 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
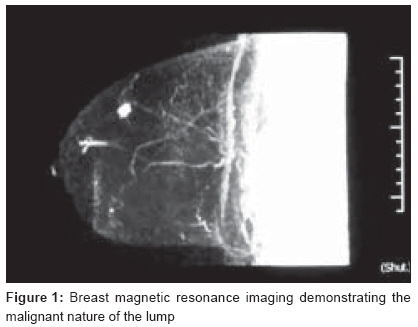
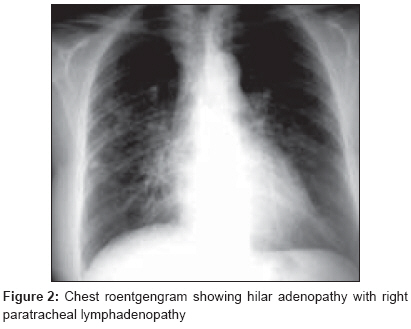
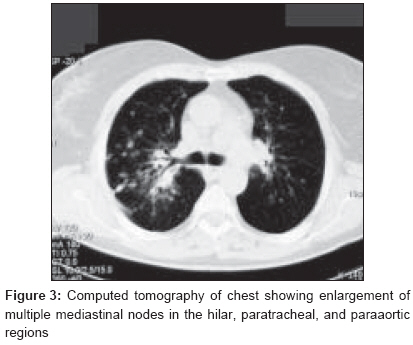
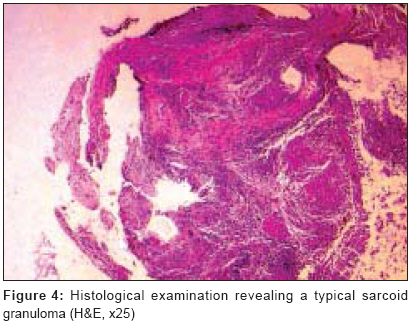
Journal of Cancer Research and Therapeutics, Vol. 4, No. 3, July-September, 2008, pp. 134-136 Case Report Pulmonary sarcoidosis simulating metastatic breast cancer Dragoumis DimitriosM, Tsiftsoglou ArisP, Assimaki AnthoulaS St Luke's Hospital, Department of General Surgery, Breast Division, Panorama, 55 236, Thessaloniki Code Number: cr08039 Abstract The clinical appearance and imaging findings of sarcoidosis and breast carcinoma may sometimes mimic one another, making the differential diagnosis between these two diseases difficult in some cases. A 69-year-old woman displayed an irregular shaped lesion in her left breast. Preoperative localization modalities detected a breast mass with malignant characters. The patient also was found to have pulmonary findings for metastatic disease on chest computed tomography. These features were proven upon biopsy to be consistent with sarcoidosis. The patient underwent breast surgery, adjuvant chemoradiotherapy and hormonal therapy, while corticosteroids were administered for pulmonary sarcoidosis. The patient is well 12 months later, without recurrence. An unfortunate consequence of the presence of both entities in the same patient is the risk of misguided differential diagnosis and incorrect therapeutic strategy. This patient shows the importance of confirming a clinical diagnosis of sarcoidosis with appropriate biopsies and histological examination, prior to initiation of breast cancer therapy. Keywords: Breast cancer, lung metastasis, pulmonary sarcoidosis Introduction Malignancies can cause mediastinal and hilar lymphadenopathy that is easily mistaken for sarcoidosis. Breast cancer can metastasize to intrathoracic lymph nodes, but it is uncommon for mediastinal or hilar lymphadenopathy to be the prevailing feature of this disease. Lymphadenopathy, however, is common in sarcoidosis and is rarely symptomatic. In this situation, proper diagnostic assessment is essential for disease management and highlights the problem of considering enlarged mediastinal lymph nodes in patients with high risk of relapse, to be the obvious sites of metastases. [1] We report a patient with breast cancer, who initially had signs of metastatic disease to the lung on chest computed tomography. Despite the rarity of breast cancer manifesting in this way, the importance of obtaining histological confirmation of suspected sarcoidosis is stressed.Case Report A 69-year-old non-smoking woman became aware of a small lump, located in the left upper medial quadrant. Her mother and one cousin had breast cancer. Menarche had occurred at the age of 11 years old. She had two miscarriages and one induced abortion in her gynecological history. On physical examination, a hard, non-tender mass, approximately 2 cm in diameter, was detected in the left upper medial quadrant. Mammography demonstrated a dense mass with ill-defined margins, which corresponded to the palpable mass, while breast ultrasonography confirmed the presence of a solid lesion with irregular margins occupying the upper quadrants of the left breast. Moreover, a subsequent breast magnetic resonance imaging (MRI) documented this spiculated lesion with heterogeneous contrast enhancement [Figure - 1], highly suggestive of malignancy. Breast fine-needle aspiration cytology (FNA) confirmed the malignant nature of the mass. Preoperative chest radiograph [Figure - 2] and computed tomography unexpectedly revealed multiple nodular lung masses and mediastinal lymphadenopathy [Figure - 3]. The patient had no previous occupational or environmental exposures. She denied dyspnea, chest pain, wheezing, fatigue, or weight loss. Pulmonary tests detected no abnormalities. Despite the obvious suspicion of metastatic breast cancer, a fiberoptic bronchoscopy was performed and biopsy samples were received from enlarged paratracheal lymph nodes. Histological examination and transbronchial aspiration cytology revealed no evidence of malignant disease, but instead showed non-necrotizing sarcoid granulomas, with large Langahns giant cells within [Figure - 4]. The patient eventually underwent a wide segmental excision of the left breast, including axillary lymph node dissection. The histological essay reported a lesion measuring 18 x 16 mm, which was recorded as a grade III, infiltrating ductal breast carcinoma and two of 11 lymph nodes were found to have evidence of metastatic disease. On immunostaining, the neoplastic cells expressed progesterone and estrogen receptors, but they did not express HER 2/neu. After surgery, six courses of 5-fluoruracil, epirubicin, and cyclophosphamide were administered followed by radiotherapy to the left chest area. As regards to the sarcoidosis, the patient received prednisone for eight weeks and significant remission of the disease was observed. The patient currently is being treated with anastrazole. Follow-up is satisfactory to date and 12 months later she remains well, without any signs of recurrence. Discussion Sarcoidosis is a granulomatous inflammatory disease, the cause of which remains largely unknown. Many features are suggestive of an infectious origin, whereas other studies underline the genetic factor. Chronic inflammation is associated with an increased risk for malignant lymphomas or cancer in the affected tissue. Theoretically this would apply also to sarcoidosis, which most frequently involves intrathoracic organs such as the lungs, the liver, and the skin. Little is known, however, about cancer incidence following sarcoidosis. [1],[2],[3] Various malignant neoplasms can develop in patients with sarcoidosis, and carcinomas can produce sarcoid-like reactions in lymph nodes. Malignancies also can have radiological characteristics that are easily mistaken for sarcoidosis. Histological confirmation is desirable before establishing a diagnosis of sarcoidosis. [2],[3] Although there has been much speculation upon the relationship between sarcoidosis and cancer, this association still remains indistinct. Patients with sarcoidosis appear to be at increased risk for malignancies, particularly for carcinomas of the lung, small intestine, stomach, liver, skin and leukemia. The estimated relative risk for breast cancer, in particular, is slightly higher than that observed in other chronic diseases such as diabetes, inflammatory bowel disease and rheumatoid arthritis. [4] The lung is the most common intrathoracic site of breast cancer metastasis. Pulmonary metastases from breast cancer are disseminated hematogenously, and the nodules are typically multiple, bilateral and peripheral in distribution. The nodules are usually sharply marginated and range in size from several millimeters to several centimeters in diameter. Multiple pulmonary nodules are common findings in lung metastasis from breast cancer, while the development of a solitary pulmonary nodule in patients previously treated for breast cancer may usually represent something other than recurrent disease, such as primary lung cancer or a benign lesion. Nodal metastases are detected on chest radiograph in 25% of patients with breast cancer. Cavitation of metastatic nodules is a rare feature at radiography. However, cavitation in metastatic adenocarcinoma, including breast cancer, is frequently encountered in computed tomography. The axially, mediastinal and hilar are most commonly involved. [5],[6] On the other hand, the diagnosis of systemic sarcoidosis typically consists of compatible radiologic imaging signs (bilateral hilar lymphadenopathy and pulmonary infiltration), biopsy evidence of noncaseating granulomas, and excludes other conditions that may have noncaseating granulomas on histology. The absence of extrapulmonary symptoms (such as fatigue, erythema nodosum, fever, arthralgia or weight loss) and the localization of the nodules do not necessarily eliminate or establish a diagnosis of sarcoidosis. [5] There are series in the literature that have attempted to assess the risk of breast distant metastases to these lymph nodes. In an autopsy, Abrams et al . reported that 66% of breast cancer patients had lymph node involvement and 77% had pulmonary parenchyma involvement. In another study of women with known metastatic breast carcinoma, the incidence of mediastinal lymphadenopathy was 24%. [7] As referred above, tissue analysis is essential for differential diagnosis of enlarged intrathoracic lymph nodes. The usual method of obtaining diagnostic tissue is transbronchial biopsy. The technique of transbronchial biopsy is a safe, simple and successful alternative to mediastinoscopy sampling of mediastinal lymph nodes. The accuracy of transbronchial cytology in the diagnosis of mediastinal sarcoidosis is dependent on the needle gauge, the bronchoscopist′s skill and the efficiency of the cytology laboratory. In some cases, further invasive procedures might be needed, such as mediastinoscopy or open-lung biopsy. [8] In conclusion, this rare coexistence of breast cancer and sarcoidosis highlights the fact that patients with prior malignancies need a thorough preoperative evaluation with histologic confirmation of the non-malignant nature of the mediastinal lymphadenopathy, thereby allowing the choice of correct curative strategy, without dangerous overtreatment regimes. Acknowledgment The authors thank Aikaterini Sikou for her assistance during the preparation of this manuscript.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08039f4.jpg] [cr08039f1.jpg] [cr08039f3.jpg] [cr08039f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}