 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
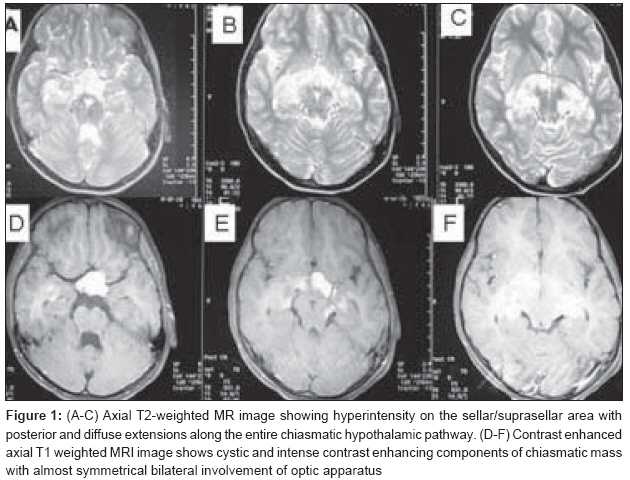
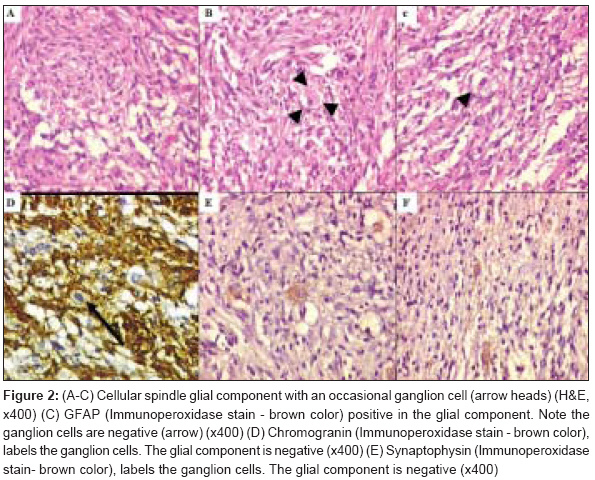
Journal of Cancer Research and Therapeutics, Vol. 4, No. 3, July-September, 2008, pp. 140-143 Case Report Suprasellar ganglioglioma with unusual diffuse involvement of the entire optico-chiasmal hypothalamic pathway Jalali Rakesh, Deopujari ChandrashekarE, Bhutani Ritu, Suhas U, Rajasekharan Preetha, Kane ShubdhaV, Gupta Tejpal Departments of Radiation Oncology and Pathology, Tata Memorial Hospital, Mumbai and Neurosurgery, BJ Wadia Hospital, Mumbai Code Number: cr08041 Abstract Gangliogliomas (GG) are mixed glioneuronal tumors of the central nervous system (CNS), occurring mostly in the pediatric population, with common sites being temporal lobes and less commonly in the frontal and parietal lobes. We report a case of a 7-year-old child who presented with bilateral visual defects for 6 months. Magnetic resonance imaging (MRI) of the brain revealed an intensely enhancing mass lesion with calcification in the sellar and suprasellar region involving the optic chiasm and the left optic nerve. The mass showed almost bilaterally symmetrical diffuse spread along the optic tracts posteriorly and hypothalamus, temporal lobes, thalami and the basal ganglia. The lesion was radiologically indistinguishable from chiasmatic astrocytoma or a germ cell tumor but histopathological features were of a ganglioglioma. While a few optic apparatus gangliogliomas have been reported in the literature, such widespread diffuse involvement of the entire optico-chiasmal hypothalamic pathway is unusual.Keywords: Chiasmal hypothalamic tumors, ganglioglioma, histopathology, imaging, optic apparatus Introduction Gangliogliomas (GG) are mixed glioneuronal tumors occurring mostly in children, where they constitute 5-8% of all brain tumors. [1] Seizures are the commonest presentation reflecting involvement of temporal lobes commonly, but they can involve any part of the neuraxis. [2] We report a rare case of a suprasellar ganglioglioma with an unusual spread along the entire optic chiasmal hypothalamic pathway and adjoining structures with a special emphasis on its imaging characteristics, histopathology and management.Case Report A 7-year-old girl with normal developmental milestones presented with gradual but progressive diminution of vision in both eyes since 6 months. Ophthalmic examination confirmed reduced visual acuity with only perception of light in the left eye. Her higher mental functions were normal for age and no focal neurological deficits were elicited. There were no detectable neurofibromatosis-1 (NF-1) features. Magnetic resonance imaging (MRI) of the brain revealed a lesion in the sella extending into suprasellar and left parasellar regions compressing and displacing the optic chiasm. The lesion was isointense on T1-weighted images; hyperintense on T2-weighted and fluid attenuated image recovery (FLAIR) sequences, with uniform contrast enhancement [Figure - 1]. Altered signal intensity was also noted in medial aspect of bilateral temporal lobes, thalami, hypothalamus and basal ganglia. The abnormal signal intensity extended along the optic tracts bilaterally almost symmetrically in multiple areas raising a suspicion of optic pathway glioma. Because of the intense enhancement and spread, a germ cell tumor was also considered. Therefore, preoperative serum and CSF tumor marker assays (beta HCG and AFP) were also carried out but were not found to be elevated. Other hormone profiles in steroid and thyroid axes were within normal limits. The patient underwent a bifrontal craniotomy wherein the right optic nerve was visualized to be normal. The distal portion of the left optic nerve was seen embedded in the tumor that arose from the chiasmal-hypothalamic area. As no exophytic component was seen and the whole chiasm appeared thickened, surgical decompression was not possible. Biopsy was taken from a definitely abnormal area so as not to disturb the vision any further. On light microscopy, the mass appeared as a low-grade mixed glioneuronal tumor composed of neoplastic spindle-shaped astrocytes arranged in sheets and vague fascicles with scattered ganglion cells [Figure 2 A-D]. The neuronal component consisted of sparse, singly scattered, irregular, dysplastic and dysmorphic ganglion cells amidst a fibrillary astrocytic background. Reticulin stain highlighted the reticulin fibers around the vessels. Interspersed thick-walled blood vessels were noted. No conspicuous perivascular lymphocytic infiltrate was seen. On immunohistochemistry (IHC), the ganglion cells stained positively with synaptophysin and chromogranin [Figure 2D] and [Figure 2E] while the astrocytes were positive for glial-fibrillary acidic protein (GFAP-[Figure 2C]). Both the components of the tumor were CD34 negative. Based on these histomorphological features, a diagnosis of an optic pathway ganglioglioma was established. In view of the residual mass and presence of visual deficits, adjuvant treatment in the form of radiation and chemotherapy were considered and discussed with the family. After discussion and appropriate consent, the patient was treated with high-precision stereotactic conformal radiation therapy (SCRT) to a dose of 54 Gy in 30 fractions, which she tolerated well. She is clinically well on the last follow-up. Discussion Temporal lobes are the commonest location for gangliogliomas, but they have been known to arise from other supratentorial sites such as the frontal, parietal and occipital region, and rarer sites include the cerebellum, brainstem and spinal cord.[2] Sellar and suprasellar areas are rare sites of involvement and a few cases have been reported. [3],[4],[5],[6],[7],[8],[9] The optic pathway GG is radiologically indistinguishable from an optic glioma. On MRI, it is iso-to-hypointense on T1-weighted images, hyperintense on T2-weighted and FLAIR images and shows on variable contrast enhancement either a nodular rim or a solid pattern.[1],[2] The differential diagnoses of suprasellar lesions in children include neoplastic conditions like hypothalamic glioma, craniopharyngioma, germ cell tumors, and pituitary adenomas; or non-neoplastic conditions such as granulomatous diseases and benign cysts. A diagnosis of chiasmatic hypothalamic glioma was considered preoperatively in our case, especially in view of the characteristic involvement of the optic pathway bilaterally, which would not occur generally with any other condition. The pathology report of a ganglioglioma was therefore a histological surprise. The nearly symmetrical bilateral involvement of the entire chiasmatic hypothalamic pathway with posterior extension along the optic tracts almost reaching the visual cortex in our case was indeed unusual, a finding hitherto rarely described previously with only one possible similar case of multifocal involvement of the optic apparatus reported in the indexed English medical literature. [9] The pathologic criteria of a GG include irregular groups of large, dysplastic, multi-polar neurons admixed with glial tumor surrounded by a reticulin network. [2],[10] The glial component is generally pilocytic or fibrillary, but ependymal and even oligodendroglial components are described. Eosinophilic granular bodies, hyaline bodies, microcystic changes, calcification, desmoplasia and perivascular lymphocyte infiltration may be present variably. [6],[10] The case under discussion shows astrocytic component with no significant mitotic activity, with singly scattered dysmorphic ganglionic cells. No significant increase in reticulin fibers or perivascular lymphocytic infiltrate was noted. The neuronal (ganglionic) cells were highlighted by the immunoreactivity to synaptophysin and chromogranin with negativity for glial-fibrillary acidic protein (GFAP); whereas the glial components were positive for GFAP. [6] More importantly, the ganglionic cells were dysmorphic with irregular shaped nuclei, which is not a feature of caught up neurons within the fibrillary astrocytomas. No definite binucleated ganglionic cells were seen but these are seen in only about 50% of cases [11] and moreover, in the present case the histological features are limited by the sample size of a biopsy rather than of total excision. No definite molecular pathogenetic pathway has been identified for gangliogliomas to date, but most of the typical cases occurring in temporal lobe are thought to have hamartomatous origin and approximately 80% of these have shown to be CD34 positive. [11] The case under discussion is from the optic pathway, which is one of the rarest sites reported in the English literature and the significance of diagnostic role of CD34 immunostaining in the diagnosis of gangliogliomas occurring at uncommon sites is not really known. Unlike ganglioglioma (GG) of other locations, treatment options for a GG at a critical location are controversial and include observation with adjuvant therapy reserved for recurrent/refractory conditions and where clinical progression can be documented . In our patient, there was a diffuse involvement of the optic apparatus sparing only the right optic nerve with no definite exophytic mass that could be excised safely without a potential risk of causing additional neurological effects. The preoperative impression being that of a chiasmatic glioma, only a biopsy was taken with a view to preserve the vision. We considered the condition to be akin to optic pathway glioma and hence decided to treat it with adjuvant therapy. Experience with chemotherapy in a ganglioglioma is relatively limited and hence radiotherapy was considered a reasonable option. In view of the patient′s age and the affected site, she received conformal radiation therapy under high precision stereotactic guidance and has a good chance for a long-term prognosis. Gangliogliomas are mixed glioneuronal tumors that rarely involve the optico-chiasmal hypothalamic pathway. Radiologically they are indistinguishable from optic pathway gliomas and require appropriate histopathological criteria for definitive diagnosis. A well-demarcated lesion with calcification in the optico-chiasmal hypothalamic pathway in the pediatric population should alert the clinician in considering ganglioglioma as a possible differential diagnosis. References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08041f1.jpg] [cr08041f2.jpg] |
| |||||||||

{kind=link}
{kind=link}