 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 111-115 Technical Report Retrospective analysis of role of interstitial brachytherapy using template (MUPIT) in locally advanced gynecological malignancies Pooja K Nandwani, Rakesh K Vyas, JP Neema, Unnikrishan K Suryanarayan, Devang C Bhavsar, Kinjal R Jani Department of Radiation Oncology, Gujarat Cancer and Research Institute, Ahmedabad Code Number: cr07029 Abstract Aim : The aim of this retrospective study was to assess treatment outcomes for patients with locally advanced gynecological malignancies being treated with interstitial brachytherapy using Martinez universal perineal interstitial template (MUPIT) and to study the acute and late sequelae and survival after treatment by this technique.Materials and Methods : Ninety seven patients untreated with histopathological confirmation of carcinoma of cervix (37) vault (40) and vagina (20) were treated by combination of external beam RT (EBRT) using megavoltage irradiation to pelvis to dose of 4000-5000 cGy followed by interstitial brachytherapy using MUPIT between September 2001 to March 2005. Median age was 46 years. Only those patients who were found unsuitable for conventional brachytherapy or in whom intracavitatory radiotherapy was found to be unlikely to encompass a proper dose distribution were treated by interstitial template brachytherapy using MUPIT application and were enrolled in this study. The dose of MUPIT was 1600-2400 cGy in 4-6# with 400 cGy /# and two fractions a day with minimum gap of six hours in between two fractions on micro-HDR. Criteria for inclusion of patients were as follows: Hb minimum 10 gm/dl, performance status - 70% or more (Karnofsy scale), histopathological confirmation FIGO stage IIB-IIIB (excluding frozen pelvis). Results : Among the 97 patients studied, 12 patients lost to follow-up and hence they were excluded from the study. Follow-up of rest of the patients was then done up to September 2006. The duration of follow-up was in the range of 20-60 months. Parameters studied were local control rate, complication rate, mortality rate and number of patients developing systemic metastasis. Local control was achieved in 56/85 (64.7%) and complication rate was 15/85 (17.6%). Local control was better for nonbulky tumors compared bulky tumors irrespective of stage of disease. Local control was better in patients with good regression of disease after external beam radiotherapy. Time of gap between EBRT and implant also had an impact on the outcome. Conclusion : Interstitial template brachytherapy by MUPIT is a good alternative to deliver high dose radiation in locally advanced gynecological malignancies where conventional brachytherapy application is either not feasible or likely to give optimal dose distribution. Loco regional control obtained is definitely better than EBRT alone and within the accepted range of complications. Keywords: Interstitial brachytherapy, locally advanced gynecological malignancies, Martinez universal perineal interstitial template Introduction Gynecological malignancies are a sizeable proportion of all the cancers among female population in India. Majority of patients have locally advanced disease at time of presentation stage IIB- IVA. Radiotherapy plays a very important role in overall management of these cancers both in early stages as well as locally advanced stages. [1],[2] It may be delivered as pelvic external beam RT (EBRT) and / or brachytherapy. External beam pelvic radiotherapy generally precedes brachytherapy as it helps in sterilizing the nodal metastasis and shrinking the primary tumor for an optimal brachytherapy application later on. Although cervix and vagina can tolerate a high radiation dose, it is not possible to deliver high dose by EBRT without causing damage to neighboring dose limiting vital structures like urinary bladder and rectum. Brachytherapy plays a vital role here as it helps in escalating the radiation dose to primary tumor area yet sparing the surrounding normal tissues resulting in improved tumor control probability and with minimum morbidity. Intracavitatory radiotherapy (ICRT) and central vaginal cylinder (CVC) are conventionally employed to deliver a very high dose to cervix and vagina with minimal dose to rectum and bladder. Thus it achieves a very good cure rate with acceptable morbidity. Though ICRT is the standard technique of brachytherapy used for cervical carcinoma, interstitial brachytherapy is recommended for some cases in which either ICRT is expected to result in a suboptimal dose distribution or it is technically not possible. Some of the indications of interstitial implantation are: [3],[4],[5]
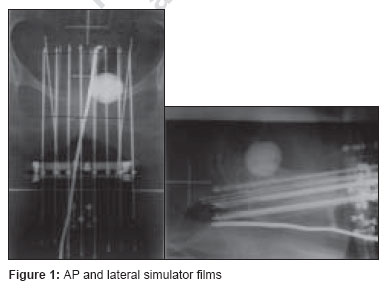
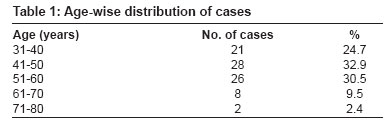
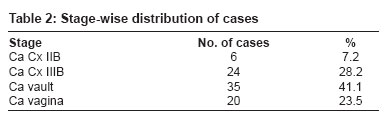
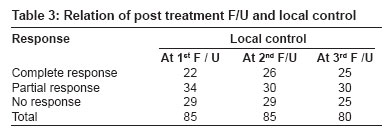
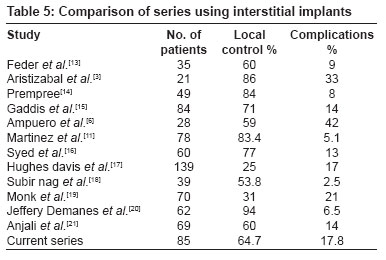
Materials and Methods Between September 2001 to March 2005, 97 patients were taken for MUPIT and the study of these patients was done retrospectively and traced till September 2006. Out of these 37 patients were of carcinoma cervix, 40 of carcinoma of vault and 20 of carcinoma of vagina. All the patients were treated with combination of EBRT followed by interstitial brachytherapy using MUPIT applicator. Since 12 patients were lost to follow-up, 85 patients were finally studied. 30 out of which were of carcinoma of the cervix, 35 of carcinoma of the vault and 20 of carcinoma of vagina. All patients underwent examination under anesthesia, biopsy and routine workup before treatment. All patients received EBRT 4000-5000 cGy midplane in 20-30 # with 180-200 cGy /#, five days a week to whole pelvis by either anterior and posterior parallel opposed portals or four field technique on cobalt 60 or dual energy linear accelerator. All patients were examined under anesthesia one to two weeks after completion of EBRT and evaluated for response to EBRT and labeled as: Complete response (CR) = complete regression of tumor Patients were also evaluated for ICRT/CVC. Only those patients who were found unsuitable for ICRT/CVC or in whom ICRT was found to be unlikely to encompass the tumor volume were treated with interstitial brachytherapy using MUPIT applicator and were enrolled for this study. Hemoglobin minimum 10 gm%, performance status 70% or more (Karnofsky scale) or 0-2 (ECOG), histopathological confirmation, FIGO stage IIB-IIIB (excluding frozen pelvis). Preimplant procedure Implant procedure Epidural catheter was maintained for postoperative pain management. Pervaginal examination under anesthesia was performed to assess the dimensions of the tumor, parametrial and paravaginal tissue involvement and relationship of the tumor to the uterus and other pelvic organs. The inferior extent of tumor was done with silver markers. Foley′s catherisation was done with 7 ml of diatriazoate (urograffin) pushed into its bulb. A stay suture was taken over anterior lip of cervix or anterior fornix with a long thread held outside by artery forceps. This was used to fix the structures. While inserting needles a guide needle was inserted mostly through the posterior vaginal wall with one finger in the rectum. The tip of this needle was taken 1-2 cm beyond the clinically palpable disease. Vaginal length was determined and vaginal cylinders were fixed to the template at that length. The cylinder was then inserted in the vagina with the guide needle in one of its groove. The template was then secured to the perineum by means of stitches through peripheral holes. The remaining needles were placed around the vaginal cylinders up to the preset depth. The number and position of needles were according to the extent of the disease. Needles were bilaterally symmetrical in most of the cases. Thereafter check cystoscopy was done and if any needle was found in the urinary bladder, that needle was removed. Thorough examination was done per rectally to confirm that no needle has pierced the rectal mucosa. The rectal plate was attached with the rest of the template to complete the assembly; rectal tube (modified malecot catheter) was pushed through the lowermost central hole. The cover plate was fixed over the template assembly. Packing was done with gauze pieces soaked in betadine solution. Treatment planning Implant was removed after completion of treatment. Throughout the treatment period, adequate antibiotic coverage was given and hydration of patient was maintained. Analgesia in the form of 60 mg of morphine was given through the epidural catheter, twice a day. Post implant follow-up Grading of reaction Grade 2: Severe and/or persistent episodes of proctosigmoiditis, cystitis, etc, that respond to conservative treatment but requires hospitalization. Grade 3: Fistula formation and complications that require surgical intervention. Results This is a retrospective study of 97 patients of locally advanced gynecological malignancies. As 12 patients were lost to follow-up, they were excluded from the study. The proportion of cases was 30 cases of cancer cervix, 35 of cancer vault and 20 cases of cancer of vagina. Majority of patients were in fourth and fifth decade of life. The age of patients ranged from 34-74 years. Age wise distribution is shown in [Table - 1]. Stage wise distribution is shown in [Table - 2]. Majority of patients were epidermoid carcinoma, moderately differentiated. All patients were given external beam radiotherapy 4000-5000 cGy in 20-30 # over -four to five weeks and assessed for response after -one to two weeks. Partial response was observed in 30 (35.2%) and complete response in 26 (30.5%) patients. Patients who were technically not suitable for intracavitary application or had bulky tumors, which were unlikely to be encompassed sufficiently by intracavitary application, were taken for interstitial implant. These patients were delivered a dose of 16 - 24 Gy in 4-6 #, 4 Gy / #, 2 # per day with minimum of six hours of gap between two fractions. All patients were followed-up monthly and the follow up period was in range of 20-60 months. Local control was 56 (65.8%) at three month follow-up which is shown in [Table - 3] cases showing persistent disease in third month never achieved local control. Local control in relation with stage is shown in [Table - 4]. Five patients developed systemic metastasis. Four patients developed liver metastasis. All of them were offered palliative chemotherapy. One of them was locally free but died when traced till the last follow-up. Rest three was in NR group out of which two also expired when traced to the last follow-up. One patient who had partial response developed supraclavicular LN 1.5 years later and was offered palliative RT (20 GY / 5 #) for the same. Two patients of NR group had progression of disease and both of them had later developed VVF. And when traced till the last follow-up, they had expired. The time gap between EBRT and implant also had an impact on the outcome. In cases with gap < or equal to 25 days, local control was better then those having > 25 days gap. Complications Discussion Standard treatment for advanced gynecological malignancies consists of combination of external beam radiotherapy and brachytherapy. External beam radiotherapy is fractionated over several weeks, usually conventional fractionation with 180 to 200 cGy per fraction with the aim of reducing the tumor to a size, which can be irradiated more effectively with brachytherapy. However, not infrequently and despite doses as high as 5000-6000 cGy by EBRT, tumor regression is only partial, leaving the tumor unsuitable for conventional brachytherapy. Conventional intracavitary applicators (tandem and ovoids) deliver a large central dose with rapid dose fall off towards the periphery. It offers the advantage of homogenous dose distribution to the tumor volume but spares the surrounding normal organs and tissues. Also, with intracavitary application, treatment can be completed over a shorter time compared to EBRT. Brachytherapy is delivered using either LDR or HDR afterloading techniques. The central dose in these applications is represented by "point A" (which is defined as 2 cm above and lateral to the cervical collar top) and peripheral dose by "point B" (which is 3 cm lateral to point A). If 100% dose is given to point A, only a 30% dose is delivered to point B. Bladder and rectum tolerance become a limiting factor in an effort to increase the dose at point B. In advanced disease, the problem is still compounded by two factors: a. Significant parametrial disease extending up to lateral pelvic wall with high incidence of positive pelvic nodes. b. Distortion of local anatomy (improper geometry) with the resultant interference in placement of applicators. If at all treatment is delivered using standard intracavitary applicators, dose distribution curve does not encompass the tumor volume properly. These limitations have long been recognized to be responsible for the lack of effectiveness of this treatment modality in advanced cases. A number of retrospective analysis in the past showed that most of tumor recurrence especially in locally advanced cases occurred in pelvis after conventional tandem and ovoids treatment. Templates were therefore invented which not only determined the position of needles but also their course inside the tumor. Primarily, these templates consist of a central large hole for placement of tandem and an array of small holes around this large hole for insertion of needles. Syed-Neblett parametrial butterfly and Martinez Universal Parametrial Interstitial Template have been the two major innovations in this direction. Most of the studies were conducted using these two templates and their prototypes. The radionuclides used are Iridium 192 [13],[14] and Iodine 125. When the perineal interstitial implant is combined with ICRT, the uterine tandem is attached to the suitable brachytherapy equipment and the interstitial template loaded separately with radioactive sources. When perineal interstitial implant was used after EBRT, a dose of 2000 or 3000 cGy is delivered in 4-6 fractions. Thus, the procedure may last for a period of three to six days and the whole applicator system may cause pain and discomfort to the patient. The major studies are listed in the [Table - 5]. Martinez et al. constructed a multipurpose template, which could be used for a variety of perineal malignancies. It has the provision of both central tandem and central needle either of which could be used justifiably for optimal dose distribution simultaneously taking care of bladder and rectal tolerance. Martinez et al. achieved the local control in 84%, with complication rate as low as 5% in a group of 78 patients with advanced gynecological malignancies. In our study, brachytherapy was delivered with high activity (10 Ci) Ir 192 stepping source using microselectron HDR. All our patients received EBRT 4000-5000 cGy, 180-200 cGy per fraction, five fractions per week followed by interstitial brachytherapy using MUPIT applicator within three to four weeks of EBRT. An indication of interstitial brachytherapy in most of our patients was either nonnegotiable cervical os or partial response to EBRT with bulky residual disease unlikely to be encompassed by ICRT. Planning at our setup was done according to stepping source dosimetry system using the computer program PLATO TPS. Geometric and dose point optimization was used for uniform dose distribution to tumor area. Total dose delivered by brachytherapy ranged from 1600 to 2400 cGy, 400cGy per fraction in four to six fractions. Two fractions were delivered in 24h with a minimum gap of six hours between two fractions. In our study local control was achieved in 56 cases (64.7%), which is comparable to other studies. Five patients (5.8%) had systemic metastasis. Four had liver metastasis and one had supraclavicular metastasis. Complication rate was 17.6%, which was also comparable to other studies. This is shown in [Table - 5]. Conclusion
References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07029t2.jpg] [cr07029t4.jpg] [cr07029t3.jpg] [cr07029t1.jpg] [cr07029t5.jpg] [cr07029f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}