 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
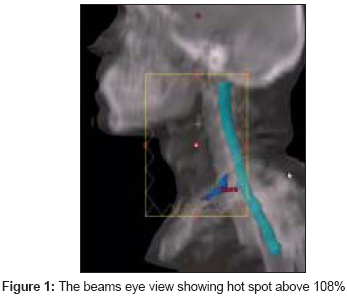
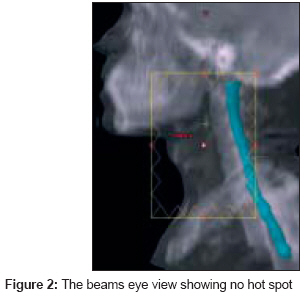
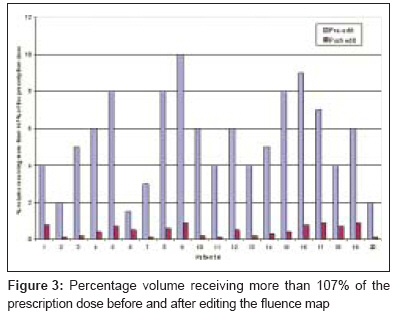
Journal of Cancer Research and Therapeutics, Vol. 4, No. 2, April-June, 2008, pp. 84-87 Brief Communication Does the fluence map editing in electronic tissue compensator improve dose homogeneity in bilateral field plan of head and neck patients? Kinhikar RajeshA Department of Medical Physics, Tata Memorial Hospital, Parel, Mumbai Code Number: cr08022 Abstract The purpose of this study was to evaluate the effect of fluence map editing in electronic tissue compensator (ETC) on the dose homogeneity for head and neck cancer patients. Treatment planning using 6-MV X-rays and bilateral field arrangement employing ETC was carried out on the computed tomography (CT) datasets of 20 patients with head and neck cancer. All the patients were planned in Varian Eclipse three-dimensional treatment planning system (3DTPS) with dynamic multileaf collimator (DMLC). The treatment plans, with and without fluence editing, was compared and the effect of pre-editing and post-editing the fluence maps in the treatment field was evaluated. The skin dose was measured with thermoluminescent dosimeters (TLDs) and was compared with the skin dose estimated by TPS. The mean percentage volume of the tissue receiving at least 107% of the prescription dose was 5.4 (range 1.5-10; SD 2.4). Post-editing fluence map showed that the mean percentage volume of the tissue receiving at least 107% of the prescription dose was 0.47 (range 0.1-0.9; SD 0.3). The mean skin dose measured with TLD was found to be 74% (range 71-80%) of the prescribed dose while the TPS showed the mean skin dose as 85% (range 80-90%). The TPS overestimated the skin dose by 11%. Fluence map editing thus proved to be a potential tool for improving dose homogeneity in head and neck cancer patients planned with ETC, thus reducing the hot spots in the treatment region as well. The treatment with ETC is feasible with DMLC and does not take any additional time for setup or delivery. The method used to edit the fluence maps is simple and time efficient. Manual control over a plan is essential to create the best treatment plan possible. Keywords: Electronic tissue compensator, fluence editing and skin dose, head and neck cancer Head and neck cancers constitute a significant proportion of the patients receiving radiotherapy (RT). Aggressive multimodality treatment has improved the local control and overall survival in head and neck cancers over the last few decades. The majority of the patients treated with conventional techniques of radiation receive bilateral fields, with or without a low anterior neck field. The anatomy of the head and neck region is irregular and the tissue separation varies considerably in different parts of the field. This makes the choice of correct prescription depth difficult and results in dose inhomogeneity within the treated volume. The hot spots (+7%) and cold spots (−5%) are analyzed from the dose-volume histogram (DVH). [1] There is a risk of overdosage in the anterior part of the neck where the tissue separation is less, resulting in both acute side effects (radiation dermatitis) and a long-term risk of late effects in the skin and subcutaneous tissue (including skin discoloration, subcutaneous edema, and fibrosis). With more and more patients treated to near tolerance doses (≥70 Gy), and an increasing number of survivors, the issue of normal-tissue complications is becoming more and more important. Sophisticated delivery techniques like intensity-modulated radiotherapy (IMRT) can address the problem of contour irregularity to a certain extent. However, in a busy radiation oncology setup, multiple-field treatment is not practical for all patients with head and neck cancer. A simpler solution to this problem is the use of tissue compensators (TC). However, this requires a considerable investment of time, both in the mould room as well as during treatment where accessories need to be attached and removed physically. Electronic tissue compensation (ETC) provides a more accurate method of compensation, both for external contour irregularities and tissue inhomogeneity; it is an automated process without the need for physical intervention, thus resulting in saving of both machine time and physical effort. Missing tissue compensation is an important issue in radiotherapy (RT) and various methods are employed to achieve dose homogeneity. One of the modality with which dose homogeneity could be achieved is the use of a multileaf collimator (MLC). MLCs are widely used for tissue compensation. [2],[3],[4],[5],[6],[7] They create variable intensities to deliver a homogeneous dose to the entire treatment field, resulting in unwanted hot spots at critical locations though inside planning target volume (PTV). If the volume of this hot spot is considerable, then it could create normal-tissue complications. Fluence editing is one way to minimize the dose inhomogeneity inside the PTV and thus reduce the volume of the hot spot. While editing the fluence the dose may at times be spilled over at other places. The purpose of this study was to effectively reduce hot spots, without any dose spillage elsewhere, to achieve the desirable dose homogeneity. The skin dose was also measured during treatment since it would not be appropriate to estimate skin dose from the treatment planning system. Materials and Methods As a part of an evaluation process for the future routine implementation of ETC in bilateral neck fields we conducted a study on a select group of patients. We chose patients with early-stage or small-volume locally advanced diseases that were planned for curative-intent radiotherapy. Those with large fields spanning a wide area of the face and neck (and therefore likely to benefit most from tissue compensation) were preferred. Twenty patients were selected for this study. All the patients underwent computed tomography (CT) scans in the supine position (Somatom Emotion, Siemens Oncology Systems, Germany) with 3-mm slice thickness. For immobilization, thermoplastic masks were used for each patient. The images were then exported to the Eclipse (Varian Medical Systems, Milpitas, CA) three-dimensional treatment planning system (3DTPS) via by local area network . After the organ delineation by the clinician, the beam parameters were determined. Two 6-MV, lateral opposed, coplanar, isocentric beams were placed. The average field size for all the patients was 10 x 13 cm. The tissue compensator was attached to both the beams and further converted to the electronic tissue compensator to create the desired fluence. A dose of 2 Gy was prescribed at the midplane. The calculation grid of 2.5 x 2.5 mm was selected for dose computation. The dose distribution was obtained and the fluence map was generated with the ETC. The dose distribution was thoroughly checked in all the axial, sagittal, and frontal slices. Further, no volume was acceptable above 107%. The volume of the hot spot was checked from the beams eye view (BEV) as well. The fluence map was edited if the volume of the hot spot exceeded the acceptable limit and the location of the hot spot was at critical location. Because editing fluence maps is done from the BEV, any edit affects all isodoses in that beam path. The plan was recalculated after the fluence of the first beam had been edited, and then the process was repeated with each successive beam edit. Thus the fluence map was edited in both the beams to reduce the hot spot effectively. The effect of fluence editing was again assessed and the plans were compared. The treatment plans with and without fluence editing were compared and the effect of pre-editing and post-editing the fluence maps in the treatment field was evaluated. In vivo dosimetry For measurements using TLD, about 40 mg of the freshly annealed TLD-100 powder was packed in a square polyethylene pouch (1 x 1 cm). This TL pouch was directly placed on the skin at the entrance of each field. The TL output of about 10 mg powders was recorded using the Rexon TLD reader and in this way four readings were obtained from each TL pouch. The mean value of the net TL output per unit weight (nC/mg) of these four readings was used for calculation. The uncertainty in TLD-100 powder measurements was ±2%. A constant time gap of 24 h was maintained between irradiation and read-out. A dose-response curve for the TLD-100 powder was generated in 60 Co gamma ray beam (Equinox 80, MDS Nordion, Canada) and was found to be linear in the range of 0.5-4.0 Gy. One packet was not irradiated to determine the background signal. The skin dose measured with TLD was then compared with the calculated skin dose by TPS. Results [Figure - 1] shows the location of hot spot for the ETC plan for one patient. The dose cloud shown in this figure is the volume of tissue receiving at least 107% of the prescription dose. From this figure it is clearly seen that though the volume of the high-dose region is small, the location is critical. In a few patients, it was seen that this volume appeared near the skin, thus making it essential to asses the skin dose. The mean percentage volume of the tissue receiving at least 107% of the prescription dose was 5.4 (range 1.5-10; SD 2.4). This volume was effectively reduced to the minimal (negligible) volume after editing the fluence map. Thus, post-editing of the fluence map showed that the mean percentage volume of the tissue receiving at least 107% of the prescription dose was 0.47 (range 0.1-0.9; SD 0.3). [Figure - 2] shows the edited fluence map which shows no hot spot. Editing the fluence maps does not necessarily increase the monitor units or the treatment time. [Figure - 3] shows percentage volume receiving more than 107% of the prescription dose before and after editing the fluence map for 20 patients. The mean skin dose measured with TLD was found to be 74% (range 71-80%) of the prescribed dose while the TPS showed the mean skin dose to be 85% (range 80-90%). The TPS overestimated the skin dose by 11%. Discussion This paper reports the clinical application of ETC to achieve dose homogeneity in 20 head and neck cancer patients. An ETC is a field modifier implemented by means of a DMLC that replaces a mechanical compensator. Electronic compensation does not require the high overheads in production as is in the case with mechanical compensators, and multi-beam treatments are much faster because there is no need to install a different physical compensator before each treatment beam. ECs are added to a plan in Eclipse by first inserting a standard plane compensator in the plan and then converting it into an EC. The compensation method used is plane compensation. The conversion of a standard plane compensator into an electronic compensator creates an optimal fluence, according to the calculation parameters. The calculation is done for each field by scanning all points within the field on the selected plane. The compensator calculation begins at the user-defined distance from the edge of the patient tangential border. The optimal fluences are then converted into actual fluences and a pattern is generated by the leaf motion calculator (LMC). When the plan and the DMLC motions are completed, the DMLC leaf motion file can be exported to the treatment unit. The uniform dose distribution is computed using the dose back-projection method, in which the optimal fluences are defined. The dose back-projection is done in the diverging field coordinate system. However, there are some limitations with ETC. Electronic compensation is available for open coplanar photon fields. One cannot add an electronic compensator to an electron field, and electronic compensators cannot be used for arc fields. Moreover, one field may not contain both a physical plane compensator and an EC. Tissue compensation is used to correct the dose inhomogeneity resulting from an irregular patient surface. Improved dose homogeneity can be obtained using ETC, in which the fluence distribution required to produce an isodose surface perpendicular to the central axis at a specified depth is calculated and delivered using an MLC. Ray tracing and determining the amount of missing tissue along each ray line calculates the fluence distribution. TLDs were found to be useful dosimeters for measuring the skin dose due to their minimal dependence on dose rate, temperature, and energy in the therapeutic range and their wide applicable dose range. Conclusion Fluence map editing proved to be a potential tool for improving dose homogeneity in head and neck cancer patients planned with ETC, thus reducing the hot spots in the treatment region as well. Treatment with ETC is feasible with DMLC and does not take any additional time for setup or delivery. The TPS overestimated the skin dose by 11%. The method used to edit the fluence maps is simple and time efficient. Manual control over a plan is essential to create the best treatment plan possible.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08022f3.jpg] [cr08022f1.jpg] [cr08022f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}