 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
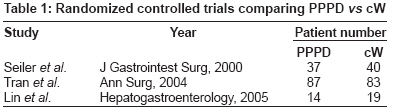
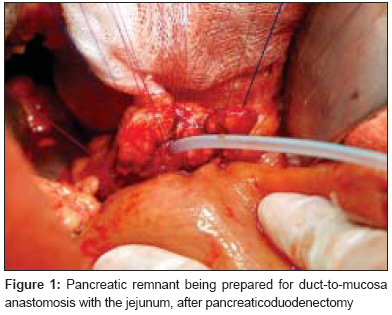
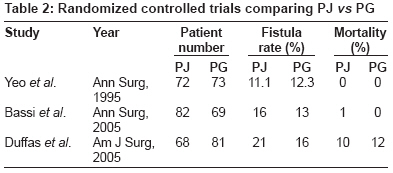
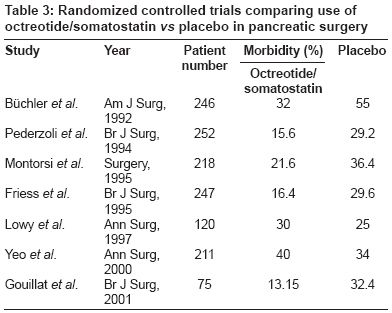
Journal of Cancer Research and Therapeutics, Vol. 4, No. 2, April-June, 2008, pp. 77-83 Review Article Pancreatic resectional surgery: An evidence-based perspective D'souza MelroyA, Shrikhande ShaileshV Department of Gastrointestinal and Hepato-Pancreato-Biliary Surgical Oncology, Tata Memorial Hospital, Mumbai Code Number: cr08021 Abstract A diagnosis of pancreatic cancer carries a very dismal prognosis, with the 5-year survival rate being the lowest of all types of cancer. Surgical resection offers the only hope for cure in these patients. Pancreatic resectional surgery is technically demanding, and while mortality has decreased in centers of excellence, the morbidity remains significant. Numerous controversies exist regarding various aspects of complex pancreatic resections. This review attempts to address these controversies with an evidence-based perspective. We performed a literature search in MEDLINE (www.pubmed.org) with relevant key words and the corresponding MeSH terms. The search was limited to English language publications on human subjects. A manual cross-reference search of the bibliographies of relevant papers was carried out to identify publications for possible inclusion.Keywords: Delayed gastric emptying, distal pancreatectomy, extended lymphadenectomy, octreotide in pancreatic surgery, pancreatic anastomosis, pancreatic duct stenting, pancreatic fistula, pancreatic resections, pancreaticoduodenectomy, segmental pancreatectomy A diagnosis of pancreatic cancer carries a very dismal prognosis, with the 5-year survival rate being the lowest of all types of cancer. Surgical resection offers the only chance for cure for these patients. [1] At diagnosis, more than 85% of pancreatic tumors are at an advanced stage and thus potentially curative resection is feasible in only around 10-15% of patients. [2] The standard procedure for pancreatic head lesions is a pancreaticoduodenectomy (PD), while a distal pancreatectomy (DP) with or without splenectomy is the procedure of choice for body and tail tumors. While hospital mortality after a PD is now <3-5% in experienced centers, postoperative morbidity despite having decreased considerably still remains significant at around 20-30%. [3] Despite improved outcomes after pancreatic surgery, various controversies still exist; for example, pylorus preservation vs antrectomy during a Whipple′s procedure, pancreaticojejunostomy vs pancreaticogastrostomy, use of octreotide in pancreatic surgery, and the role of extended pancreatic resections, segmental pancreatectomy, laparoscopic pancreatic surgery etc. This review attempts to systematically address these issues. Materials and Methods A literature search in MEDLINE ( www.pubmed.org ) was performed with the key words pancreatic resections, pancreaticoduodenectomy, pylorus-preserving pancreaticoduodenectomy, distal pancreatectomy, segmental pancreatectomy, delayed gastric emptying, pancreatic anastomosis, pancreaticojejunostomy, pancreaticogastrostomy, pancreatic duct stenting, octreotide in pancreatic surgery, pancreatic fistula, extended lymphadenectomy, pancreatic cancer, staplers in pancreatic surgery, laparoscopic pancreatic surgery and the corresponding MeSH terms. The search was limited to English language publications on human subjects. A manual cross-reference search of the bibliographies of relevant papers was carried out to identify publications for possible inclusion. Pylorus-preserving pancreaticoduodenectomy (PPPD) vs classical Whipple (cW) [Table - 1] Popularized in 1978 by Traverso and Longmire, [4] it has been postulated that PPPD by preserving the stomach and pyloric function would improve gastrointestinal function and reduce the morbidity associated with an antrectomy and a gastroenterostomy, viz, gastric dumping, biliary reflux gastritis, and ulceration. During the performance of a PPPD, the right gastroepiploic and the right gastric vessels are divided and the duodenum is skeletonized distal to the pylorus. The duodenal bulb is then transected with a stapling device. Criticisms of this surgery have included claims that it is associated with a higher incidence of delayed gastric emptying ((DGE) and that it may be less radical. However, in a study of 140 operative specimens from patients with cancer of the pancreatic head, no extension of tumor tissue adjacent to the pylorus and no lymph node involvement along the lesser and greater curvatures of the stomach could be found. [5] In a prospective, multicenter, randomized study by Tran et al ., PPPD was compared with cW in 170 consecutive patients. [6] Both procedures were comparable with regard to operative time, blood loss, hospital stay, morbidity, mortality, and incidence of DGE. There were also no statistically significant differences between the two groups with regard to overall and disease-free survival. In a recent meta-analysis of 2822 patients by Kocher et al ., both cW and PPPD had similar morbidity rates, with PPPD showing lower mortality and better long-term survival; however, this was not reflected in the subgroup analysis. [7] Thus, in 2008, both PPPD and cW are recommended operations for resectable periampullary and pancreatic head tumors. [8] As a general guideline, cW is reserved for patients with larger, more extensive tumors or for tumors located in the dorsal part of the head of the pancreas or the first part of the duodenum. Pancreatic Anastomosis [Figure - 1] Pancreaticojejunostomy (PJ) vs pancreaticogastrostomy (PG) [Table - 2] Development of a pancreatic fistula after PD is one of the most important causes of procedure-related morbidity and mortality in pancreatic resectional surgery and can result in delayed hemorrhage, local sepsis, wound infection, and DGE. [3],[9] Ductal occlusion using glue and duct ligation have been found to be associated with very high fistula rates and have largely been abandoned. The safe reconstruction of pancreaticoenteric continuity remains a challenge for the pancreatic surgeon. The risk of fistula formation depends on the consistency of the remnant pancreas, the caliber of the main pancreatic duct, pancreatic vascularity, and the technique of construction of the pancreatic anastomosis. [10],[11] The two commonly employed techniques of pancreatic anastomosis are the PJ and the PG. The PJ can be performed by the dunking method or in a duct-to-mucosa fashion. Only a few randomized controlled studies dealing with different surgical techniques for the management of the pancreatic remnant after PD have been published and, of these, only three randomized trials have been performed that have compared PG vs PJ. [12],[13],[14] Earlier uncontrolled studies, such as those published by Takano et al . and Oussoultzoglou et al ., [15],[16] were in favor of PG reconstruction. A PG is said to be easier to perform due to the close proximity of the stomach and is also said to be less prone to ischemia due the rich gastric blood supply. However none of the three randomized controlled trials (RCTs) showed any difference in the overall postoperative complication rate or incidence of pancreatic fistula. However, in the study by Bassi et al ., which involved 151 patients, the incidence of biliary fistula, postoperative collections, and DGE were significantly reduced in patients treated by PG. [13] Two recent meta-analyses have showed that even RCTs had an element of bias and, therefore, no superiority of any one technique could be concluded. [17],[18] Thus, it can be inferred that as long as a duct-to-mucosa tension-free anastomosis between well-perfused tissues is performed, using fine sutures and the consistent practice of a single technique, any type of pancreatic anastomosis should have a good outcome. [3],[19] Role of magnification in pancreatic anastomosis Since a duct-to-mucosa anastomosis is crucial for good outcome, meticulous approximation assumes great importance. Some authors have advocated the use of operating loupes to allow precise construction of the pancreatic anastomosis. Recently Traverso et al ., in a retrospective analysis, highlighted the role of the operating microscope in pancreatic anastomosis. He reported a markedly reduced incidence of pancreatic fistula with the use of the operating microscope as compared to that with the use of the operating loupes. [20] Role of stenting of the main pancreatic duct (MPD) Stenting of the MPD during the performance of the pancreaticoenteric anastomosis facilitates precise placement of mucosal sutures and also diverts pancreatic juice away from the anastomotic site and, in doing so, is said to improve anastomotic integrity. The results using this strategy have been encouraging. [21],[22] In a prospective but nonrandomized trial in 85 patients, Roder et al . [21] demonstrated that stenting of the pancreatic duct reduced the pancreatic fistula rate to 29.3% from 68% and the median hospital stay from 29 to 13 days. An RCT [23] reported that external drainage of the MPD with a stent reduced the rate of pancreatic fistula after a pancreaticoduodenectomy. On the other hand, some studies, including an RCT by Yeo et al ., have shown no benefit of internal stenting in the prevention of pancreatic leakage and exocrine insufficiency. [24],[25],[26] Thus, available evidence is conflicting and practice depends on personal choice and experience. Role of octreotide and somatostatin analogues in decreasing the rate of complications and pancreatic fistula after pancreatic surgery [Table - 3] Octreotide is a synthetic analogue of native somatostatin and, like somatostatin, has been used perioperatively to inhibit pancreatic exocrine secretion. Prospective RCTs conducted in Europe have evaluated the use of subcutaneous octreotide/somatostatin in patients undergoing elective pancreatic resection. [27],[28],[29],[30],[31] These trials concluded that octreotide reduced the incidence of occurrence of pancreatic fistulae and other complications. However, other trials have yielded contradictory results. Studies by Yeo et al . and Lowy et al . showed no benefit with the perioperative use of octreotide in pancreatic resection. [32],[33] Meta-analyses and systematic reviews of octreotide use have also yielded conflicting results. [34],[35] A meta-analysis by Poon et al . of six prospective randomized trials on the prophylactic use of octreotide in pancreatic resections did not show any effect of octreotide in reducing the pancreatic fistula rate. [34] Despite this inconsistent data, many surgeons routinely use octreotide in patients undergoing pancreatic surgery. It has been recently suggested that selective administration of octreotide to patients deemed to have high-risk glands (ie, those with soft texture, small duct size, and ampullary, duodenal, cystic or islet-cell pathology) maybe associated with a decreased incidence of pancreatic fistula. [36] Extended pancreatic resections Pancreatic cancer is associated with a high frequency of lymph nodal metastases and extension beyond the pancreatic capsule into the retroperitoneum and surrounding structures and vessels. In an attempt to improve outcomes, surgeons have performed radical or extended pancreatectomies. This approach was pioneered by Fortner who performed en bloc resection of the pancreas and surrounding organs, along with a retroperitoneal lymph node dissection. [37] He had very good results at a time when mortality after PD was very high. Extended resections may include:
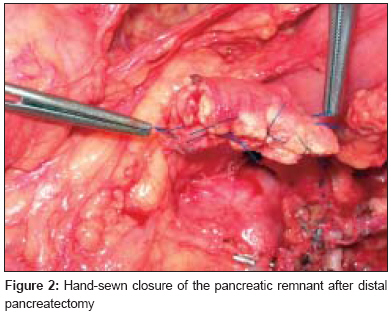
Total pancreatectomy (TP) The rationale for TP is that it allows for more extensive lymphadenectomy, obviates possible leak from the pancreatic anastomosis, and decreases the chances of a positive cut margin. Disadvantages of a TP include obligate diabetes mellitus, decreased immunity because of splenectomy, and loss of pancreatic exocrine function. Most studies of this procedure have reported worse survival after TP or no survival difference between TP and standard PD. [38],[39],[40] A TP for pancreatic head cancer should not be performed unless, serial positive cut margins on frozen section analysis lead to it, there is a soft pancreas with a very high chance of pancreatic leak, or there is a documented family history of multicentric disease. [41] Extended lymph node dissection (ELND) Up to 30% of patients with pancreatic cancer have retroperitoneal lymph node disease that would not be resected by a standard PD. [41] It was hypothesized that survival could be improved by using an ELND to help achieve node negativity and to dissect out lymph nodes that could potentially get infiltrated by malignant cells. ELND involves, in addition to removal of the pancreaticoduodenal nodes, removal of lymph nodes along the hepatic artery, superior mesenteric artery, celiac axis, and between the aorta and the inferior pancreaticoduodenal artery. Furthermore, the anterolateral aspect of the aorta and the inferior vena cava are also dissected. The earliest proponents of ELND were the Japanese, who demonstrated improved survival rates with extended surgery. The first RCT evaluating ELND vs standard lymphadenectomy (SL) was from Italy and by Pedrazzolli et al . [42] Subsequent RCTs comparing ELND vs SL during PD included a large trial with 280 patients by Yeo et al . at the Johns Hopkins University. [43],[44],[45] All these studies failed to show any survival benefit because of the addition of ELND to PD, although the Italian study did show a trend towards improved survival when ELND was performed in node-positive patients. [46] Meta-analyses of SL and ELND by Michalski et al . [47] further confirmed the findings of the above trials that ELND increased morbidity and offered no survival benefit over SL with PD and concluded that ELND should only be performed within controlled trials, if at all. Arterial/venous resections with reconstruction Vascular resections can be performed based on two rationales: firstly, to achieve negative resection margins in case of vessel invasion by the tumor or adhesion of the vessel to the tumor, making separation impossible; secondly, it can be performed as part of an extended pancreactectomy with ELND. [41] Vein resections include that of the portal vein (PV), superior mesenteric vein (SMV), or the SMV-PV confluence. Venous resections followed by graft reconstruction can be performed without increased morbidity and mortality and may be performed to achieve negative resection margins. [48],[49],[50] In contrast, arterial resections of the mesenteric, celiac, and hepatic arteries are rarely performed and are considered by most as contraindicated in PD due to the greatly increased morbidity and mortality. [48],[50],[51] Delayed gastric emptying (DGE) after PD According to definition, DGE is said to occur when the nasogastric (NG) tube is left in place for 10 or more days and there is also one of the following: emesis after removal of the NG tube, reinsertion of the NG tube, postoperative use of prokinetic agents after the tenth postoperative day, or failure to progress with diet. [52] A number of factors have been known to influence DGE, including removal of the duodenum, extent of lymph node dissection, vascular and neural damage, sepsis, presence of other complications, and type of reconstruction. Horstmann et al . showed that patients without other complications had a DGE rate of 1%, but in the presence of moderate and severe postoperative complications this rate climbed to 28% and 43%, respectively. [53] It is a common perception that an intact pylorus leads to a greater incidence of DGE after PPPD, but a comparison of the incidence of DGE after cW and PPPD suggests that both procedures are equivalent as far as the occurrence of DGE is concerned. [54] Alternate techniques have been used to reconstitute gastrointestinal continuity after PD with an aim to decrease the incidence of DGE; these techniques have included the use of an undivided Roux-en-Y loop for reconstruction and pyloric dilatation. [55],[56] However, there is level 1 evidence that antecolic reconstruction (as opposed to retrocolic duodenojejunostomy/gastrojejunostomy) is associated with a significantly reduced DGE rate. [57],[58] This is because an antecolic reconstruction avoids the possible torsion or angulation that may occur with a retrocolic anastomosis. There is also convincing evidence that DGE can be reduced by up to 37% with intravenous erythromycin. [52] Staplers in pancreaticoduodenectomy and total pancreatectomy (TP) As experience with pancreatic surgery evolves, further innovations and techniques are inevitable in order to decrease operating time and blood loss and increase safety, thus improving outcomes without compromising oncologic principles. For example, the use of stapling devices in pancreatic surgery has been widely reported in the literature by some authors, and the technique has been utilized for various steps during pancreatic surgery. [59],[60],[61],[62] Two technically challenging maneuvers during PD and TP involve the division of the proximal jejunal mesentery in the area of the duodenojejunal flexure and ligament of Treitz and dissection of the uncinate process from its posterior retroperitoneal attachments and the vascular branches from the superior mesenteric artery and portal vein. Both maneuvers can be safely performed with the aid of endovascular and endo-GIA linear stapler devices. [61],[62] Distal Pancreatectomy (DP) Management of pancreatic remnant after DP: stapled vs hand-sewn closure Complication rates after DP range between 22-37%, with a relatively high fistula rate of 5-6%. Pancreatic fistulae also remain a major cause of morbidity after distal pancreatectomy. A variety of procedures have been described to reduce the frequency of pancreatic fistula; these include hand-sewn closure [Figure - 2], stapled closure, combined stapled and suture closure, fibrin glue application, serosal jejunal patch, and prolamine injection. [63] While hand-sewn closure is a time-tested method, stapler application has gained increasing acceptance with the advent of laparoscopic DP. Knaebel et al . [64] published a meta-analysis that included six studies comparing stapler vs hand-sutured closure; they showed a nonsignificant combined odds ratio for occurrence of a pancreatic fistula of 0.66 (95% CI: 0.35 to 1.26; P = 0.21) in favor of stapler closure. However, more recently, Kleeff et al . [65] published a large, single-institution series of 302 DPs, wherein it was observed that stapler closure was associated with a higher pancreatic fistula rate. It thus appears that the jury is still out and surgeons must follow their own individual experience when dealing with the pancreatic remnant after DP. In hand-sewn closure, the guiding principle should be to make an effort to identify the pancreatic duct, close it with fine sutures, and then close the entire stump with sutures. The impact of splenectomy on outcomes after DP and TP Conventionally, the spleen is removed as part of a DP. This has been done with the rationale that splenic preservation might compromise oncologic principles. However, splenectomy is associated with septic postoperative complications, including the risk of overwhelming postsplenectomy sepsis, although the risk is low. To prevent these complications, spleen-preserving DP has been advocated by a number of surgeons. [66],[67] Schwarz et al . [68] studied a group of 326 patients with adenocarcinoma of the pancreas who underwent DP and TP, with or without splenectomy. They concluded that splenectomy has no significant impact on postoperative recovery, but it negatively influenced long-term survival independent of disease-related factors. They advocated the avoidance of splenectomy unless the splenic capsule was involved by, or adherent to, the tumor; the splenic hilum was infiltrated by the tumor; or nodal clearance mandated a splenectomy. On the other hand, Sledzianowski et al . [69] failed to prove the importance of splenic conservation in DP. Mirza et al . concluded that spleen preservation did not influence outcomes after DP and TP and that in order to fully assess the effect of splenectomy on survival after pancreatectomy, larger series of patients would be required. [70] Segmental pancreatectomy [Figure - 3] Small and circumscribed benign and low-grade malignant tumors of the body, neck, and tail of the pancreas have been traditionally removed by PD or DP. However, these procedures, despite low mortality, result in a significant loss of normal pancreatic parenchyma, leading to endocrine and exocrine pancreatic dysfunction and, in addition, are associated with anastomotic complications and problems related to the alteration of the biliodigestive passages and splenectomy. [68],[71] To avoid these, many surgeons perform enucleation of these small tumors. However, despite apparently avoiding the pancreatic duct, complications like pancreatic fistula, acute pancreatitis, and pseudocysts are common. [72] A segmental pancreatectomy, alternatively known as middle segmental pancreatic resection, median pancreatectomy, central pancreatectomy, or intermediate resection, involves removal of the lesion with adequate margins on either side, the procedure being guided by intraoperative frozen-section analysis. This preserves the normal pancreatic parenchyma, the bile duct, duodenum, and spleen. The cephalic stump is then sutured and the distal stump anastomosed to a Roux-en-Y jejunal loop. [73] Despite a higher incidence of pancreatic fistula, and the subsequent increased morbidity and hospital stay, segmental pancreatectomy is a safe and adequate operation for selected patients with centrally placed benign or low-malignant-potential lesions of the pancreas. [71],[74] Laparoscopic pancreatic resections Gagner [75] has been credited with performing the first laparoscopic Whipple′s operation. Since then, a few papers have appeared from different centers describing their experience with this procedure. [76],[77] These papers suggest that it is technically possible to perform such a demanding operation laparoscopically. However, the morbidity of the Whipple′s operation is not related to the length of the abdominal incision but to the extensive nature of the actual intra-abdominal surgery. At present there is no worthwhile evidence to suggest that laparoscopic Whipple′s is better than open surgery. This procedure may be performed by highly trained surgeons, in high-volume dedicated centers, and that too within the context of good clinical trials. Laparoscopic surgery is ideally suited for those procedures which otherwise require a large abdominal incision to access and remove a small organ or tumor. Therefore, compared to PD, the scenario with laparoscopic DP is somewhat different. Increasing evidence has documented benefits of laparoscopy over open surgery in the management of small benign tumors of the pancreatic body and tail, eg, cystadenomas, insulinomas, gastrinomas, etc. [78] Laparoscopic DP or enucleation of such tumors is a safe procedure in experienced hands, with comparable morbidity and mortality. [78],[79] In summary, with regard to laparoscopic PD, feasibility should not be confused with benefit. [80] On the other hand, laparoscopic DP may well provide a distinct advantage over open surgery in the near future in highly selected small tumors of the body and tail. However, training surgeons for these complex procedures has to be undertaken in high-volume centers of pancreatic surgery. References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08021t1.jpg] [cr08021f2.jpg] [cr08021f1.jpg] [cr08021t2.jpg] [cr08021t3.jpg] [cr08021f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}