 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
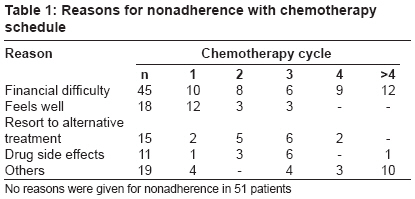
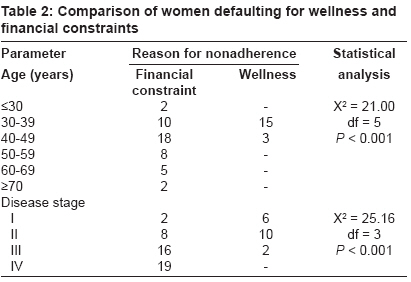
Journal of Cancer Research and Therapeutics, Vol. 4, No. 3, July-September, 2008, pp. 107-110 Original Article Paradox of wellness and nonadherence among Nigerian women on breast cancer chemotherapy Adisa AdewaleOluseye, Lawal OladejoOlukayode, Adesunkanmi Abdul RasheedKayode Department of Surgery, Obafemi Awolowo University and Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife Code Number: cr08033 Abstract Context: Intentional nonadherence among cancer patients is rare and may occur only when the benefits of treatment are not obvious to the patient.Aims: To highlight a group of women on chemotherapy for breast cancer who defaulted from their medications because they were improving. Settings and Design: A study was carried out of the reasons for nonadherence to medications among women receiving chemotherapy for breast cancer at a Nigerian teaching hospital between January 1993 and December 2002. Materials and Methods: A retrospective review of patients' records was done. Results: Of the 188 women who received chemotherapy during the study period, 152 (80.9%) defaulted from treatment at one point or another. The reasons for nonadherence were available in 101 patients. Among these, 18 (18.0%) reported nonadherence because they felt better after commencing chemotherapy. They were aged 31-50 years (Mean = 35.6 (SD3.2)). Six (33.3%) of them presented in AJCC Stage I, and 10 (55.6%) in stage II. Age and disease stage at presentation were found to have significant influence on their reason for nonadherence. Of the nine women on neo-adjuvant chemotherapy, six (66.7%) had complete response but defaulted and five (55.6%) re-presented within a year with metastatic disease. Three of the patients receiving systemic post-surgery chemotherapy presented within a year with local recurrence. Most of the other patients were subsequently lost to follow-up. Conclusions: Nonadherence due to wellness among breast cancer patients is associated with poor outcome. We propose a detailed prospective study to establish factors that may influence such behavior. Keywords: Breast cancer, chemotherapy, nonadherence, wellness Introduction Adherence in healthcare is defined as the extent to which a person′s behavior (taking medications, following a diet and or executing lifestyle changes) corresponds to agreed recommendations from a healthcare provider. The term ′adherence′ is now preferred to the authority laden word "compliance" by many authors. [1],[2] The psychological basis of nonadherence among patients with different medical conditions has not been fully understood. However, nonadherence to treatment has been noted to account for poor clinical outcome, worsening of diseases, death and increased cost of healthcare in many patients. [3],[4] Realization of this has led to various measures to monitor and improve treatment adherence among many patients with different diseases. [5],[6],[7],[8] Many studies have reported intentional and non-intentional nonadherence with drugs among patients. In the USA, one in three adults reported nonadherence with medication prescription. [3],[9] Generally, the incidence of adherence is higher in acute conditions while nonadherence is higher in chronic conditions especially those in which healthcare recommendations require prolonged medication or drastic lifestyle changes. [10],[11],[12] Despite the seriousness often associated with the treatment of cancers, some studies have also affirmed that nonadherence exists among cancer patients. The reasons for nonadherence however differ among these patients. Unintentional nonadherence may however be commoner among cancer patients and drug side-effects, forgetfulness, financial constraint and availability of insurance, inadequate supervision and history of mental illness among others are factors that may lead to drug noncompliance. [13],[14] A previous study of breast cancer patients found that 1 in 6 reported intentional nonadherence. [15] Elwyn et al . also noted that intentional nonadherence may occur when the benefits of treatment are not obvious. [16] However in a recent review of chemotherapy adherence among breast cancer patients in our hospital, 18 patients reported intentionally choosing not to take their medications because they had seen the improvement of previous medications. This paradox of wellness and nonadherence has not been previously reported among breast cancer patients. We present here the clinical findings among this group of women as well as a review of the literature. Materials and Methods The treatment records of all patients who had chemotherapy for breast cancer at a single centre in South West Nigeria over a ten-year period from January 1993 to December 2002 were reviewed. Patients′ adherence to medications and reasons for nonadherence, treatment outcome and patients′ outcome were also studied. Nonadherence was defined as omission of two consecutive doses of injectable chemotherapy or a self report of taking 90% or less of the oral chemotherapeutic drugs including cyclophosphamide, capecitabine and prednisolone at any of the oncology clinic visits. Patients who had drug omission due to inadequate hematological profile or poor clinical condition were not categorized as non-adherers. Data of the patients who reported nonadherence due to a feeling of improvement were grouped together and subjected to descriptive analyses using simple frequency and chi-square test. Critical level of statistical significance was set at 0.05 and statistical tests were one tailed. Results Within the study period, 285 histologically proven cases of breast cancer were managed. Of these, only 225 records were complete and suitable for analysis. One hundred and eighty-eight patients had chemotherapy for breast cancer and 152 of these (80.9%) had records of nonadherence at one point or another. The reasons for nonadherence were recorded in only 101 patients and are as shown in [Table - 1]. Among the 101 patients in whom reasons for nonadherence were obtained, 18 (18.0%) reported nonadherence with chemotherapy because they felt better after commencing chemotherapy. They were aged 31-50 years with a mean age of 35.6 (SD3.2). Twelve (66.6%) of the patients were less than 35 years of age. Using the American Joint Committee on Cancer (AJCC) staging system, six (33.3%) patients presented in Stage I, 10 (55.6%) in stage II, and the remaining two (11.1%) had stage III disease at initial presentation [Table - 2]. Histopathology of trucut biopsy and/or mastectomy specimen confirmed invasive ductal carcinoma in 16 (88.9%) of the patients while the other two (11.1%) had malignancy confirmed by fine needle aspiration cytology. Nine (50.0%) of these women were on neo-adjuvant chemotherapy while the others were receiving systemic chemotherapy after initial surgery. A combination of Cyclophosphamide, Methotrexate and 5-fluorouracil (CMF), was used in 13 (72.2%), three (16.6%) had a combination of Cyclophosphamide, Adriamycin and 5-fluorouracil (CAF) while one patient had CAF with Methotrexate. Of the nine women on neo-adjuvant chemotherapy, six (66.7%) had complete response to chemotherapy with documented non-palpable tumors in five women after the first two cycles of chemotherapy. In the final analysis, five of the nine women on neo-adjuvant chemotherapy re-presented within 6-12 months with metastatic disease while the remaining four were lost to follow-up. Among those receiving systemic chemotherapy post-surgery, three re-presented within a year with local recurrence at the site of previous surgery, two re-presented within a year in good condition and were recommenced on adjuvant chemotherapy but both defaulted again and were subsequently lost to follow-up, one patient re-presented after two years with hepatomegaly and ascites. The remaining three were not seen again after the initial default from treatment. Discussion Intentional nonadherence in breast cancer patients is an unexpected finding due to the usual seriousness attached to the management of the disease. The group of patients highlighted in this study reported intentional nonadherence for reasons of feeling well. The main reasons for not continuing medication among these patients was because the breast masses had disappeared or reduced considerably with chemotherapy or has been removed surgically. This is in spite of earlier education on the possible consequences of nonadherence to chemotherapy. All 18 patients were young adults with a mean age of 35.6 years. Two of every three are aged between 30 and 34 years. This is a much younger age group compared to the general population of patients with breast cancer in our hospital with a mean age of 48.2 years. [17] Younger age was found to have a statistically significant relationship to nonadherence due to wellness in this study. Some studies had earlier shown that adherence to medications is not usually related to socio-demographic factors such as age, sex, level of education or race.[15],[18],[19] However, a previous study of nonadherence to Tamoxifen among women with breast cancer identified younger age as one of the factors associated with lower rates of adherence.[20] In African communities, breast cancers frequently occur in younger women and the observation of a higher rate of adherence may be related to the younger age of presentation in our environment. At a younger age, most women in our setting are more concerned with keeping their breasts and the fear of possible mastectomy may contribute significantly to the rate of nonadherence. Unfortunately, late disease stage at initial presentation coupled with nonadherence to medication and the non-availability of radiotherapy in our setting usually limit the practice of breast conserving surgeries among our women who may otherwise be happier with modalities of treatment that allow them to keep their breasts. Unlike the population of patients reporting nonadherence for financial constraints or other reasons who presented at late stages of the disease, those reporting nonadherence due to wellness had earlier presented in early operable stages. Sixteen of 18 presented in AJCC stages I and II while the remaining two presented in AJCC stage III. This is in contrast to the general population of breast cancer patients in our setting in whom we have observed that up to 75% may have stages III and IV diseases at initial presentation. [17] One half of them were on neo-adjuvant chemotherapy with significant effects including complete regression in five patients. The other half stopped their drugs within the first two cycles of systemic chemotherapy after mastectomy. This attitude may be related to poor understanding of the course and management of the disease among these patients. On the other hand, we feel that these women give an excuse of feeling better to stop their treatment even when they understand that the disease is not yet cured. Clinicians in our setting should hence be aware of such undue claims of "feeling well" as this may herald the beginning of nonadherence to further treatment. Many studies have identified lack of adequate information about the advantages and disadvantages of a treatment as a factor associated with nonadherence. [13],[16] In other studies, patients′ knowledge of their disease or its therapy were found not to be related to their adherence to their treatment. [21],[22] In our study, patients of high socio-economic status were also among the non-adherers. The strong belief in traditional healing practices where patients are told the tumor will disappear after certain things are done might have influenced some of the patients to default from further orthodox care especially with complete tumor response to chemotherapy. Previous studies had noted that intentional nonadherence may occur when the benefits of treatment are not obvious. [16],[23] However, the group of patients we highlighted in this study defaulted from further treatment because they saw the benefit of the initial treatment and felt well thereafter. Psychological adaptation of patients has also been associated with intentional nonadherence. The hypothesis of locus of control, in which an individual who believes he or she has a great control over the outcome of an illness is observed to adhere more strictly to medications was earlier described by Partridge and colleagues. [24] Using this model among breast cancer patients, Atkins and Fallowfield found a high incidence of intentional nonadherence among patients who viewed themselves as having less influence over their own health. [15] Avres and colleagues also showed that mood and adjustment to cancer influenced adherence to chemotherapy among breast cancer patients. A high score of fighting spirit was associated with greater adherence to chemotherapy. [25] Two recent studies evaluating the use of tamoxifen and anastrazole among breast cancer patients reported adherence rates dropping from 88% in the first year to 60% in the third year of continuous medication. [26],[27] One study identified drug side effects and financial constraints as the main reasons why patients may not adhere to medications. [26] In our study, the level of nonadherence is relatively high, with close to half of the patients complaining of financial constraint. In most developing countries without a functional health insurance system, the financial burden of chemotherapeutic agents may be beyond the reach of the poor majority. Similarly, resort to alternative traditional and or spiritual cure was common among our patients. This stems from a firm belief in the supernatural methods of healing especially in instances where orthodox medicine does not offer immediate cure. It is also noteworthy that drug side effects contributed significantly to the nonadherence among our patients similar to findings in western countries. Ameliorating these side effects when they occur will hence be important in improving the rate of nonadherence among our patients. This retrospective study may however have some limitations. Assessment of nonadherence has been by self-reporting among the patients and the attending physicians were expected to have properly documented the reports. Also adequacy of record keeping has not been ascertained. Therefore, a prospective study to evaluate the findings of this study will be necessary. In conclusion, this study has highlighted the unhealthy paradox of wellness and nonadherence that occur in some women on breast cancer chemotherapy. Younger women with early disease were more involved and many socio-cultural beliefs as well as poor psychological adaptation may be associated with nonadherence among these women. Acknowledgment We acknowledge the support of all surgical residents, including Drs. Kunle Oke, Dare Esan, Olaogun and others who assisted in the collation of data for this work.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08033t2.jpg] [cr08033t1.jpg] |
| |||||||||

{kind=link}
{kind=link}