 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
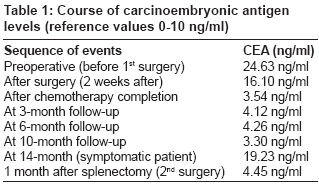
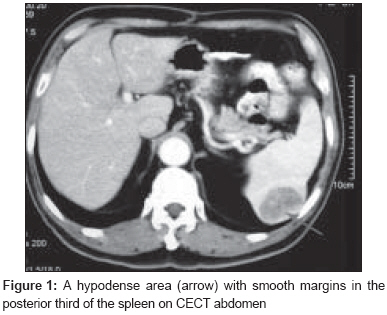
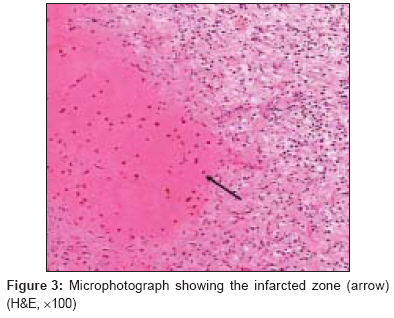
Journal of Cancer Research and Therapeutics, Vol. 4, No. 2, April-June, 2008, pp. 99-101 Case Report Splenic infarct as a diagnostic pitfall in radiology Joshi SanjeevC, Pant Ishita, Shukla AdityaN, Anshari MA Department of Oncology, Palliative Care Unit, Radiology Advanced Medical and Dental Institute, Universiti Sains Malaysia, Pinang Code Number: cr08028 Abstract Follow-up of colorectal carcinoma after therapy is based on symptoms, tumor markers, and imaging studies. Clinicians sometimes face diagnostic dilemmas because of unusual presentations on the imaging modalities coupled with rising serum markers. We report a case of colorectal carcinoma that presented with gastrointestinal symptoms 14 months after completion of treatment. Investigations showed rise in carcinoembryonic antigen (CEA). Suspecting disease recurrence, complete radioimaging workup was performed; the only abnormality detected was a smooth, hypodense area in the posterior third of the spleen on contrast-enhanced computed tomography abdomen. In view of the previous diagnosis of carcinoma colon, the symptoms reported by the patient, the elevated CEA, and the atypical CECT appearance, a diagnosis of splenic metastasis was made. The patient was subjected to splenectomy as a curative treatment. However, the histopathological report revealed it to be a splenic infarct. The present case reemphasizes the limitations of radiological studies in the follow-up of carcinoma colon.Keywords: Contrast-enhanced computed tomography, colon cancer, metastasis, splenic infarct Follow-up for carcinoma patients after completion of initial therapy relies on symptoms, serological markers, and radiological imaging studies. However, each modality has its own limitations and presents clinicians with diagnostic dilemmas. We report a case of a 76-year-old man suffering from adenocarcinoma of the colon who presented with such diagnostic dilemma while under follow-up. Case Report A 76-year-old man underwent exploratory laparotomy and extended right hemicolectomy and diagnosed with invasive adenocarcinoma of right hepatic flexure colon; staged as Duke′s B2 (Astlar-Coller modified Duke′s classification). Four of nine lymph nodes were positive for metastasis and there was perinodal invasion. The patient had an elevated CEA level (24.63 ng/ml; reference range 0-10 ng/ml). All other investigations were normal. The patient was advised adjuvant chemotherapy. He received eight cycles of chemotherapy. Each chemotherapy cycle comprised of oral capecitabine 1.25 gm/m 2 twice daily for 14 days followed by 1 week rest. Following chemotherapy, the blood carcinoembryonic antigen (CEA) level decreased to 3.54 ng/ml. The patient then had quarterly follow-up with serological studies. He remained symptom free, and CEA levels were within normal limit till the fourteenth month postoperatively [Table - 1]. However, left abdominal pain for 1 month and raised CEA level at the fourteenth postoperative month necessitated complete metastatic workup, including X-ray chest, CECT abdomen and thorax, plain CT head, and bone scan. Computed tomography (CECT scan) [Figure - 1] of the thorax and abdomen revealed a rounded hypodense mass with smooth margins in the posterior one-third of the spleen; there was no dissemination of disease in the liver, peritoneum, and para-aortic lymph nodes. Based on the rising CEA levels and the radiological CECT appearance suggestive of metastatic deposits it was provisionally reported as splenic metastases. The patient was subjected to a complete preoperative workup and hematological examinations which were normal. In view of the patient′s favorable general health and the absence of any other site of metastasis, he was subjected to exploratory laparotomy and a splenectomy was done to prolong survival and to confirm the diagnosis histologically. However, the histopathology showed a splenic infarct and not metastasis [Figure - 2] and [Figure - 3]. Postoperatively, CEA levels started dropping and reverted to the normal range within 4 weeks. To the best of our knowledge, this is the first case report of a colorectal carcinoma where the typical features of metastasis and the rise in CEA led to the diagnosis of metastases in the spleen, whereas the lesion was, in fact, a splenic infarct. Discussion Our patient was followed up at 3-monthly intervals with serum CEA monitoring as per the ASCO (American Society of Clinical Oncology) recommendations. [1] The same guidelines also recommend that an elevated CEA warrants further evaluation for metastatic disease and CEA results should not be interpreted as absolute evidence for the presence of malignant disease but should be used in conjunction with other investigations. As such, our patient was followed up with radioimaging investigations, which revealed a hypodense lesion suggestive of solitary metastases in the posterior third of the spleen. CECT is the imaging modality of choice for conditions affecting the spleen. [2] The majority of solitary splenic lesions identified with CECT are of primary splenic origin, eg, hemangioma, lymphoma, hematoma, abscess, and infarction. However, in patients with a past history of malignant disease, especially if accompanied by a rising serum marker, such a lesion must be considered as malignant unless proven otherwise. It is important to confirm the diagnosis by means of percutaneous fine needle aspiration biopsy or by histopathology following splenectomy. [3],[4] In the absence of other sites of neoplastic disease, splenectomy seems to be the preferred therapy because it can be performed with low morbidity and also favors long-term survival. [5] The spleen is the tenth most common site for metastases, with splenic metastases reported in 7.1% of 7246 patients with various types of malignant tumors. [6] Solitary splenic metastasis in colon carcinoma is rare, with fewer than 30 cases reported in literature; [4] it accounts for about 11% of all solitary splenic metastasis. Our patient presented with left abdominal pain for 1 month and a rise in serum CEA. The available literature reports that solitary splenic metastases are asymptomatic or else present with nonspecific symptoms like abdominal pain; even the rise in serum markers is not a consistent feature. [3] A few patients with isolated splenic metastasis become symptomatic because of the presence of an associated splenic abscess or the spontaneous rupture of the spleen. [7] On radioimaging modalities like ultrasonogram, CT, and MRI, splenic metastases usually appear as multiple discrete nodules. CECT images typically appear as rounded hypodense nodules. Sometimes these hypodense areas may demonstrate cystic changes and/or calcification. [8] Splenic infarct is an uncommon form of pathology. It is the result of arterial or venous compromise and is associated with a heterogeneous group of diseases including thromboembolic disorders, atrial fibrillation, myocardial infarction, hematological malignant diseases, sepsis, underlying thrombophilia, and coagulation disorders. The splenic infarct classically appears as a sharply demarcated wedge-shaped lesion, with the broad base towards the capsule. The hemorrhagic component may be visible as high-attenuation areas on CECT. [8] However, some cases of chronic subcapsular hematoma of the spleen and infarction of spleen may show a pseudocystic image. [9],[10] Although, the time between cessation of chemotherapy and diagnosis of splenic infarct is about 8 months in our case, the institution of chemotherapy and the mode of administration of chemotherapy probably contributed to a procoagulant state as has been suggested by some researchers. [11] The rise in CEA levels and the decline subsequent to splenectomy, without any adjuvant therapy, may be due to the presence of inflammation in the infarcted spleen. Elevated CEA levels are reported in some nonneoplastic conditions which have inflammation as an integral component, eg, ulcerative colitis, pancreatitis, cirrhosis, smoking, infections, and inflammatory bowel disease. [12] Positron emission tomography (PET)/computed tomography (CT) has emerged as a significant molecular imaging technique. PET/CT has a unique ability to detect and quantify the physiological and receptor processes that is not possible by other imaging technique; [13] it can therefore be very sensitive in identifying malignant conditions. During follow-up, the use of PET scanning can easily differentiate between malignant conditions and splenic infarct. Unfortunately, none of the different societies of clinical oncology strictly recommend PET scan in the follow-up protocol of colonic cancer. We emphasize that when there is clinical suspicion of metastasis but imaging is unclear and also, especially, in the setting of an unusual site of metastases, planning of PET/CT scan is mandatory. Conclusion As currently accepted serological and radioimaging studies lack sufficient specificity and sensitivity, such diagnostic dilemmas may be faced by clinicians. Splenic infarct should also be considered in the differential diagnoses in patients with a solitary splenic lesion suggestive of malignancy. Radiologically, whenever a diagnosis of metastasis is considered following CT scan, further investigations like PET/CT image fusion can be informative and diagnostic. The diagnosis may be further confirmed by splenectomy and pathological techniques depending upon the patient′s condition. There exists a need for the wider availability of better radiological imaging techniques like PET/CT fusion imaging which may be of help in such scenarios; unfortunately, such facilities are not available in our setting.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08028f3.jpg] [cr08028f2.jpg] [cr08028f1.jpg] [cr08028t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}