 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
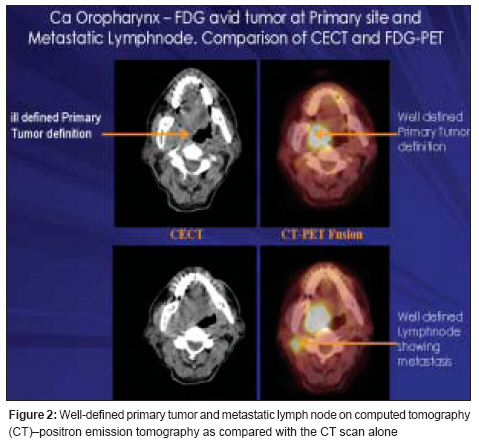
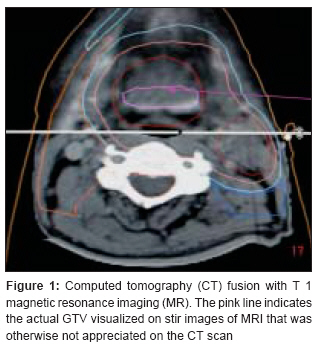
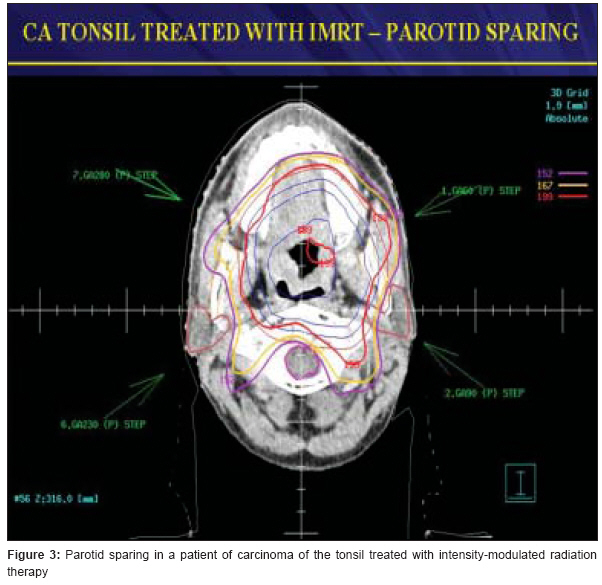
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 148-150 INVITED EDITORIAL Intensity-modulated radiation therapy for head and neck cancer in India: A promise waiting to be delivered Anand AK Department of Radiation Oncology, Rajiv Gandhi Cancer Institute and Research Centre, New Delhi Code Number: cr08046 Intensity-modulated radiation therapy (IMRT) was introduced as an innovative method of delivering radiation therapy by varying the intensity of radiation across a beam. It has virtually revolutionized the dose distribution capability not only in the tumor volume but also in the surrounding and often in the dose-limiting organs/structures. Hence, often, we fail to deliver the desired dose to the tumor because of the limited radiation tolerance of the critical structures in the vicinity of the tumor volume, like spinal cord, brain stem, optic apparatus, etc. It can be well imagined that such a situation can lead to either a compromise in tumor control or an unacceptable normal tissue toxicity. We started IMRT in July 2003 with a compensator-based technique, and one and a half years later the multileaf collimator-based delivery with a "step and shoot technique" [Figure - 2] was introduced. IMRT is still in its infancy, especially in our country, and several issues need to be emphasized to launch and sustain a successful IMRT program across the country. First and foremost is the training of medical professionals, medical physicists and technologists in various aspects of IMRT. Radiation oncologists are today required to be abreast with a thorough knowledge of radiological anatomy with respect to computed tomography (CT) scans, magnetic resonance imaging (MRI) scans and, now, CT-positron emission tomography (PET) scans. Until recently it was not a part of the curriculum of the post graduate program in Radiation Oncology and, therefore, all radiation oncologists had to learn to "read" (of course with the help of radiodiagnosis colleagues) CT scans and MRI scans themselves. IMRT is much less forgiving than conventional radiation and if one misses the subtle extension of the tumor in planning scans the intended dose would not be delivered to the desired volume, leading to "geographic misses" or "marginal failures." Another factor is the considerable interobserver variation in gross tumour volume and clinical target volume among various radiation oncologists, which can potentially lead to variation in tumor control or adverse effects. Interobserver variation can reduce with experience or by utilizing additional facilities such as CT-MRI fusion or CT-PET fusion. Several publications have reported that MRI and PET scans [Figure - 1] and [Figure - 2] can significantly change the tumor volume (GTV), which was delineated on the CT scan alone. These additional modalities also help in reducing the interobserver variations. IMRT planning is laborious and demanding for both the radiation oncologists and the medical physicists. Beam optimization, dose to non-target structures, number of segments, dose homogeneity and conformity are some of the issues involved in the day-to-day planning. During the course of 6-7 weeks of treatment, a number of variabilities arise due to tumor regression or loss of weight of the patient and often a decision has to be made whether there is need for replanning. It is again time consuming and stretches the resources of the department. Radiation oncologists and medical physicists also have to tackle the issues of interfractional and intrafractional tumor motion. Quality control is perhaps the biggest issue in IMRT because there are very tight margins around the tumors. Each department has to know its own "set-up uncertainties" and follow strict protocols for quality assessment (QA). Different machines have different tools for QA, which should be exploited to the fullest. A major development in this regard is the advent of image-guided radiation therapy with megavoltage (MV) imaging (EPID), kilovoltage (KV) imaging, and cone beam CT (KV or MV). How often these procedures need to be performed - daily, on alternate days, or weekly - depends on the site of tumor location and its organ motion. However, all these facilities come at a cost and IMRT is both labor intensive and expensive. Despite all these limitations, IMRT offers several distinct advantages in head and neck cancers (HNCs). Xerostomia, as we all have witnessed, is one of the most distressing long-term morbidity of head and neck radiation seen in 60-95% of the patients. It causes dental caries and adversely affects the quality of life, especially speech and swallowing. IMRT can prevent Xerostomia by limiting the dose to parotid glands in about 70-80% of the patients. It is the single most important indication of IMRT in HNC if more than two-thirds of the parotid gland enters the radiation field [Figure - 3]. Our own experience (J Clin Oncol. 2006:18:497-504) is also similar and very gratifying for both patients and radiation oncologists. Chronic dysphagia is another distressing complication seen in long-term survivors after head and neck radiation. Radiation therapy is thought to induce fibrosis and abnormal motility of the muscles of deglutition. Structures responsible for dysphagia include pharyngeal constrictors and the glottic and supraglottic larynx. Moderate sparing of these structures is achievable with IMRT. In our series of HNC patients treated with IMRT, 77% had no long-term dysphagia (under publication in BJR). Regarding the impact of IMRT on locoregional control and survival, most of the data have come from single institutional phase-II studies. The 2-year locoregional control rates of 60-70% have been reported, which compare favorably with conventional radiation. Other techniques of dose escalation like simultaneous integrated boost are being exploited to further improve the locoregional control. Although there is only a modest impact of IMRT on locoregional control and survival, it still seems a preferred modality of treatment for patients with HNCs. It seems justified because of its profound favorable impact on long-term morbidities associated with radiation therapy, especially Xerostomia and chronic dysphagia. It has resulted in an improvement in the quality of life of HNC patients treated with a curative dose of radiation with or without concurrent chemotherapy. To that extent it has fulfilled its promise. Future clinical trials with newer drugs and escalated radiation doses will answer the question of improvement in locoregional control and survival. Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08046f3.jpg] [cr08046f2.jpg] [cr08046f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}