 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
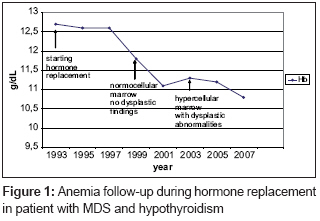
Journal of Cancer Research and Therapeutics, Vol. 4, No. 2, April-June, 2008, pp. 102-103 Letter To Editor The relationship between the thyroid hormone (or its lack) and dysplastic hematopoiesis Magalhaes SMM, Pinheiro DA, Souza MD, Pinheiro RF Hospital Universitário Walter Cantídio - Division of Hematology - Federal University of Ceará Code Number: cr08029 Related articles: cr07011 Sir, We read with interest the report of the clinical study by Akoum et al . on myelodysplastic syndrome and hyperthyroidism. [1] Erythropoiesis is influenced directly or indirectly by many hormones other than erythropoietin. Both hyperthyroidism and hypothyroidism are associated with hematological abnormalities. Untreated thyroid insufficiency can be insidious or subclinical. In these cases anemia is usually mild, may be masked by a decrease in plasma volume, and is probably related to tissue oxygen consumption and arrested red cell production. Iron kinetic abnormalities typical of the anemia of chronic disease have also been documented. [2],[3] Myelodysplastic syndromes (MDS) are characterized by progressive marrow failure and a tendency for evolution to acute leukemia. Dysplastic hematopoiesis is the cornerstone of diagnosis. In addition, cytogenetic analysis may provide diagnostic and prognostic information. However, dysplastic hematopoiesis is a frequent finding in patients with cobalamin/folate deficiency, HIV infection, kidney and liver failure, and in autoimmune and metabolic diseases, including thyroid dysfunctions. Especially in cases with no excess of blast or clonal cytogenetic abnormality, the diagnosis of MDS requires an extensive exclusion of reversible nonclonal disorders. [4] In an unselected series of 138 adult patients with MDS, primary hypothyroidism (TSH> 10 mU/l; normal range 0.25-4 mU/l) was present on diagnosis in six cases. Anemia was present in all patients. Vitamin B 12 and folate deficiencies were systematically excluded. Cytogenetic analysis was performed in five patients and no clonal abnormalities were detected. The median follow-up period was 7 years (range 1-13 years). Continuous hormone replacement resulted in normalization of TSH; the hemoglobin level rose in all cases but one [Figure - 1], although none reached the normal range. Interestingly, the bone marrow analysis performed after at least 6 months of adequate treatment revealed increase in cellularity, more pronounced dysplastic abnormalities involving more hematopoietic lineages and, in two cases, a thickness of reticulin that has not previously been documented. Anemia is common in hypothyroidism and is considered to be an adjustment to a decreased basal metabolism. It is characterized by reticulopenia, erythroid hypoplasia, and a decreased level of endogenous erythropoietin. [5] It is possible that the thyroid insufficiency, and the consequent arrested hematopoiesis, hinder or prevent the full-blown bone marrow dysplastic features of MDS from manifesting. The replacement treatment, by correcting the hypoproliferative status, makes the dysplastic abnormalities more conspicuous and concomitant MDS more evident, the possible reason for partial or no hemoglobin response. Continued attention to thyroid function therefore seems essential in the diagnosis and management of MDS. References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08029f1.jpg] |
| |||||||||

{kind=link}