 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
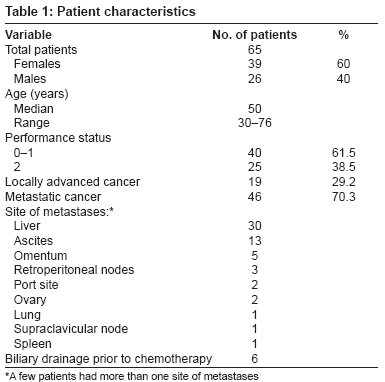
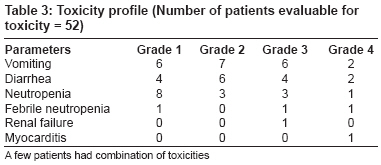
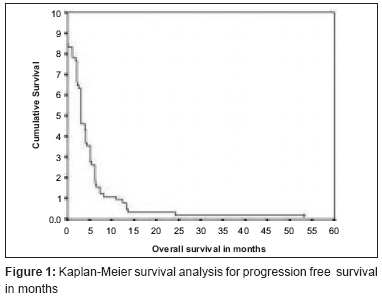
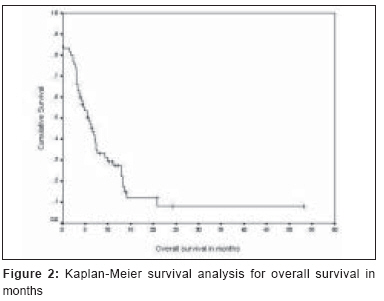
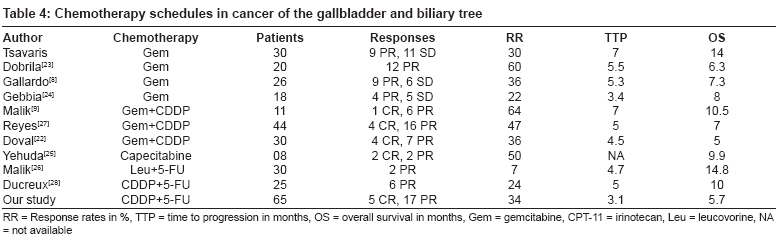
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 151-155 Original Article Infusion chemotherapy with cisplatinum and fluorouracil in the treatment of locally-advanced and metastatic gallbladder cancer Chatni SS, Sainani RS, Mehta SA, Mohandas KM Department of Digestive Diseases and Clinical Nutrition, Tata Memorial Hospital, Mumbai - 400 012, Maharashtra Code Number: cr08047 Abstract Background: Gallbladder cancer (GBC) has a poor prognosis. Chemotherapy is traditionally considered to be ineffective. The goal of the current study was to evaluate the efficacy of infusional 5-fluorouracil (5-FU) and cisplatinum (CDDP) in patients with inoperable GBC.Materials and Methods: A total of 65 patients with inoperable GBC received palliative chemotherapy with CDDP and 5-FU. All the patients had clinically measurable disease as well as adequate bone marrow, hepatic, and renal function. Response was assessed after three cycles of chemotherapy. Results: A total of 19 patients had locally advanced unresectable cancer and 46 patients had metastatic cancer. There were 39 females and 26 males, with a median age of 50 years. A total of 212 chemotherapy cycles were administered to the patients. Response evaluation after three cycles of chemotherapy revealed complete response in five patients [7.69%; 95% confidence interval (95% CI): 2.87-16.22], partial response in 17 patients (26.15%; 95% CI: 16.57-37.81), stabilization of disease in 9 patients (13.85%; 95% CI: 6.96-23.88), and progression in 21 patients (32.30%; 95% CI: 21.80-44.35). At 6 months 44.6% patients were alive and 18.5% patients were alive at 12 months. The median overall survival was 5.7 months and the median time to disease progression was 3.1 months. This chemotherapy combination was well tolerated. There were no chemotherapy-related deaths. Conclusions: Infusion chemotherapy with CDDP and 5-FU appears to have a fair amount of activity in patients of inoperable GBC, with acceptable toxicity. Tumor shrinkage following treatment with this regimen enabled surgical resection in two patients. We believe that this promising combination must be tested against gemcitabine-based combinations in patients with inoperable GBC. Keywords: Chemotherapy, cisplatinum, gallbladder, gemcitabine, metastatic, palliative Introduction Adenocarcinomas of the gallbladder and bile ducts (cholangiocarcinoma) have a poor prognosis. Gallbladder cancer (GBC) is one of the most common gastrointestinal malignancies seen in India. [1] The incidence in the Gangetic plains of northern India is 4.5 cases per 100,000 population in men and 10.1 cases per 100,000 in women. High incidence of this cancer has also been reported from Chile, Bolivia, Mexico, Israel, and Japan. In Chile, GBC is the leading cause of death from cancer among women.[2] Most patients with GBC have advanced disease at presentation due to a propensity of this malignancy for lymph node metastases; for direct invasion into the liver; and for seeding of the peritoneal cavity, biopsy tracts, and laparoscopic sites. [3],[4] The overall 5-year survival rate is less than 5%. [5],[6] The French Surgical Association survey of 724 patients reported a median survival of 3 months, with a 1-year survival of 14% and a 5-year survival of 5%. [5] Surveillance, epidemiology, and end results (SEER) data demonstrated an overall 5-year survival of 12.3% in 2330 patients. [4] It is generally believed that GBCs are resistant to chemotherapy. To date, chemotherapy has had limited impact on the natural history of this disease. Some progress been made in the treatment of advanced GBC by using gemcitabine-based chemotherapy. The histogenetic affinity between the pancreas and gallbladder might be helpful.Combination chemotherapy of gemcitabine with other agents, such as cisplatinum (CDDP), has shown tumor responses ranging from 9-64%, with acceptable toxicity. The overall median survival in these studies have ranged from 6.3 to 16 months.[7] Gallardo et al. treated 26 patients with advanced and metastatic GBC using weekly gemcitabine and had a response rate of 36% (95% CI: 17.1-57.9%). The median survival time was 30 weeks. [8] Malik et al. used the combination of gemcitabine and CDDP in advanced GBC with a 64% response rate. The median time to progression was 28 weeks and median overall survival was 42 weeks. [9] The combination of infusion 5-fluorouracil (5-FU) and CDDP has been used for the treatment of several cancers, such as that of the head and neck, esophagus, stomach, anal canal, and pancreas. [10],[11],[12],[13],[14] This combination is easy to use, affordable in developing countries, and has fair amount of activity in many epithelial cancers. Tumor response has been reported using infusion of CDDP and 5-FU in small series of biliary cancers in Japan. We offered this combination to those of our patients who were unable to afford gemcitabine-based chemotherapy. This study is a prospective audit of palliative chemotherapy using infusion CDDP and 5-FU in patients with advanced GBC. The objectives of the trial were to determine the response rate, time to disease progression, survival, and safety profile with this combination. Materials and Methods This study is a prospective observational audit of patients who were evaluated and treated at our center for GBC between January 2000 and October 2003. Consecutive patients with histologically confirmed, unresectable GBC who received infusion chemotherapy with CDDP and 5-FU were included in the study. They were offered infusion CDDP and 5-FU after obtaining informed consent. The inclusion criteria included chemonaive patients; presence of measurable disease; a southwest oncology group performance status of 0-2; adequate bone marrow function (total white blood cell count > 4,000/cm 3 , absolute neutrophil count > 1,500/ cm 3 , and platelet count > 100,000/ cm 3 ); adequate hepatic function (total bilirubin < 3.0 mg/dl and alanine transaminases and aspartate transaminases < 3 times the upper limit of institutional normal); and adequate renal function (creatinine < 1.5 mg/dl). All these patients were initially offered gemcitabine-based chemotherapy but were unable to take it due to financial reasons. All the chemotherapy cycles were given in the hospital after adequate hydration with saline and diuresis using mannitol; antiemetic medications were given as required. CDDP, 20 mg/m 2 , was infused intravenously for 1 h, followed by 5-FU, 650 mg/m 2 , as a 23 h infusion for 5 consecutive days of each cycle. Cycles were repeated every 28 days. Doses of both the drugs were reduced by 20% if the patient had grade 3-4 hematological or nonhematological toxicities. Chemotherapy was stopped for tumor progression, unacceptable toxicity, and on the patient′s request. Tumor response was assessed using response evaluation criteria in solid tumors, with computer tomography scans at baseline and after every three cycles. The primary measure of interest was the tumor objective response rate; the others were overall and progression-free survival, time to progression, and safety and tolerability of this treatment. Standard response criteria were used to determine objective tumor response. A complete response (CR) was defined as disappearance of all measurable tumors without the appearance of any new lesions. Partial response (PR) indicated a reduction of more than 50% in the sum of products of the greatest perpendicular dimensions of all measurable lesions, without the appearance of any new lesions. Stable disease (SD) indicated a reduction of less than 50% in the sum of products of the greatest perpendicular dimensions of all measurable lesions or an increase of less than 25% in the sum of products of the greatest perpendicular dimensions of all measurable lesions. Progressive disease (PD) was defined as an increase of more than 25% in the sum of products of the greatest perpendicular dimensions of all measurable lesions, the appearance of any new lesions, or worsening of evaluable disease. Survival was measured from the time of initiation of the therapy to death. Time to progression was defined as the time from the start of treatment to the date that PD was first observed. Common toxicity criteria, version 2.0, was used for evaluation of the toxicity. Statistical methods The objective of the current study was to collect all pertinent clinical information regarding patients with inoperable GBC who were treated with CDDP and 5-FU between January 2000 and October 2003. Analyses of overall survival and time to disease progression were conducted using SPSS 11.5 for Windows. The 95% confidence intervals (95% CI) for proportions of responders were calculated by way of large sample approximation. Survival curves were generated using the Kaplan-Meier method. Results Between January 2000 and October 2003 we evaluated 194 patients with GBC. [Table - 1] summarizes patient characteristics. Palliative infusion chemotherapy using CDDP and 5-FU was given to 65 patients. There were 39 women and 26 men, with a median age of 50 years (range: 30-76 years). Nineteen (32%) patients had locally advanced cancers that were not resectable. Forty-six (68%) patients had distant metastatic disease: liver (30), ascites (13), omentum (5), retroperitoneal lymph nodes (3), ovary (2), laparoscopy port site metastases (2), lung (1), spleen (1), and supraclavicular lymph node (1). Six patients underwent biliary drainage to relieve biliary obstruction prior to starting chemotherapy. Response evaluation after three cycles of chemotherapy revealed complete response in five patients (7.69%; 95% CI: 2.87-16.22), partial response in 17 patients (26.15 %; 95% CI: 16.57-37.81), stabilization of disease in nine patients (13.85%; 95%CI: 6.96-23.88), and disease progression in 21 patients (32.30%; 95% CI: 21.80-44.35) [Table - 2]. Following patient with metastatic disease and major response to chemotherapy was rendered free of disease surgically. Exploratory laparotomy was done for the above patient, when a gallbladder mass was seen with omental metastases and ascites. Biopsy of the omental mass and ascitic fluid cytology indicated adenocarcinoma. We decided to give infusional CDDP and 5-FU. A CT scan of abdomen and pelvis was done after three cycles of chemotherapy, which showed a distended gallbladder with an irregular wall and near complete resolution of ascites and omental metastases. As the patient had shown favorable response, chemotherapy was continued. After six cycles of chemotherapy a CT scan was done, which showed CR. A simple cholecystectomy was performed. A gynecologist did intraoperative assessment of the ovaries and uterus. On final histopathology of the specimen, moderately differentiated adenocarcinoma was seen, with tumor invasion of the muscularis propria. The patient was asymptomatic for 5 months, after which she developed a recurrence, with obstructive jaundice. Endoscopic retrograde cholangiopancreatography revealed a type-1 hilar block; a metallic biliary stent was placed, following which there was 50% reduction in pruritus. Another patient had port site metastases and ascites following laparoscopic cholecystectomy. He received infusional CDDP and 5-FU and had a CR. However, after 13 months he expired following an acute myocardial infarction. Of the 65 patients enrolled in the study, 52 patients were evaluable for toxicity [Table - 3]. The total number of cycles administered was 212 cycles and the median number of cycles was 3 (range: 0-9 cycles). Grade 3-4 toxicities were observed in 11 patients and included vomiting (eight patients), diarrhea (six patients), neutropenia (four patients), febrile neutropenia (two patients), renal failure (one patient), and myocarditis (one patient). Chemotherapy was stopped in one patient after one cycle due to severe toxicity. There were no treatment-related deaths. The overall median time to progression [Figure - 1] was 3.1 months (95% CI: 2.38-3.75). Overall median survival [Figure - 2] of all patients was 5.7 months (95% CI: 3.59-7.88), with 44.6% and 18.5% of patients alive at 6 months and 12 months, respectively. Discussion There is no current standard chemotherapy in advanced biliary cancer. Oncology practices vary considerably and range from not offering patients chemotherapy because of concern over lack of efficacy and detrimental toxicity to offering patients multiple-drug regimens. Clinical trials in cholangiocarcinoma and GBC have suffered from the relative rarity of these tumors and the generally morbid condition of the patients at presentation. Our study of 65 patients is probably the largest study in which inoperable GBCs were treated with a uniform chemotherapeutic regime. This study produced promising results, including a response rate of 33.9% (95% CI: 23.15-45.95%) and a 1-year survival of 18.5%. With an additional 13.8% patients experiencing stable disease, chemotherapy resulted in abrogation of progression in 47.7% of the patients. All of the 65 patients were considered for evaluation. Patients who were lost to follow-up were considered to have expired and the date of the last follow-up visit was taken as the date of death. Treatment-related toxicity was mild and was not radically different from the toxicities observed in other studies. Tumor shrinkage enabled surgical resection in two patients. The majority of patients (more than 75%) with GBC present with locally advanced or metastatic cancer where surgery is not possible and prognosis is dismal. Radical or extended cholecystectomy is potentially curative and possible in less than 30% of patients. There are few reports on the role of cytoreductive R+ resection in GBC. Summary of the various chemotherapy schedules in cancer of the gallbladder and biliary tree have been enumerated in [Table - 4]. It is generally believed that GBCs are chemoresistant. [15] There is no standard-of-care chemotherapy. Several studies have tested single-agent and combination chemotherapy in gallbladder or bile duct cancers. Monochemotherapy yielded disappointing results, with objective response rates ranging from 5 to 20%. The most extensively used drug is 5-FU and it has been combined with various other drugs with varying results. For single-agent systemic chemotherapy, objective response rates were 10% for mitomycin C [16] and 11% for 5-FU. [17] The response rates for 5-FU-based combination systemic chemotherapy were 5% for 5-FU plus lomustine; [17] 31% for FAM [18] (5-FU, adriamycin, and mitomycin C); and 26% for 5-FU plus leucovorine. [19] More recently gemcitabine alone or in combination has been used in the treatment of advanced GBC with response rates varying from 20 to 40%. Gemcitabine is expensive and not affordable by most Indian patients. CDDP- and 5-FU-based chemotherapy have been used in the treatment of various malignancies, for example, cancers of the anal canal, breast, cervix, esophagus, stomach, and nasopharynx. Mishra et al. used various combination chemotherapy regimens in the treatment of advanced GBC. [20] The response rates with various regimens were as follows: 34% with intra-arterial 5-FU plus mitomycin C ( n = 26; PR 8); 25% with intravenous 5-FU plus mitomycin C ( n = 28; CR 1, PR 6); 30% with 5-FU, mitomycin C, and leucovorine ( n = 23; PR 7); 38% with CDDP and 5-FU ( n = 21; PR 8); 10% with paclitaxel and 5-FU ( n = 10; PR 1); and 61% with gemitabine and CDDP ( n = 11; CR 1, PR 10). In a study in which 30 patients of advanced GBC were treated with 5-FU, leucovorine, and hydroxyurea, nine had partial response. The median duration of response was 6.5 months and median survival was 8 months. A regional therapy has been examined using intra-arterial mitomycin C, and a 48% response rate and median survival of 5 months (as compared to 14 months in untreated controls) was recorded. [21] Doval et al. treated chemotherapy-naοve, unresectable GBC with gemcitabine and cisplatinum. [22] They achieved a response rate of 36.6% (95% CI: 34-40%) in 30 evaluable patients, with a median time to progression of 18 weeks (95% CI: 14-24 weeks), overall survival of 20 weeks (95% CI: 14-31 weeks), and 1-year survival of 18.6%. In our study one patient with locoregional disease and complete response after three cycles of chemotherapy underwent surgical resection. Thereafter she was treated with chemoradiotherapy and, after a 48-month follow-up, she remains disease free. In summary, our study reveals that infusional chemotherapy with CDDP and 5-FU is a useful therapy for patients with advanced unresectable GBC and has manageable chemotoxicity. Following good response two patients could undergo curative resection. We believe that this combination must be tested in a randomized trial against gemcitabine-based chemotherapy. [28] References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08047t2.jpg] [cr08047f1.jpg] [cr08047t3.jpg] [cr08047t1.jpg] [cr08047t4.jpg] [cr08047f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}