 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
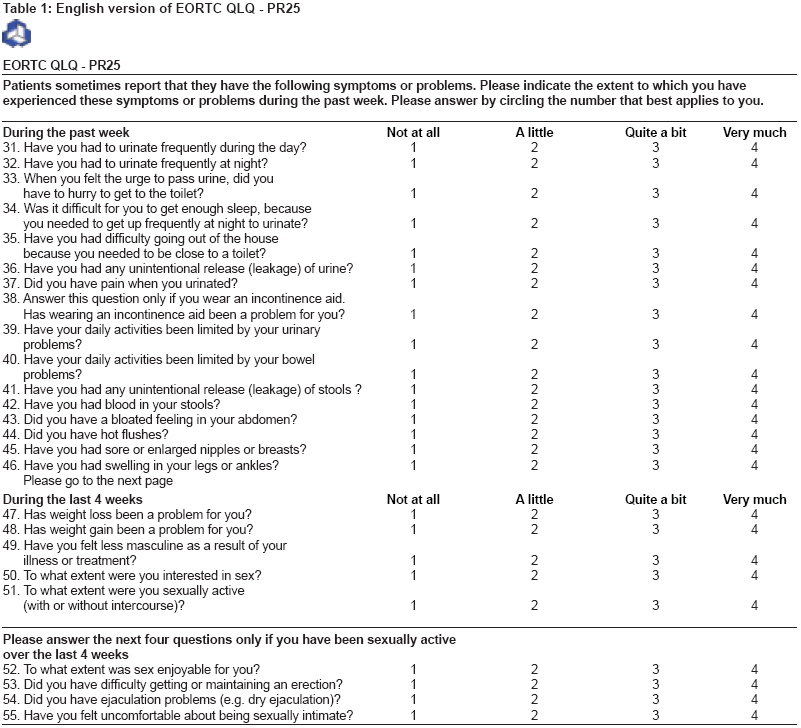
Journal of Cancer Research and Therapeutics, Vol. 4, No. 2, April-June, 2008, pp. 64-69 Original Article The European Organization for Research and Treatment of Cancer prostate-specific quality of life module (PR-25) in Hindi and Marathi: Translation and pilot testing process Wadasadawala Tabassum, Murthy Vedang, Mahantshetty Umesh, Engineer Reena, Shrivastava Shyamkishore, Dinshaw Ketayun Depatment of Radiation Oncology, Tata Memorial Hospital, Mumbai Code Number: cr08019 Abstract Background: The side effects of various treatments for prostate cancer have a measurable impact on the general as well as disease-related quality of life, which is of pivotal concern as an outcome measure.
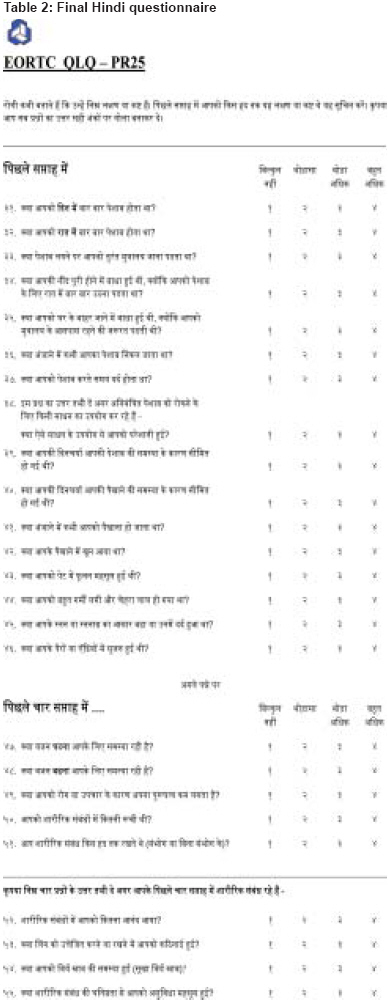
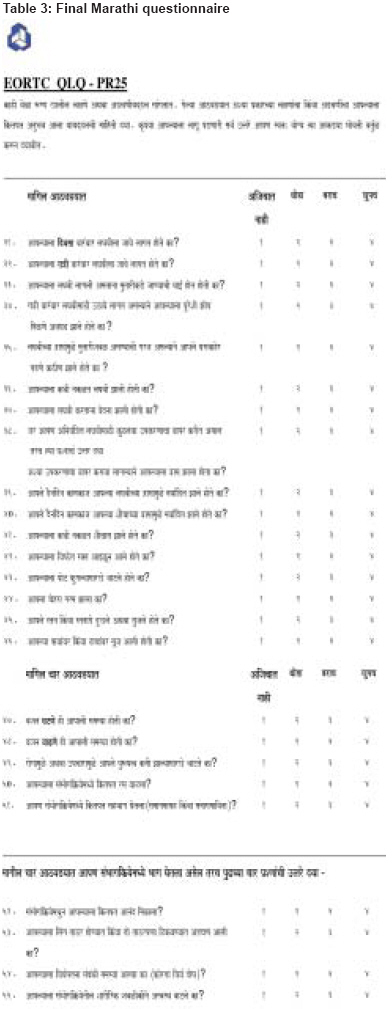
Keywords: Backward translation, European Organization for Research and Treatment of Cancer QLQ-PR25, forward translation, pilot testing Prostate cancer is the most common solid-organ malignancy among North American men, [1] and has traditionally been considered a disease of the West. The incidence of prostate cancer however has been on the rise in recent years in India as indicated by the urban population-based registries. [2],[3] Prostate cancer has now become one of the leading types of cancer in urban India. It is now the third commonest cancer in Delhi (previously eighth), fourth in Mumbai (previously eighth), fifth in Bangalore (previously seventh), and has maintained its ninth position in Chennai. The adoption of western culture by the native population and increasing urbanization are thought to be behind this increasing trend in urban areas. This is similar to the increasing incidence of breast cancer (surpassing cervical cancer) in urban females. [2],[3] Although the traditional measures of disease outcome like response to treatment, control of symptoms, clinical or biochemical relapse, and survival are important in prostate cancer, health-related quality of life (HRQOL) is an equally relevant clinical end point. A wide array of treatments are available for different stages of the disease and almost all of these result in significant sexual, urinary, and bowel dysfunction, with persistence of treatment-related morbidity for prolonged periods due to the relatively long survival of most patients. These side effects of treatment are bound to have a measurable impact on the general as well as disease-related QOL. Measuring HRQOL, in addition to measurement of survival outcomes, enriches clinical research and may be decisive when the effects of different treatments on the traditional end points are similar or minimal. QOL instruments are now a part of most prospective or cross-sectional studies. Various QOL instruments are available that assess prostate-specific symptoms like Functional Assessment of Cancer Therapy-Prostate (FACT-P) cancer subscale, Expanded Prostate Cancer Index Composite (EPIC), an expanded version of the University of California, Los Angeles, Prostate Cancer Index (UCLA-PCI), International Prostate Symptom Score (IPSS), European Organization for Research and Treatment of Cancer (EORTC)-Prostate Cancer Module (EORTC-QLQ-PR25), etc. All of these questionnaires are self-administered, as QOL evaluation mandates the use of patient-administered and, ideally, validated instruments, because physician ratings of patient symptoms do not correlate well with patient self-assessments of QOL. [4] Unfortunately, most of the standard questionnaires are available only in English and thus of no use for the non-English-speaking population. In view of a dearth of QOL data in Indian patients due to the lack of an appropriate QOL instrument in the local language, we decided to undertake the translation of the English version of EORTC-QLQ PR 25 into Hindi (national language) and Marathi (local language in Maharashtra state) as it is the most widely used prostate cancer-specific QOL module in clinical studies. This paper describes the translation methodology in detail including the problems faced, how those problems were overcome, and how the results of the pilot testing specific to Indian population were interpreted. We aimed to formulate an appropriately translated and acceptable questionnaire in Hindi and Marathi languages. Materials and Methods The EORTC QLQ PR-25 module has not been translated or tested in Hindi or Marathi. We confirmed with the EORTC QL unit that the translation of the EORTC QLQ PR-25 module in Hindi and Marathi was not currently under preparation. The translation was performed as per the second edition of the EORTC Quality Of Life Group Translation Procedure. The EORTC-QLQ PR-25 is designed to be used along the EORTC-QLQ C-30, which is a core questionnaire assessing general QOL, and consists of 30 questions. The EORTC-QLQ PR-25 consists of 25 questions numbered 31 to 55 [Table - 1]. In order to maintain uniformity of wording for the same item across different modules as mentioned in the translation manual of the EORTC, the item numbers 44, 49, 50, 51, and 52, which were available in Hindi and Marathi from previous translations, were not translated. Likewise, preexisting translations of the instructions and response categories were also available in Hindi and Marathi and so the original wording of these was accepted. The final Hindi and Marathi version of EORTC PR-25 module is the result of a translation process comprising of the following steps: Forward translation from English to Hindi and Marathi 1. Two forward translations of the original English questionnaire into Hindi and Marathi were done by two native speakers of the respective languages who were also fluent in English. These translators included both oncologists and non-oncologists. 2. After discussions between the translators and the local project coordinator, the first intermediary questionnaire for Hindi and Marathi were formulated. Backward translation from Hindi and Marathi to English 3. Two backward translations of the first intermediary questionnaire into English were done by two independent translators. 4. The second intermediary questionnaire was the outcome of comparison of the backward translations with the original English questionnaire followed by appropriate modifications. Pilot testing in patients with prostate cancer 5. This second intermediary questionnaire was then administered to ten patients who had never seen the questionnaire before. Each patient, after completing the questionnaire, was interviewed by the local project coordinator who questioned them about each item in the second intermediary questionnaire; they were asked whether they was any difficulty in answering, confusion while answering, or difficulty in understanding the questions; whether the questions were upsetting; and whether the patients themselves would have framed the question in a different way. 6. Based on the suggestions or interpretations of this pilot testing, the final Hindi and Marathi questionnaires were formed. Results Forward translation: (Steps 1 and 2) The two independent forward translations were done by a radiation oncologist (SK) and a management executive (RK) in Hindi and by a non-oncologist (AK) and a medical dosimetrist (CT) in Marathi. First intermediary questionnaire: The two forward-translated questionnaires in Hindi and Marathi were evaluated by the project coordinators (authors: TW and VM). If the translations by both the forward translators were identical to each other and were thought to convey the correct meaning from English then no changes were made. Wherever there were differences between the two versions, the points were discussed with the translators to arrive at a consensus regarding the changes necessary. Because the language structure of Hindi and Marathi is significantly different from English, the literal translation of the original English version was sometimes not possible. So we chose or modified the sentences such that a conceptually comparable meaning could be drawn that was as close as possible to the original meaning. We also, on certain occasions, opted to use the vernacular in order to facilitate comprehension. Thus, a first intermediary questionnaire was formed, one each for Hindi and Marathi. In the following text, we discuss the major difficulties encountered in the formation of the first intermediary questionnaire. Question 36: The translation of this question was satisfactory in both the languages but the word ′leakage′ could not be translated as there is no appropriate, easily understandable, and commonly used word for ′leakage′ in either Hindi or Marathi. We omitted it as we did not think there would be much change in the meaning of the question due to its omission. Question 38 and 41: This was a difficult question for translation into Hindi as well as Marathi as there is no appropriate word for ′incontinence aid.′ We therefore accepted the translation, which meant ′uncontrolled urination.′ The Hindi translation, being unsatisfactory, required the formulation of a third intermediate question with substitution of a few words. The Marathi translation by AK was accepted after substitution of the phrase ′laGavaI nakLt na ha} dNaa¹yaa′ with the words ′Ainayai~t laGavaIsaazI′. Question 43: No literal translation of ′bloated feeling′ could be decided upon. It is described in Hindi and Marathi by various meanings, eg, ′formation of gas in stomach′ or ′increase in size of the abdomen′ or ′swelling of the abdomen.′ For Hindi, there was no agreement in the translation between the two translators. We combined both the questions and framed an intermediate one after discussion with both the translators. For Marathi, the question as translated by AK was short and meaningful. To make it even more appropriate, ′flalyaasaarK′ was replaced with ′fgalyaasaarK′. Question 55: It was extremely difficult to translate this question. Neither of the Hindi translators could appropriately translate the words ′sexually intimate′. After a long and exhaustive discussion with the two translators and an official Hindi translator employed at the Tata Memorial Hospital, we agreed that Back translation: (Steps 3 and 4) The intermediate questionnaire in Hindi and Marathi was given separately to two radiation oncologists (SGL and SV for Hindi and YA and BZ for Marathi) working at the hospital. They had never seen the original EORTC PR-25 questionnaire. They were given information regarding the questionnaire and the purpose of the exercise and were requested to back translate the questionnaire into English, formulating the questions in simple English that would be understood by the lay patient population. This exercise was done to review the modifications of the first intermediary Hindi and Marathi questionnaire in the light of the backward translation. Second intermediate questionnaire: The two back translations were comparable to each other and also to the first intermediary questionnaire and the original English questionnaire (both for Hindi and Marathi). So the first intermediate Hindi and Marathi questionnaires did not need any modification and were adopted as the second intermediate Hindi and Marathi questionnaires, respectively. Pilot testing: (Steps 5 and 6) Each of the second intermediate questionnaires (Hindi and Marathi) was then administered to ten patients diagnosed with prostate cancer. These patients had never seen the questionnaire before and were all native Hindi or Marathi speakers. Each patient after completing the questionnaire was then interviewed by the project coordinators. Direct questions were asked about each item with respect to difficulty in answering, confusion while answering, and difficulty in understanding the questions; the patients were also asked if the questions were upsetting in any way and if they would themselves have framed the question in any other way. All patients were well educated and could read and write in the concerned language. All were married and retired from full-time work. Patients with localized, locally advanced, and metastatic cancer, either on postradiotherapy follow-up or currently undergoing radiotherapy, were included. All of them were given explanations about the importance of assessing QOL issues associated with cancer treatment as well as the need to translate the English questionnaires into the local languages. Most of the translated questions were well understood by all patients. There were only few problem questions; these are illustrated below: Question 47 and 48: One patient (DP) in pilot testing for Hindi and two patients (DK and LV) in pilot testing for Marathi stated that they did not have any weight loss or weight gain, so there was no question of any problem arising from it. They said that the question was neither difficult to understand nor confusing or upsetting. On further questioning, they said that these questions presume that one has weight loss or weight gain and the questions are only asked to know whether one is facing any problem from this weight loss or weight gain. For both the languages, we tried to reframe these questions in order avoid such misinterpretation. The new questions were ′D;k otu ?kVuk vki ds fy, leL;k jgh gSS′ and ′′D;k otu c<+uk vkids fy, leL;k jgh gS?′ for Hindi and ′vajana GaTNa hI tumacaI samasyaa hatI ka?′ and ′vajana vaaZNa hI tumacaI samasyaa hatI ka?′ for Marathi. This change was accepted for the final Hindi and Marathi questionnaires. Question 52, 53, 54, and 55: Six patients from each language group did not attempt these questions. They either left these questions blank or wrote that these questions were not applicable to them because of their old age. However, when specifically asked whether the questions were appropriately translated, all six patients stated that there was no difficulty at all in understanding these questions. Only four patients (SuS, KP, DS, and SS from Hindi and EP, LV, SK, and SA from Marathi) answered the questions and none of them encountered any problem. Final questionnaire The final Hindi and Marathi questionnaire which were submitted to the EORTC as the end result of this translation process were formed taking into consideration all the above points. Both the translations have been approved and accepted by the EORTC [Table - 2] and [Table - 3]. Discussion The EORTC QLQ PR-25 module is still under development and thus is being shared only with those groups willing to provide data relevant to the evaluation of its psychometric properties. The module comprises 25 questions that seek to assessing disease symptoms, side effects of treatment, and some specific psychosocial issues of importance to patients with prostate cancer. These 25 questions have been divided into four proposed or hypothesized (not yet finalized) scales or domains pertaining to: urinary symptoms (1-9), bowel symptoms (10-13), treatment-related symptoms (14-19), and sexual functioning (20-25). The full psychometric properties of the module will be published soon by the EORTC after factor analysis. Until this is available, scoring of the module should be done on the basis of information provided by the principal investigator of the module. We tried to fulfill the aim of producing clear (easy to read and understand) and conceptually equivalent translations in the commonly used local languages. The translation procedure described by the EORTC was rigorously followed and the relevant information required was sought from the translation coordinator of the QL Unit. The entire translated questionnaire was well understood by the patients in both the languages and required revision for only two questions following pilot testing. An interesting aspect that we came across (probably not surprising in our population) was that the majority of the patients chose not to answer the questions related to sexual functioning. This could be related to the cultural barriers, especially in elderly patients. Although these questions are important constituents of the overall HRQOL, their relevance in the context of the average Indian population needs to be kept in mind. The entire translation process was written up as a project report separately for Hindi and Marathi and duly submitted to the EORTC. These reports were reviewed by the translation coordinator of the EORTC. Both the translations were finally accepted with the requisite of transferring the copyright for the translated versions to the EORTC. These modules can now be used in various clinical trials on prostate cancer for QOL assessment. Acknowledgment Our sincere thanks to Sajal Kakkar, Rishi Khanna, Sarbani Ghosh, Shilpa Vyas, Atul Kulkarni, Chandrashekhar Tambe, Bhooshan Zade, Yogesh Anap, Deepa Shashikumar, and Minal Parab for their kind help in translations.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08019t3.jpg] [cr08019t1.jpg] [cr08019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}