 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 4, No. 3, July-September, 2008, pp. 116-120 Original Article Quality of life outcome measures following partial glossectomy: Assessment using the UW-QOL scale Kazi R, Johnson C, Prasad V, De Cordova J, Venkitaraman R, Nutting CM, Clarke P, Evans PRhys, Harrington KJ Head and Neck Unit, Royal Marsden Hospital, 203 Fulham Road, London SW3 6JJ; The Institute of Cancer Research, 237 Fulham Road, London SW3 6JB Code Number: cr08035 Abstract Background: The consequences of a diagnosis of head and neck cancer and the impact of treatment have a clear and direct influence on well-being and associated quality of life (QOL) in these patients.
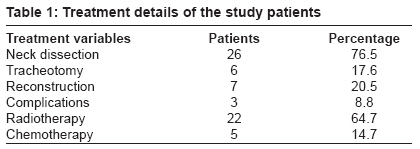
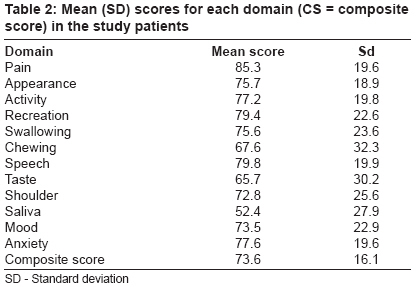
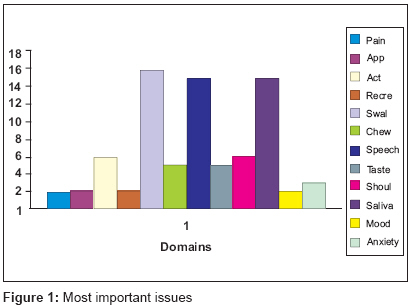
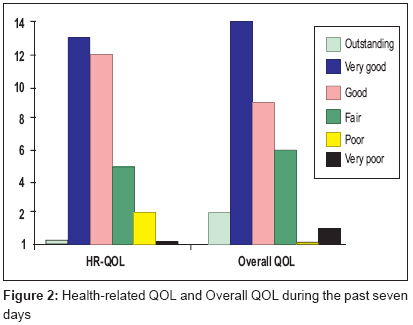
Keywords: Glossectomy, quality of life, questionnaire Introduction Patients with head and neck cancer (HNC) are vulnerable to psychosocial problems because social interactions and emotional expression depend to a great extent upon the structural and functional integrity of the head and neck region. [1],[2] The consequences of a diagnosis of head and neck cancer and the impact of treatment have a clear and direct influence on well-being and associated quality of life (QOL) in these patients. As surgery has progressed over the years with surgeons perfecting more complex techniques such as micro-vascular surgery, sensate reconstruction and organ preserving chemo-radiation, the simplistic view of using survival rates alone is not a sophisticated enough approach to assess the outcome of the modern cancer patient. [3],[4] While survival rates are similar for the different modalities patients and clinicians alike are looking increasingly to quality of life issues as a factor in deciding treatment plans. Now, more than ever, when it is clear that evidence based medicine is essential to good practice, it is important to try and evaluate the considerable impact of our interventions. It forces us to look at our techniques and think about other ways in which to perform procedures to not only improve survival but also life quality in general. A good example of this is the now accepted view that in laryngectomy patients, primary voice restoration using prosthetic speech is the management of choice. This does not affect survival rates but does improve the quality of life significantly. [5] QOL questionnaires/scales are increasingly being used in the United Kingdom. A recent questionnaire study by Kanatas and Rogers estimated that approximately 30% of clinicians involved in head and neck oncology are now using health related (HR- QOL) questionnaires. [6] However, they concluded that the lack of compliance despite the vast amounts of literature available on the importance of HR-QOL in head and neck cancer shows there is still some doubt over their potential usefulness. The University of Washington Head and Neck Quality of Life (UW-QOL) is a well-validated QOL instrument that was revised in 2002-3 to its current version 4 by Weymuller et al., to try and eliminate inconsistencies and improve on important missing elements in the spectrum of disease-specific response to treatment. [7],[8] Consequently, the UW-QOL (v. 4) contains 12 domains that allow the researcher to assess the effects of head and neck cancer and its treatment across the spectrum. The impact of a partial glossectomy on the QOL needs to be examined more carefully using patient self-report scales. Much of the limited work done before has been handicapped either by the small patient numbers, variety of assessment scales used or inadequate data. [9],[10],[11],[12],[13],[14],[15] No study has yet used the version 4 of the UW-QOL in oral/oropharyngeal cancer patients. Performing such cross-sectional studies is an excellent way to monitor practice and to identify and address areas of concern. Having large numbers of studies allows a comparison and alteration of current management in line with good evidence based practice. In this cross-sectional study we present our first experience of using the University of Washington QOL questionnaire in oral/oropharyngeal cancer patients who have undergone a partial glossectomy. Consequently, the purpose of this investigation was threefold: (1) to determine how effectively QOL can be assessed in partial glossectomy patients using the well-validated UW-QOL version 4 instrument; (2) to determine treatment variables that influence QOL; and (3) to compare these outcomes with those already reported previously in the literature. Materials and Methods Thirty-eight oral/oropharyngeal cancer patients who had undergone a partial glossectomy operation and were disease-free were identified from the Royal Marsden Hospital head and neck database. All 38 patients were sent the UW-QOL scale (version 4) by mail with a personalized covering letter providing information about the study along with a prepaid return envelope. The UW-QOL questionnaire is a simple, brief, well validated and widely used head and neck cancer-specific, self-administered scale. [7],[8] It consists of 12 domains: pain, appearance, activity, recreation, swallowing, chewing, speech, shoulder function, taste, saliva, mood, and anxiety that are assessed over the period of the last seven days. It also assesses the most important issues over the last seven days. The domains in the scale are simply scored on a scale ranging from 0 (worst) to 100 (best), to give a composite score that is computed as the arithmetic mean of the 12 individual domain scores (maximum score, 1200). The global QOL is a direct overall assessment of QOL and is determined by asking all patients to ′consider everything that contributes to your personal well-being - how would you rate your overall quality of life during the past seven days.′ The possible responses here are excellent, very good, good, fair, poor or very poor. Time from inception to completion of this cross-sectional study, approved by the local research and ethics committee, was 4 months. Statistical analysis Results We received thirty-four completed questionnaires from our initial cohort of thirty-eight patients with a resultant response rate of 89.5%. Responses were received from 26 males and 8 females with a mean age of 49.6 years (range: 28 to 73). Most of the questionnaires were received in the first week and all by the end of the fourth week. Median time since the operation was 31 months (12-258). All patients had undergone a partial glossectomy operation (surgical excision of half or less than half of the tongue as governed by the size/depth of the cancer). The treatment details of the study patients are shown in [Table - 1]. Of the patients who had a neck dissection, 14 had a selective neck dissection and 7 a modified radical neck dissection (no more details in 5 patients). No patient had a mandibular resection. Three patients underwent radial forearm free flap, two a pectoralis major flap, one latissimus dorsi flap and one an antero-lateral thigh flap reconstruction. The mean (SD) composite score of the QOL in our series of patients with glossectomy was reasonably high at 73.6 (16.1). We found that our patients scored well in general and across all the domains except in chewing, taste and saliva function [Table - 2]. Interestingly, although men scored higher than women (77.25 vs. 66.63), this was not significantly different with the exception of mood where women score significantly lower ( P = 0.03). All the domains were identified by the patients as important issues over the last 7 days. However, in particular, swallowing (n = 16, 47.1%), speech (n = 15, 44.1%) and saliva (n = 15, 44.1%) were most commonly cited [Figure - 1]. As regards the overall quality of life, 71.8 percent of our patients cited it as very good (43.7%) to good (28.1%) [Figure - 2]. QOL and treatment variables Discussion HNC and its treatment can have a profound effect on the patient′s physical, functional and emotional well-being. [1],[2],[3] Treatment for oral cavity or oropharyngeal cancers particularly is increasingly aimed at preserving vocal and swallowing function and this has resulted in a greater role for chemo-radiotherapy and organ-sparing surgery. Nonetheless, radical surgical excision, in the form of glossectomy (partial or total), reconstruction and surgery to the neck, pharynx and/or larynx, continues to play a central role in the management of these tumors. [1] Patients who have undergone a glossectomy present a range of challenges to the clinical team. The tongue is an organ of central importance that integrates the functions of articulation, mastication, deglutition, taste, airway protection, maintenance of oral hygiene and enjoyment of food. The impact of a glossectomy on a patient′s life can be significant and it is essential that their perspective is taken into account.[2],[3] Questionnaires provide a structured snapshot into the patients′ point of view. They facilitate multidisciplinary team working with the recognition of poor outcome groups, provide better information for the patient and their carers, and allow the opportunity to identify problem areas and target intervention. [4] We decided to use the University of Washington Quality of Life questionnaire, version 4 (UW-QOL), a HNC disease-specific questionnaire, because it is well-validated, brief, simple to process, and proven to provide clinically relevant information, particularly in HNC. [7],[8] We adopted a self-administration mode, because it avoids potential interviewer bias, is quick, simple, allows the patient to complete it at their convenience and is easy to process. Our study had a mix of male and female patients that was representative of current incidence trends. The results of this study demonstrate that partial glossectomees have a good global long-term QOL and a high composite score that is comparable to other studies in the literature. [9],[10],[11],[12],[13],[14],[15] This fact suggests that the impact of the operation on QOL is probably lower that one could expect and agrees with previous studies reporting that patients have good QOL and learn to cope with the disease in time. [3],[5] These relatively high rates of patient satisfaction may reflect the perceived success of effective multi-disciplinary team management of these patients. Although the composite score (sum of domain scores) in the scale is easy to compute and compare at first glance, it should be viewed with caution. This is because patients can tend to adjust/cope to their disabilities with time and this can cause a so-called ′cancellation effect′ (i.e., while one score is rising, another one is falling, and the total score does not change much). [8] We feel that the domain scores should be analyzed separately so that treatment-specific effects may then become apparent through contrasting specific responses within the domains. Swallowing, speech and saliva were the most commonly identified important issues as identified in our series. This is totally acceptable considering the location of these cancers. The low score would indicate a significant discontent and therefore this is an area which needs to be addressed and certainly be taken into account when deciding on treatment. In our study, we found that time since surgery, reconstruction, neck dissection, complications and radiotherapy were significant predicators of the QOL scores. Interestingly, our study group comprised patients who had their glossectomy some time ago and this may have had a bearing on the responses that we received. This is because they may be better adjusted to the effects of the operation on their voice related quality of life than previously. Much of the significant effects of radiotherapy on the domains of saliva, swallowing and chewing could be explained by its effect on the production of saliva that is essential for lubrication. [16] We also noticed that the saliva issue improved significantly with time and this is possibly due to habituation as well a palpable increase in the amount of saliva with time. While the negative effect of a neck dissection on shoulder mobility is clearly comprehensible, we can only hypothesize about the effect of complications and reconstruction on the mood and activity domains. Speech domain was significantly affected as a result of complications and this could be a result of further surgery/reconstructions that many of these patients consequently require. In our study, the younger patients were significantly more anxious than the older patients and this could be related to their active, professional status. In summary, the UW-QOL scale is a brief and simple scale that can be used effectively in oral and oropharynx cancer patients. The scale concerns issues that have been important in the last seven days, which are easy to recollect. It arms the clinician with useful information and can contribute to decision making based on patient feed-back. [11] The availability of open-ended text in the scale, albeit as a single item, provides yet another avenue of information regarding individual patients. We have received a variety of written comments, some of which have allowed us to recognize health care problems in need of attention that would have otherwise escaped our notice. In addition, it can help in audit, and research and assist in the making of patient information leaflets/videos. However, on the negative front, the UW-QOL scale is totally subjective with no room for clinician input and is closed format with only a single open-ended question. The strengths of this study include the relatively large patient numbers in a select group of partial glossectomees and the high response rate (close to 90%). Possible weaknesses include the cross-sectional nature of the study, selection and survival bias. However, the cross-sectional technique allows a subset of surviving patients to be identified and studied utilizing a single interaction (a questionnaire). We advise prospective longitudinal studies that adequately identify changes in QOL over a period of time and, indeed, eliminate the cancellation effect to an extent. To allow full assessment of changes in quality of life, large studies looking at scores over defined time periods and inter-departmental comparisons allow us to compare the overall progression of patients to an acceptable standard. However, such prospective studies are a labor-intensive and expensive enterprise. Even when thorough data collection is accomplished, other realities can compromise the usefulness of the data in light of the unavoidable drop-off of patients owing to recurrence, intercurrent death, lack of motivation or loss of follow-up. [12] Conclusion This cross-sectional study represents our first experience of using the University of Washington QOL questionnaire (version 4) in oral/oropharyngeal cancer patients who have undergone a partial glossectomy. In summary, the composite score and overall QOL as assessed using the UW-QOL scale (version 4) were high in our series of partial glossectomy patients and this could possibly be a reflection of adequate multi-disciplinary management. Swallowing, speech, and saliva are regarded as the most important issues. Stage of the disease, neck dissection, reconstruction, complications and radiotherapy were seen to significantly affect domain scores. The UW-QOL questionnaire is a simple and validated scale that can be effectively used in head and neck cancer patients. We strongly urge the use of prospective longitudinal studies and emphasize the importance of domain assessments to identify any QOL changes over time. References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08035f2.jpg] [cr08035t2.jpg] [cr08035f1.jpg] [cr08035t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}