 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
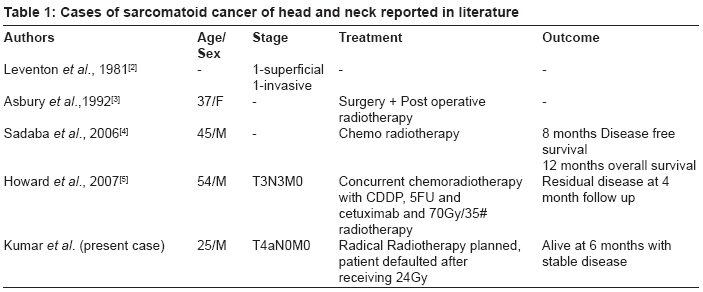
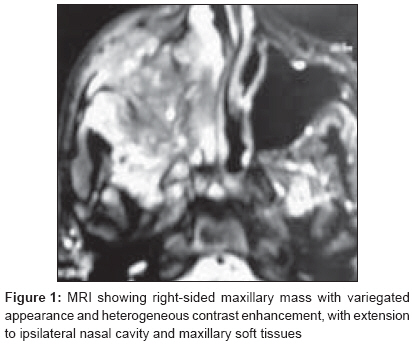
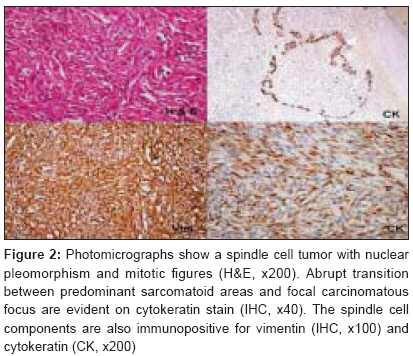
Journal of Cancer Research and Therapeutics, Vol. 4, No. 3, July-September, 2008, pp. 131-133 Brief Communication Sarcomatoid carcinoma of the maxillary sinus: A rare head and neck tumor Kumar Milind, Goyal Shikha, Bahl Amit, Das Prasenjit, Sharma DN, Ray Ruma, Rath GK Department of Radiation Oncology, All India Institute of Medical Sciences, New Delhi-110 029 Code Number: cr08038 Abstract Sarcomatoid carcinomas are rare tumors. These tumors have been reported at other sites, but head and neck origin is extremely uncommon. We report here a rare case of sarcomatoid carcinoma involving the maxilla. Only four such cases with maxillary origin have been discussed in English literature earlier. As compared to squamous cell carcinoma of maxilla, this variant is associated with poor prognosis and advanced disease at presentation, as was also seen in our case. There are no standard recommendations for management owing to the rarity of this histology. Surgery and radiotherapy form the mainstays of treatment. Exploration of the role of chemotherapy and novel targeted therapy agents is warranted in order to improve treatment results.Keywords: Head and neck, radiotherapy, sarcomatoid cancer Introduction Sarcomatoid carcinomas are biphasic tumors with both epithelial and sarcomatous elements. They can involve any organ and have been reported from diverse sites such as upper aerodigestive tract, esophagus, salivary glands, thyroid, thymus, lung, breast, gastrointestinal tract, hepatobiliary system, genitourinary tract and uterus. [1] Head and neck involvement is extremely rare. Maxillary involvement by this malignant tumor has been documented in only four cases prior to this report [Table - 1]. The other head and neck subsites reported include larynx, pharynx, oral cavity and nasal area in descending order. [2] The clinical presentation is usually advanced and follows an aggressive course. We present a case of sarcomatoid carcinoma involving the right maxillary antrum and briefly discuss the management of such cases. Case Report A 25-year-old man presented to our head and tumor clinic with complaints of numbness of the right side of the upper lip for eight months and right-sided facial swelling for last five months. Symptoms were progressive, with development of nasal obstruction, burning sensation and right-sided facial pain. There was no significant past medical history or any associated comorbid conditions. He gave a history of tobacco chewing for last fifteen years. On clinical examination the patient had a Karnofsky performance status (KPS) of 70, with fair nutrition. Fullness in right maxillary region was noted. Intraoral examination revealed a bulge in the right side of the hard palate with an 8x7 cm proliferative growth without any ulceration. Nasal speculum examination showed a fleshy mass filling the right-sided nasal cavity with nasal septum deviated to the left side. Visual acuity was 6/6 in both eyes. No neck nodes were palpable and cranial nerves examination was normal. Systemic examination was unremarkable. On imaging, a MRI scan revealed a mass arising from right maxillary sinus reaching up to base of skull, sphenoid sinus, and involving pterygoid plates medially and orbit superiorly; inferiorly the hard palate was involved [Figure - 1]. A biopsy taken from the palatal growth revealed a sarcomatoid carcinoma. On histopathology, both squamous cell and sarcomatoid components could be seen. The squamous cell carcinoma component consisted of polygonal cells exhibiting intracellular keratinization which was blending with the sarcomatous component of the tumor. Moderate to marked nuclear pleomorphism and hyperchromatic nuclei were also seen. On immunohistochemistry (IHC), the cells showed strong positivity for both cytokeratin and vimentin. The tumor cells were negative for smooth muscle actin (SMA), while the vascular smooth muscle cells showed positivity for SMA [Figure - 2]. The patient was diagnosed with Sarcomatoid carcinoma of the right maxilla, stage IVA (T4aN0M0). The patient refused surgery and was scheduled for definitive radiotherapy in view of young age and preserved general condition. Treatment was started on a Cobalt -60 unit but the patient defaulted for treatment after receiving a dose of 24 Gy over 12 fractions. Six months later on telephonic contact, the patient was symptomatically better with resolution of swelling in face and was taking analgesics for symptom relief. Discussion Sarcomatoid carcinomas are histopathological entities having a mixture of both carcinoma and sarcoma containing differentiated mesenchymal tissues. Morphologically, they may be either monophasic or biphasic (both epithelial and mesenchymal). In most cases, a dominant and a minor pattern may be recognized, though the two patterns are more commonly intermixed. Sarcomatoid carcinomas are known by variety of nomenclatures such as carcinosarcoma, pseudosarcoma, spindle cell squamous carcinoma, pleomorphic carcinoma, and carcinoma with pseudosarcomatous stroma.[2] However, the terminology of sarcomatoid carcinoma is preferred. [2],[3] On immunohistochemistry, immunopositivity with both cytokeratin and vimentin is seen, as in our case also. Morphologically, the cells are spindle shaped with marked to moderate pleomorphism. Two hypotheses for origin have been proposed. While the convergence hypothesis suggests origin from two stem cell lines, the divergence hypothesis suggests origin from a single stem cell differentiating into epithelial and sarcoma elements. It has been shown that the expression patterns of K-ras gene, p53 gene and X-chromosome inactivation are similar in both the epithelial and sarcomatous components giving support to origin from a single stem cell. Clinically they tend to present at an advanced stage, with most tumors being T3 or T4 at presentation and pursuing an aggressive course. Neck node involvement, which is uncommon in squamous cell carcinomas of maxilla, may be present. [4] Leventon et al. have proposed depth of invasion by the tumor to be the most important prognostic criterion, with deeper infiltration indicating a poorer survival. [2] These tumors need to be differentiated from pure spindle cell carcinomas and epitheloid sarcomas. Spindle cell carcinomas are monophasic tumors resembling soft tissue sarcoma with immunohistochemical evidence of epithelial differentiation. True carcinomatous elements are not present in such tumors and this helps to distinguish them from sarcomatoid carcinomas. [5] Epitheloid sarcomas are unusual low grade sarcomas with tendency for local recurrence. They are biphasic tumors with evidence of both epitheloid and spindle-shaped tumor cells. Epithelioid sarcoma tends to grow in distinct, cohesive nodules with central areas of hyalinization and necrosis. They can be differentiated from squamous cell carcinoma by the absence of keratin pearls and dyskeratosis. Absence of epitheloid cells would help in differentiating them from sarcomatoid carcinomas. [6] Treatment is usually planned on the lines of squamous cell carcinoma of maxilla and usually consists of surgery followed by post operative radiotherapy. [7] Owing to the advanced presentation at diagnosis, surgery is often ruled out. In such cases, chemoradiation may be used as an alternative. Cisplatin based chemotherapy may be tried as part of neoadjuvant or adjuvant strategies. [8] Conclusions Sarcomatoid carcinoma of maxilla is a rare aggressive tumor with poor prognosis. Surgery and radiotherapy form the mainstay of treatment. Exploration of the role of chemotherapy and novel targeted therapy agents is warranted in order to improve treatment results.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08038f1.jpg] [cr08038t1.jpg] [cr08038f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}