hypertrophy and the echocardiography confirmed concentric hypertrophy of the left ventricle and dilatation of aortic arch. Initially the patient did not consent for an esophagoscopy and hence a barium esophagogram was performed. It showed irregular narrowing of the mid-portion of esophagus, an esophago-bronchial fistula and compression of the esophagus by the aortic aneurysm in the upper and lower portions [Figure - 1]C. CT scan of the thorax revealed a growth in the mid esophagus, a left-sided esophago-bronchial fistula and aneurysms of the arch and descending thoracic aorta with multiple areas of calcification consistent with diffuse atherosclerosis. An esophagoscopy showed an ulceroproliferative growth in the mid esophagus nearly obstructing the lumen and a fistulous opening into the left main bronchus. Biopsy from the growth confirmed the presence of well-differentiated squamous cell carcinoma. The patient was managed by feeding through a nasogastric tube, intravenous ceftriaxone one gram 12 th hourly and metronidazole 500 mg 8 th hourly. The patient and her relatives were informed about the options of radiotherapy and chemotherapy and the necessity of an esophageal stenting for palliation of the malignancy but she died on the fourth day of treatment from the worsening pneumonia. Discussion Elderly patients presenting with dysphagia pose an important clinical challenge to physicians. Esophageal neoplasm is a serious concern in such patients unless proved otherwise by invasive clinical evaluation. Of the multitude of causes for dysphagia, aortic aneurysms causing compression of the esophagus resulting in dysphagia aortica is rather uncommon. [1] Atherosclerosis is associated with chances of development of aneurysms of descending aorta. [3] Multiple areas of calcification in the aorta, seen in radiological imaging, point towards an atherosclerotic etiology for the aneurysm in this patient. More so, she had risk factors for atherosclerosis such as advanced age, hypertension and history of smoking. Worsening of dysphagia in this patient had been related to development of the esophageal malignancy. Smoking is a proven etiologic factor in the development of squamous cell carcinoma of the esophagus. [4] Even though this patient had stopped smoking four years earlier, previous smoking could have predisposed to her esophageal cancer. Another possible predisposing factor for the development of cancer might have been chronic food stasis related to the dysphagia aortica that functionally mimics achalasia cardia, a known premalignant codition for esophageal squamous cell carcinoma. Achalasia cardia, which causes esophageal food stasis, can induce chronic hyperplastic esophagitis and eventually malignant transformation of esophageal epithelial cells. [5] Dysphagia for both liquids and solids implies advanced obstruction to the esophagus. Ono′s sign, coughing while swallowing, should alert the physician about the possibility of an acquired esophago-airway fistula. Cough and choking spells while swallowing and development of pneumonia were the results of an acquired esophago-bronchial fistula in this case. Recurrent aspiration and pneumonia, food particles in expectorated material and fear of drinking fluids because of choking spells are the classical features of an esophago-airway fistula. [2] Acquired esophago-airway fistulae can result from both malignant and nonmalignant causes. A majority of them results from malignancy of the esophagus but can also result from tumors of the lung, trachea, larynx, thyroid and lymph nodes. [2] Nonmalignant diseases that can cause acquired esophago-airway fistulas are prolonged tracheal intubation, ingestion of corrosives, blunt and penetrating chest trauma, granulomatous mediastinal infections, prior surgery on esophagus and tracheobronchial tree, iatrogenic injuries, indwelling stents and AIDS. [2] Regardless of the etiology, the important life-threatening complications from esophago-airway fistulae are pulmonary infections and poor nutrition. Once they are diagnosed, urgent treatment is warranted, the delay of which results in catastrophic pulmonary complications. Surgical correction of nonmalignant esophago-airway fistulae gives good results and the recurrences are uncommon. [6] There is no cure for malignant esophago-airway fistulae and palliative procedures like esophageal stenting, esophageal exclusion, esophageal bypass, fistula resection and repair may prolong survival. [2],[7] Insertion of a coated self-expandable metal stent is the treatment of choice for an individual with malignant esophago-airway fistula. [8] Radiotherapy and or chemotherapy also offer effective palliation and the median survival time had been prolonged with closure of few fistulae in a reported series. [9] Without treatment the median survival time may be one to six weeks [2],[7] and aspiration pneumonia is the usual cause of death. References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07028f1.jpg] |
| |||||||||

{kind=link}