 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
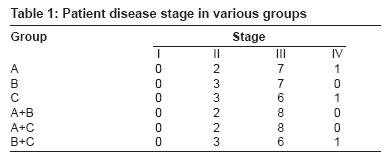
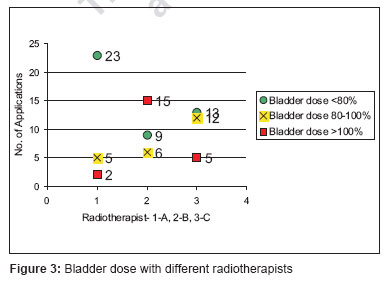
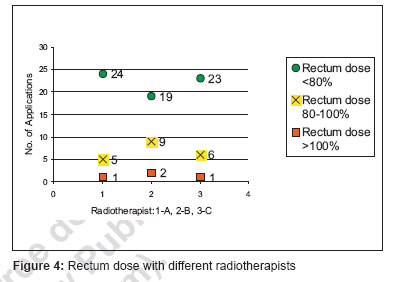
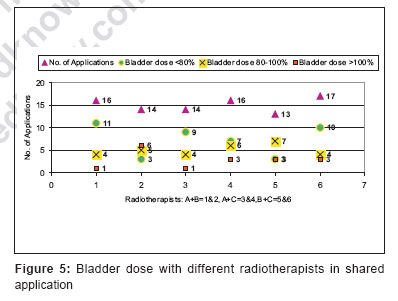
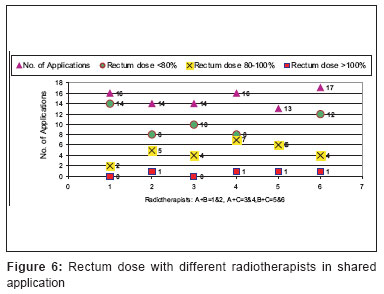
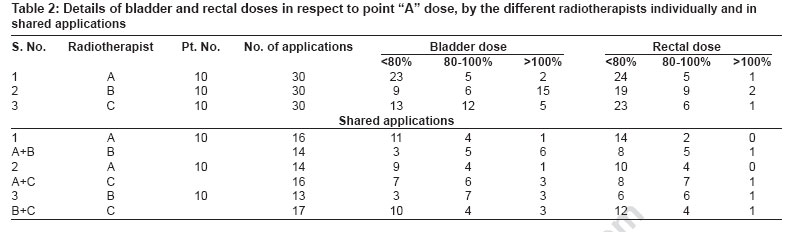
Journal of Cancer Research and Therapeutics, Vol. 3, No. 2, April-June, 2007, pp. 116-120 Technical Report High-dose-rate-intracavitary brachytherapy applications and the difference in the bladder and rectum doses: A study from rural centre of Maharashatra, India Vandana S Jain, Mukund B Sarje, Kailash K Singh, R Umberkar, Rajeev Shrivastava, Shailendra M Jain Department of Radiotherapy and Clinical Oncology, Pravara Rural University (Deemed University), Loni, BK - 413 736, Ahmednagar Code Number: cr07030 Abstract Aim : To report the difference in the bladder and rectum doses with different applications by the radiotherapists in the same patient of the carcinoma of the uterine cervix treated by multiple fractions of high-dose-rate (HDR) intracavitary brachytherapy (ICBT).Materials and Methods : Between January 2003 to December 2004, a total of 60 cases of the carcinoma uterine cervix were selected randomly for the retrospective analyses. All 60 cases were grouped in six groups according to the treating radiotherapist who did the HDR-ICBT application. Three radiotherapists were considered for this study, named A, B and C. Ten cases for each radiotherapist in whom all three applications were done by the same radiotherapist. And 10 cases for each radiotherapist with shared applications in the same patient (A+B, A+C and B+C). The bladder and rectal doses were calculated in reference to point "A" dose and were limited to 80% of prescribed point "A" dose, as per ICRU-38 recommendations. Received dose grouped in three groups- less then 80% (<80%), 80-100% and above 100% (>100%). A total of 180 applications for 60 patients were calculated for the above analyses. Results : There is a lot of difference in the bladder and rectal doses with the application by the different radiotherapists, even in the same patient with multiple fractions of HDR-ICBT. Applications by 'A' radiotherapist were within the limits in the self as well as in the shared groups more number of times, by 'B' radiotherapist was more times exceeding the limit and by 'C' radiotherapist doses were in between the A and B. Discussion and Conclusion : For the rectal and bladder doses most important factors are patient's age, disease stage, duration between EBRT and HDR-ICRT and patient anatomy, but these differences can be minimized to some extent by careful application, proper packing and proper fixation. Keywords: Carcinoma cervix, high-dose-rate brachytherapy, radiotherapy Introduction Carcinoma of the uterine cervix is the most common malignancy in women in developing countries, such as India. [1] As most of the cases present at advanced stages such as stage III and IV, in which surgery is not possible, radiotherapy plays an important role. [2],[3],[4],[5],[6],[7] Radiation has been used successfully to treat cervical cancer for nearly a century. The combination of external beam irradiation and brachytherapy has been shown to be an effective treatment for carcinoma cervix patients. Success of brachytherapy requires delivery of a high radiation dose to the tumor while sparing the surrounding normal tissue to some degree. It has been used clinically for many countries. Carcinoma uterine cervix (Ca. Cx.) is the commonest malignancy in females reported in our center. Our hospital is situated in the rural area of Maharashtra, India, with the facility of one Cobalt unit, HDR / PDR remote after loader unit and a treatment planning system. The department was started in Aug.1996. This study is aimed to evaluate the differences in the bladder and rectal doses with different applications by radiotherapists in the same patient of the carcinoma of the uterine cervix treated by multiple fractions of high-dose-rate (HDR) intracavitary brachytherapy (ICBT). Brachytherapy treatment was delivered by HDR / PDR remote after loader unit, in which single high stepping iridium ( 192 Ir) source of 10ci with active dimensions of 0.6 mm diameter and 3.5 mm length. The source is encapsulated in a stainless steel capsule, which forms a total diameter of 1.1 mm and 5.1 mm length. The source is present at the tip of the drive cable of the same outer diameter. Motor drives the cable with source from distal end of the applicator (from first position) to proximal end (last position). Dwell positions can be adjusted from 1 mm to 10 mm apart, according to the desired treatment plan and dwell times can be adjusted to 0.1 sec. to 999 sec. Materials and Methods Between January 2003 to December 2004, a total of 60 cases of the carcinoma uterine cervix, which completed their EBRT and HDR-ICBT in time, were selected randomly (by simple random sampling with replacement) for each six groups (10 patients in each group). Groups were made according to the treating radiotherapists who did the HDR-ICBT application. Three radiotherapists were considered for this study, named A, B and C. 10 cases for each radiotherapist in which all the three applications were done by same radiotherapist. And 10 cases for each radiotherapist with shared applications in the same patient (A+B, A+C and B+C). All were histopathologically confirmed cases. All cases were investigated for routine hematological, biochemical examination, X-ray chest and Ultrasonography of the abdomen and pelvis before starting radiotherapy treatment. All patients were examined and staged clinically according to the International Federation of Gynecologists and Oncologists (FIGO) staging system. Stage of the disease is shown in [Table - 1]. Radiation therapy: All patients had external beam radiotherapy by anterior- posterior / posterior- anterior (AP / PA) or four field box technique with cobalt 60 unit. Patients were treated to mid plane dose on AP / PA and at isocenter on four field box technique. Dose delivered was 5000 cGy - 5040 cGy in 25-28 fractions with five fractions per week, for five to six weeks duration without any midline block. Brachytherapy: After completion of external radiotherapy the cases were planned for brachytherapy after 12 to 18 days interval. All cases were given three fractions of HDR-ICBT at weekly interval. Fixed length three channel Fletcher applicator insertion was done under general / spinal anesthesia. A Foley′s catheter was inserted and balloon was filled by 7 cc diluted Urograffin to identify the bladder neck region. A rectal catheter with lead wire inside it was inserted in rectum to visualize rectal mucosa for rectal points. After applicator insertion, vagina was packed by regular betadine soaked gauze packs to push bladder and rectum away and stabilize the applicator by fingers / forceps [Figure - 1]. Once the procedure was over, the applicator is fixed to the table and no movement of the patient is allowed till her treatment was over [Figure - 2]. AP and lateral semi-orthogonal marker X-ray films with the help of jig were taken by C- arm at the same place for all insertions. Semi-orthogonal X-ray films were reconstructed and planning was done with the help of the Abacus treatment planning system (Program version-3.1; Germany). Dose was prescribed to point "A". Point "A" is described as a point 2 cm up from the cervical os point of the uterine tube (tandem) and 2 cm lateral to the uterine source. Dose to urinary bladder and rectum were calculated by bladder and rectal reference points. Bladder reference points were marked on the anterior radiograph at the center of the balloon and on lateral radiograph a antero-posterior line was drawn through the Foleys catheter balloon center and the bladder reference point was taken on this line at the posterior surface of the balloon (as per ICRU-38). For rectal reference points we used rectal catheter with a marker lead wire inside [9] is not the ideal recommendation as per ICRU-38, but for convenience and cost effectiveness this is used. Multiple rectal reference points are delineated on the lateral radiograph. For R1 rectal point in lateral radiograph an anterior-posterior line was drawn through lower end of the uterine source to 5 mm anterior to the rectal marker. Four more rectal points R2, R3, R4 and R5 were taken 1-1 cm above and below the R1 point respectively. In anterior radiograph rectal point R1 was taken at the lower end of inter uterine source and four more rectal points R2, R3, R4 and R5 were taken 1-1 cm above and below the R1 point respectively. All points were in the line of the rectal marker. Doses delivered were 21 Gy to point "A" by HDR, in three fractions at weekly interval (per fraction dose was 7 Gy). Bladder and rectum doses were limited to 80% of prescribed point "A" dose, (as per ICRU-38 recommendations). The bladder and rectal doses were calculated in reference to point "A" dose and grouped in three groups- Dose less then 80% (< 80%), 80-100% and above 100% (>100%). Total 180 applications for 60 patients were analyzed for bladder and rectum doses for the above mentioned six groups of treating radiotherapists. Results There were 10 cases in each six groups. The stage of disease in each group is shown in [Table - 1]. The bladder and rectal doses were calculated in reference to point "A" dose and grouped in three groups- Dose less then 80% (< 80%), 80-100% and above 100% (>100%). In total 180 applications for 60 patients were calculated for the above analyses. The bladder dose for 30 applications for 10 patients by A, B and C radiotherapists were below 80% in 23, 9 and 13 applications, 80-100% in 5, 6 and 12 applications and above 100% in 2, 15 and 5 applications respectively [Figure - 3]. The rectal doses for 30 applications for 10 patients by A, B and C radiotherapist were below 80% in 24, 19 and 23 applications, 80-100% in 5, 9 and 6 applications and above 100% in 1, 2 and 1 applications respectively [Figure - 4]. The shared applications for 10 patients by A+B radiotherapists were 16+14 respectively. The bladder dose for shared 30 applications by A and B radiotherapists were below 80% in 11 and 3 applications, 80-100% in 4 and 5 applications and above 100% in 1 and 6 applications respectively. The rectal doses for the same shared 30 applications were below 80% in 14 and 8 applications, 80-100% in 2 and 5 applications and above 100% in 0 and 1 application respectively. The shared applications for 10 patients by A+ C radiotherapists were 14+16 respectively. The bladder dose for shared 30 applications by A and C radiotherapists were below 80% in 9 and 7 applications, 80-100% in 4 and 6 applications and above 100% in 1 and 3 applications respectively [Figure - 5]. The rectal doses for the same shared 30 applications were below 80% in 10 and 8 applications, 80-100% in 4 and 7 applications and above 100% in 0 and 1 applications respectively. The shared applications for 10 patients by B+C radiotherapists were 13+17 respectively. The bladder dose for shared 30 applications by B and C radiotherapists were below 80% in 3 and 10 applications, 80-100% in 7 and 4 applications and above 100% in 3 and 3 applications respectively. The rectal doses for the same shared 30 applications were below 80% in 6 and 12 applications, 80-100% in 6 and 4 applications and above 100% in 1 and 1 applications respectively [Figure - 6]. Details of all applications are shown in [Table - 2].Discussion Radiotherapy is an effective treatment modality for all the stages of carcinoma of the cervix and is widely used in developing countries. [1] The success of brachytherapy requires delivery of high radiation dose directly to the tumor, while sparing to some degree, the surrounding normal tissues. [8] Though HDR- ICRT (HDR-ICBT) is an acceptable, efficient and safe alternative to traditional low dose rate (LDR) - ICRT requires multiple applications. American Brachytherapy Society (ABS) recommends multiple HDR insertion for progressive tumor volume reduction, allowing more effective disease coverage with subsequent applications. 4 to 8 fractions of HDR- ICRT with dose range from 5.3 to 7.5 Gy per fraction and total dose by EBRT from 20 Gy to 50.4 Gy to early and late stages of diseases and ICRT is given during EBRT (but EBRT is not given on the day of HDR). [2] At our setup, treatment plan for three fractions of HDR-ICBT after completion of EBRT is preferred as the patients were uneducated and financially poor. In an institute like ours where three - four radiotherapists work, the same radiotherapists did not compulsorily do the different applications for the same patient. This was observed that the difference is always there, even though the same radiotherapist for the same patient does the application and this is more if done by other radiotherapist. If we exclude the patient factors, the other probable reasons for this difference might be difference in technique while putting the applicator (size of the ovoids), packing by finger (instead by plan forceps, as forceps can reach to the required depth above and below the ovoid) and lastly the most important is after the application and packing the fixation of applicator which is always ignored. Dose to point "A" is commonly used for prescribing and reporting in gynecological radiation therapy and this point is related to applicator positioning, thus applicator position plays an important role in reference to bladder and rectum doses. One can try to reduce the bladder and rectum doses by changing dwell position, dwell times and step distance with the help of the computers and various planning systems, but this has its own limitations. Although in all cases with more then 80% of the prescribed point "A" dose, the total dose was reduced to 18 Gy and 15Gy in three fractions, in 80-100% and> 100% groups respectively. Total prescribed point "A" dose by EBRT and HDR-ICBT in all cases ranged from 65-71Gy. In cases with> 100% of the prescribed point "A" dose bowel and bladder complications were slightly more. There is lot of difference in the bladder and rectal doses with the multiple applications by the different radiotherapists, even in the same patient. Applications by ′A′ radiotherapist were within the limits in self as well as in shared groups more number of times, by ′B′ radiotherapist was more times exceeding the limit and by ′C′ radiotherapist doses were in between the A and B. For the rectal and bladder doses most important factors are patient age, disease stage, duration between EBRT and HDR-ICBT and patient anatomy, but these differences can be minimized to some extent by careful application, proper packing and proper fixation. Acknowledgement I was helped by the excellent institutional facility in rural Maharastra, India, especially for the poor. To submit this article I was helped by Mr. Sanjeev Kulkarni, Dr. Swati Chaudhary and my husband Dr. S.M. Jain. I thank them all sincerely. References
Copyright 2007 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr07030f2.jpg] [cr07030f5.jpg] [cr07030f4.jpg] [cr07030t2.jpg] [cr07030t1.jpg] [cr07030f3.jpg] [cr07030f6.jpg] [cr07030f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}