 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
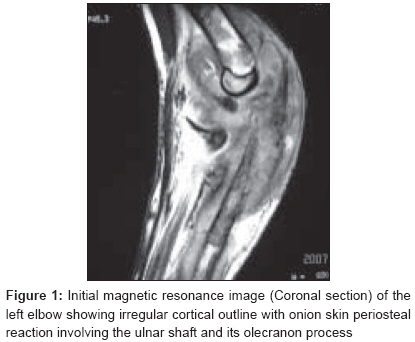
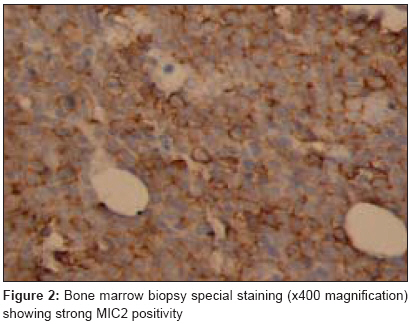
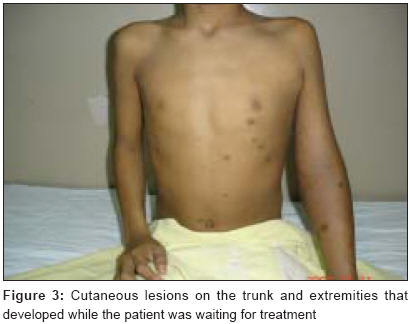
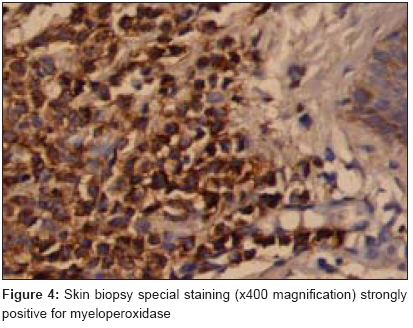
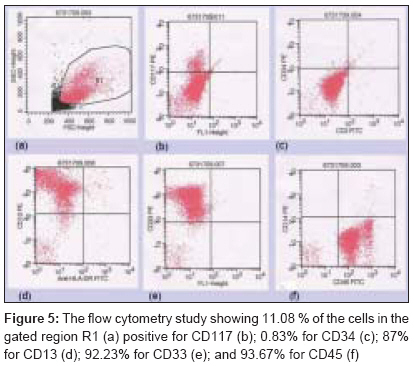
Journal of Cancer Research and Therapeutics, Vol. 4, No. 3, July-September, 2008, pp. 137-139 Case Report Granulocytic sarcoma masquerading as Ewing's sarcoma: A diagnostic dilemma Haresh KunhiParambath, Joshi Nikhil, Gupta Chaitali, Prabhakar Ramachandran, Sharma Daya Nand, Julka PramodKumar, Rath GouraKishor Department of Radiotherapy and Oncology, All India Institute of Medical Sciences, New Delhi-110 029 Code Number: cr08024 Abstract An eleven-year-old boy presented with a swelling in his left elbow. Radiologically the features were that of an Ewing's sarcoma involving the ulna. Histopathology showed small round cell tumor strongly positive for Monoclonal Imperial Cancer research fund 2 (MIC2) antigen. Similar cells in the bone marrow were involved with MIC2 positivity. The patient developed skin lesions, which on biopsy were found to be chloromas. The initial biopsies were reevaluated with special stains revealing granulocytic sarcomas in acute myeloid leukemia masquerading as Ewing's due to its MIC2 positivity. The possibility of myeloid neoplasms should be considered routinely with known MIC2 positive round cell tumors.Keywords: Acute myeloid leukemia, chloroma, extra-medullary myeloid tumor, Ewing′s sarcoma, granulocytic sarcoma Introduction Granulocytic sarcoma (GS), also called myeloblastoma or myeloid sarcoma is a rare solid tumor composed of immature myeloid cells. It was first described in 1811. Such tumors often display a greenish color due to the enzymatic action of myeloperoxidase in the tumor cells; hence, the term "chloroma" was given to this lesion in 1853. [1] More recently the term extra-medullary myeloid tumor (EMMT) has been proposed to include all forms of extra-medullary myeloid leukemic infiltrates. [2] GS is a rare occurrence with an estimated incidence of 0.7 per million in children and 2 per million in adults.[3] This tumor occurs in about five percent of adults and 13% of children with myeloid leukemias. In autopsy series, GS occurs in two to eight percent of patients with acute and chronic myelogenous leukemia. [2] They occur most commonly in bone, periosteum, soft tissues, lymph nodes and skin, but can occur virtually anywhere. [4]Case History An eleven-year-old boy presented to a local hospital with a history of fall. As he had sustained some injuries to his elbow, a plaster cast was applied for 40 days. On removal of the cast the doctor noticed a swelling in the left elbow involving the lower third of the arm. Skin was tense with dilated veins over it. Movement of the elbow was restricted and painful. X-ray of the elbow showed peri-osteal reaction involving proximal and middle third of the shaft of ulna including the olecranon process. There was evidence of radiolucency with sclerotic changes in the medullary area with irregularity of the cortex and soft tissue swelling in the forearm. Magnetic resonance imaging of the elbow [Figure - 1] showed irregular cortical outline with onion skin periosteal reaction involving the ulnar shaft and its olecranon process. Marrow signal intensity was altered. Tumor was hypointense on T1 and mixed signal intense on T2 weighted / Short tau inversion recovery (STIR) images. There was an associated large infiltrative soft tissue mass encasing the ulnar shaft and involving almost the entire surrounding musculature of the forearm. Soft tissue component was seen to cross the elbow joint with involvement of the lower end of the humerus for a length of 5 cm. Neurovascular structures were involved. The patient further underwent an open biopsy from the ulnar swelling at the local hospital. Histopathology revealed a malignant round cell tumor. He was then referred to us. Bone marrow biopsy done at our hospital showed deposit from a malignant small round cell tumor with strong Monoclonal Imperial Cancer research fund 2 (MIC2) antigen positivity [Figure - 2]. A complete blood count, liver and kidney function tests were normal. Based on these clinical, radiological and histopathological features, a diagnosis of round cell tumor, possibly Ewing′s sarcoma (ES) metastasizing to marrow was considered. While awaiting definitive treatment, the boy developed skin lesions on anterior and posterior abdomen and in the arms. [Figure - 3] shows well defined round violaceous elevated dome shaped rubbery plaques over trunk and upper extremities suggestive of cutaneous metastases. Biopsy from one of these lesions showed a thinned out epidermis. Dermis as well as subcutaneous tissue showed diffuse infiltration by round cells which have scanty to moderate cytoplasm with vesicular nuclei. These neoplastic cells were immunoreactive for myeloperoxidase [Figure - 4] and leucocyte common antigen. Cells were negative for T-cell, B-cell markers, synaptophysin and chromogranin. In view of morphology and immunohistochemistry, a diagnosis of hematopoietic malignancy of myeloid origin with leukemia cutis was considered. With this background, special stains were then performed on the initial bone marrow biopsy. The neoplastic cells in the bone marrow were found to be positive for myeloperoxidase and leucocyte common antigen. The flow cytometry study showed that 11.08% of the cells in the gated region are positive for CD117; 0.83% for CD34; 87% for CD13; 92.23% for CD33; and 93.67% for CD45 [Figure - 5]. Cytogenetic study showed 46 XY chromosome status with Promyelocytic leukemia-Retinoic acid receptor alpha (PML RAR alpha) negative by polymerase chain reaction (PCR). Thus a final diagnosis of Acute Myeloid Leukemia (AML) with GS involving skin, bone and soft tissue in the elbow was reached. The patient was then referred for chemotherapy. Discussion The radiological features in our case initially suggested a diagnosis of Ewing′s sarcoma. Other small round cell tumors include Neuroblastoma, Wilms tumor, Rhabdomyosarcoma (RS) and Desmoplastic Small Round Cell Tumor (DSRCT). Among the small round cell tumors (SRCT), MIC2 expression is not limited to ES and primitive neuroectodermal tumors (PNET), but also shows strong and reliable expression in lymphoblastic lymphomas and related leukemias. Rhabdomyosarcoma and DSRCT can also be MIC2 positive. MIC2 analysis continues to be helpful in the diagnosis of SRCT, provided that a panel of antibodies is used. [5] Light microscopy and a limited panel of immunohistochemical markers can cause misdiagnosis of small round cell tumors and to prevent this, the markers should include cluster of differentiation (CD)79a, CD43, Terminal Deoxynucleotidyl Transferase (TdT), CD10 and CD34 if lymphoma is suspected, in addition to other routine markers. None of these markers are positive in ES. In controversial cases, gene rearrangement by PCR also can be of great value. Positive immunoglobulin heavy chain gene rearrangement (IgH-R) or T cell receptor gamma chain gene rearrangement (TCR-R), never positive in Ewing′s sarcoma, will support the diagnosis of lymphoma or lymphoblastic leukemia. Similarly demonstration of Ewing′s sarcoma - Friend leukemia virus integration 1 gene (EWS/FL-1) fusion transcript by reverse transcriptase-PCR will support the diagnosis of ES/ (PNET). [6] We suggest a cost-effective and comprehensive antibody panel comprising of LCA, MIC2, CD34, Myeloperoxidase, Myogenin and Desmin in the differential diagnosis of SCRT. GS is a tumor that is also frequently misdiagnosed especially in a negative clinical setting (i.e. with no previous history of myeloid malignancy). In one series the initial diagnosis was correct in only 44% of 61 cases with the most common other histologic diagnoses including malignant lymphoma, small cell carcinoma, sarcoma (ES and PNET) and undifferentiated neoplasm. [1] Chloroma or GS can develop in a patient who does or does not have leukemia as a soft tissue mass, raising the differential diagnosis of round cell sarcomas. MIC2 expression has been frequently used as a marker, differentiating ES/PNET or lymphoblastic neoplasia from other round cell tumors. However, because of the high incidence of detectable MIC2 expression in myeloid hematopoietic neoplasms, the use of CD99 immunoreactivity is of limited value in the differential diagnosis of round cell sarcomas versus lymphoblastic lesions versus chloroma, particularly in patients who do not have leukemia. Instead, the possibility of myeloid neoplasms, including chloromas, should be considered routinely with the known MIC2 positive round cell tumors, such as ES/PNET, lymphoblastic lesions, and others. [7] References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08040f2.jpg] [cr08040f3.jpg] [cr08040f4.jpg] [cr08040f1.jpg] [cr08040f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}