 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
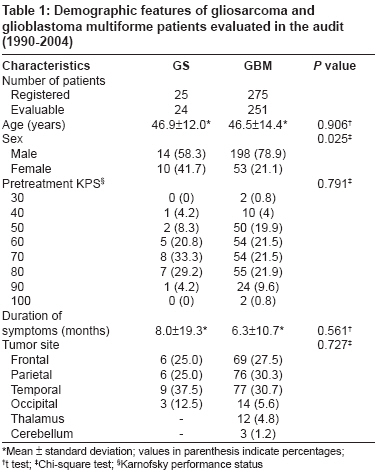
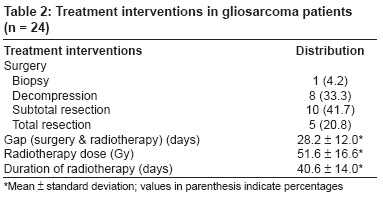
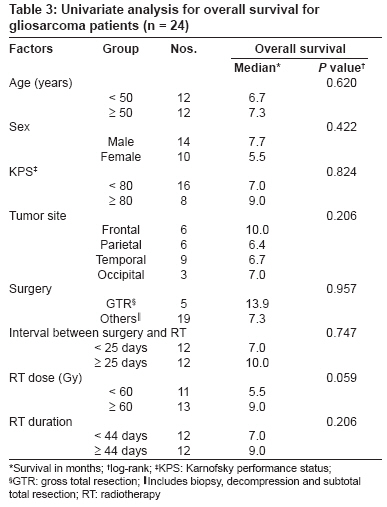
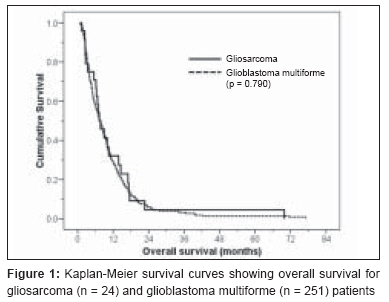
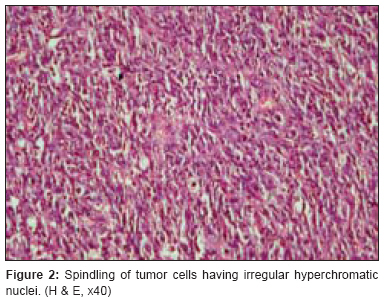
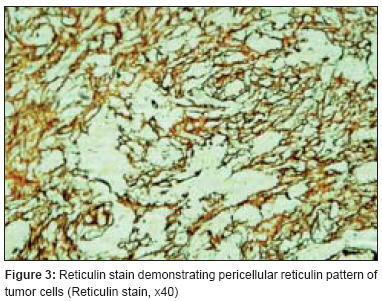
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 164-168 Original Article Gliosarcoma: An audit from a single institution in India of 24 post-irradiated cases over 15 years Kumar Piyush, Singh Shalini, Kumar Pavan, Krishnani Narendra, Datta Niloy R Department of Radiotherapy, Regional Cancer Centre, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow- 226 014, U.P Code Number: cr08049 Abstract Background: Gliosarcomas (GS) are biphasic brain tumors composed of glioblastoma multiforme (GBM) and sarcomatous component. Therapeutic approaches include maximum surgical decompression with postoperative radiotherapy. Outcomes in gliosarcoma are poor despite multimodality management.Aims: To analyze the outcome in patients of GS treated in our institute over a period of 15 years and compare it with GBM treated during the same period. Settings and Design: Clinical records of the post-irradiated GS patients and GBM patients seen between 1990 and 2004 were retrieved. Materials and Methods: Demographic and treatment variables were evaluated for their influence on overall survival (OS). The survival outcomes of GBM and GS treated during the same period were also compared. Statistical Analysis: Univariate analysis was carried out using the Kaplan-Meier method and tested using log-rank test for significance. Results: During these 15 years, 24 evaluable GS patients were treated as compared to 251 evaluable patients of GBM. There was a slight male preponderance in GS (14 males vs.10 females) with a median age of 50 years. All patients underwent surgery followed by post-operative radiotherapy (median dose of 60 Gy). None of the patient or treatment related factors were found to be significantly influencing their OS. Median OS in GS was 7.3 months compared to 7.5 months in GBM patients (P = 0.790). Conclusions: The OS appears to be similar for GS and GBM. None of the demographic variables appeared to prognosticate the survivals of GS. Keywords: Glioblastoma multiforme, gliosarcoma, radiotherapy, survival Introduction Gliosarcomas (GS) are biphasic brain tumors composed of glioblastoma multiforme (GBM) and sarcomatous component, and were first described in 1895 by Heinrich Stroebe. [1] The mesenchymal component typically resembles fibrosarcoma, but differentiation patterns resembling osteosarcoma, chondrosarcoma, angiosarcoma and rhabdomyosarcoma have also been described. [2] It is a rare cerebral tumor that has been classified as a separate clinico-pathological entity, even though it remains closely related to GBM. [3],[4] Gliosarcomas account for 8% of all GBM. [5] Therapeutic approaches include maximum surgical decompression with post-operative radiotherapy (RT) although prognosis continues to be poor despite these interventions. This audit has been carried out to analyze the clinical features and survival outcomes in GS patients seen over a period of 15 years and to compare their demographic features and outcomes with GBM patients treated during the same period . Materials and Methods Between January 1990 and December 2004, 1,236 patients of brain tumors were registered in the Department of Radiotherapy at our Institute. Of these, there were 25 histopathological confirmed patients of GS and 275 cases of GBM. Of the 25 patients of GS, one patient did not turn up for post-operative RT and was excluded from the analysis. Thus, the remaining 24 GS patients who received RT were considered for this audit. Of the 275 patients of GBM, 24 did not report for any adjuvant treatment after registration and hence were excluded from the analysis. The remaining 251 evaluable GBM who received RT were considered for a survival outcome comparison with GS patients of this audit. The status of all these patients on or before 1 st July 2007 was extracted from the individual treatment records. Both patient and treatment related variables already documented in the clinical files of the patients were evaluated. The patient related parameters included age, sex, duration of symptoms, tumor site and pre-radiotherapy Karnofsky performance status (KPS). Treatment related parameters examined included extent of surgical resection, interval between surgery and start of RT, and overall treatment time for RT. Total resection of the tumor was considered if 90% or more of the tumor was resected as recorded in neurosurgical operative records. The target delineation was based on contrast enhanced computed tomography (CECT) or magnetic resonance imaging (MRI) or both. CT scan was used in the initial years and in later years MRI was also used. Radiotherapy was usually delivered in two phases; phase I for clinical target volume, consisting of the volume encompassing the peri-tumoral edema as seen on CECT or the hyper-intense T2W image. For the phase II treatment, the contrast enhancing regions depicting the mass effect on CECT or T1W contrast images constituted the gross target volume. All patients were subjected to RT simulation and dose distributions were evaluated on treatment planning systems (Radplan, ASHA- 3-D, M/s TSG Integrations, India and ISIS-3D, Technologie Diffusion, France). Patients were treated on telecobalt or 6 MV / 10 MV photon beams or their combinations. A majority of patients were scheduled to receive a dose of 40-45 Gy in phase I and 15-20 Gy in phase II, delivered at a dose per fraction of 180-200 cGy over a period of 6 to 7 weeks. Three patients were scheduled RT for a dose more than 60 Gy under a study protocol, two of whom received 70 Gy by altered fractionation and one received 66 Gy by standard fractionation schedule. One patient was treated with the hypofractionated protocol with a total dose of 35 Gy. Statistical analysis Demographic features between GS and GBM patients were compared using either chi-square test (for discrete variables) or t-test (for continuous variables). For OS, death from any cause was considered as an event. The end point was computed from the date of surgery. For patients not reporting for follow up, every possible effort was made to ascertain their status by postal or telephonic communication. The analysis was carried out as "worst case scenario" wherein the patients lost to follow up were considered as an event. Univariate analysis was carried out using the Kaplan-Meier method and tested using log-rank test for significance. [6] Cut-off points for univariate analysis of continuous variables were based on median values of their distribution. Results Patient demography The demographic features of the 251 GBM patients are summarized in [Table - 1]. Median age was 48 years with a male predominance (male: female: 3.7:1). Most of them had KPS in the range of 50 to 80 and only 26 patients (10%) had a KPS of at least 90 or more. All patients had surgical interventions, before being referred for adjuvant therapy. Treatment related parameters for GS have been detailed in [Table - 2]. All patients had surgical interventions; a majority underwent subtotal resection, before being referred for post-operative RT. The surgical descriptions were entered as per the neurosurgical records. RT was usually started within 3 to 4 weeks (median - 24 days) of surgery and a median dose of 60 Gy was delivered. In GBM, post-operative RT commenced within 3 to 4 weeks (median - 26 days) of surgery, and a dose of 60 Gy was received by 151 patients (60.2%), while 59 (23.5%) patients received less than 60 Gy and 41 (16.3%) received doses more than 60 Gy to a maximum of 73 Gy. The minimum and median RT doses for patients who received less than 60 Gy were 12.6 Gy and 55 Gy respectively, while the median dose for those who received more than 60 Gy was 60 Gy. Chemotherapy either in the form of a single agent CCNU (lomustine) or a combination protocol of PCV (procarbazine, lomustine and vincristine) for a maximum of six cycles was prescribed in 108 (43%) patients, which was based upon the discretion of different clinicians. Survival analysis On univariate analysis, none of the patient or treatment related factors were found to be statistically significantly influencing the OS, although the subgroup of patients who had received the total RT dose of 60 Gy or more had a better outcome (median survival < 60 Gy vs. > 60 Gy was 5.5 vs. 9 months, ( P = 0.059) [Table - 3]. There was a definite impact of this chemotherapy in terms of overall survival in our cohort of GBM patients. The overall survival in the group of patients receiving chemotherapy and not receiving chemotherapy was 9.8 and 5.4 months respectively, which was statistically significant ( P = 0.005). Median OS for the entire cohort of GS patients was 7.3 months. Overall survival for GS at 1 year, 2 years and 5 years were 32.0%, 4.6% and 4.6% respectively. In GBM patients, the median OS was 7.5 months and the OS at 1, 2 and 5 years were 29%, 6.8% and 1.7% respectively. There was no significant difference in the OS between GS and GBM patients (log-rank, P = 0.790) [Figure - 1]. Toxicity Discussion Gliosarcoma is a rare malignant brain tumor with mixed morphological features of both GBM and sarcoma. The incidence reported in various series ranged from 2% to 8% of all GBM, [3],[4] which is almost similar to 8.7% in our audit. Therapeutic irradiations given for GBM influence sarcomatous transformation. [7],[8] However, in our series all the cases were primary GSs and none was secondary to GBM. The usual age of presentation is in fifth to seventh decade. [9],[10],[11] Data published by Meis et al . [3] and Galanis et al. [12] showed that the median age of presentation in their series was 60 years while in our study, the median age was 48 years (range: 20 to 65 years). Gliosarcoma is usually not frequent in children, although it has been reported in the literature. [13],[14] Gliosarcoma affects more males than female, which can be clearly seen in our series also ([Table - 1]; 58.3% vs. 41.7%). These are usually located in the cerebrum, involving the temporal, parietal, frontal, and occipital lobes in decreasing order of frequency.[4],[12] In our series, 37.5% had involvement of temporal lobes, compared to more than 50% reported by Morantz et al . [4] and Sarkar et al . [14] We did not encounter cases with any systemic metastasis, although unusual cases with spread to lung, bone and lymph nodes have been reported in the literature. [9],[15],[16],[17],[18] Histopathologically, GS is a bimorphic tumor composed of two distinct malignant cell populations. First, gliomatous component identified as astrocytes with endothelial proliferation and necrosis, and the other sarcomatous component, which is of mesenchymal nature and generally spindled [Figure - 2]. Reticulin stains [Figure - 3] and immunostains for glial fibrillary acidic protein are performed to distinguish the glial from the sarcomatous components of the tumor. The demographic profiles of our patients of GS and GBM were nearly similar for age at presentation ( P = 0.906), pretreatment KPS ( P = 0.791), duration of symptoms ( P = 0.561) and site of tumor ( P = 0.727). However, a higher preponderance in GBM in males was observed compared to those in GS (GBM: male vs. females: 78.9% vs. 21.1%; GS: male vs. females: 57.7% vs. 42.3%, P = 0.025) [Table - 1]. Most of our patients were given RT in the conventional fractionation (except 3 patients in altered fractionated schedules) with a median dose of 60 Gy. In other reported series, the RT dose ranged from 40-81 Gy with different fractionational schedules. [3],[4],[12],[14],[19] None of our patients had received chemotherapy since there is no strong evidence of its benefit. In a study of 24 patients by Morantz et al ., [4] where the average survival for all the patients was 21 weeks, a slight increase in survival was observed with the addition of chemotherapy (36 weeks) in 9 patients compared with RT alone (33 weeks) in 15 patients. Chemotherapy was used as an adjunct to RT in various forms - mithramycin (5 patients), BCNU (2 patients), adriamycin (1 patient) and intracarotid amethopterin (1 patient). Meis et al . [3] found that none of the treatment regimens, which included various combinations of radiation therapy and chemotherapy (BCNU, dacarbazine, semustine, misonidazole), improved survival of GS over GBM; median survival being 8.3 months vs. 9.6 months respectively. In another study by Galanis et al ., [12] 18 patients of GS were derived from a series of 748 grade 4 astrocytoma cases that were part of four consecutive randomized phase III trials and were treated with external radiation and nitrosurea-based chemotherapy (carmustine, PCNU and dibromodulcitol). The median survival reported was 35.1 weeks and 41.6 weeks for GS and GBM respectively, which was not statistically significant ( P = 0.27). The reported median survival in GS varied from 6.2 to 11.5 months. [11],[12],[19] In our group of patients, it was 7.3 months, which is relatively lower. Unlike GBM, in our audit of gliosarcoma patients, no prognostic factors affecting survival were seen. In a study of 11 patients by Salvati et al. , [20] age and KPS did not have any impact on the overall survival, as is also seen in our study, but the histopathological and radiological findings did have an effect. Patients with radiological features of meningioma and those with predominant sarcomatous features on histopathology, had significantly better survivals than those with GBM features or gliomatous component (62 weeks versus 53.5 weeks; P = 0.04). In some studies, young age and pre-treatment Karnofsky performance status > 70 have been shown to be associated with higher survival probability. [11],[19] The possible attributes for a lower survival in our patients could be poor KPS at the time of presentation (only 33.3% had KPS 80 or more), larger tumor dimensions restricting total tumor excision (feasible only in 20.8%) and inability to complete at least 60 Gy of postoperative RT (45.5% patients received less than 60 Gy). All these variables could have influenced treatment outcomes. Comparing with the 251 evaluable patients of GBM, it was observed that median OS of GS did not differ significantly from GBM. The overall survivals, of 7.3 with GS and 7.5 months in GBM were similar ( P = 0.790) [Figure - 1]. This has also been observed by Meis et al. [3] with median survivals of 8.3 and 9.6 months in their GS and GBM patients respectively. Survival outcomes in GS and GBM thus appear to be identical. The audit demonstrates that patients of GS and GBM appear to have similar clinical features and outcomes. Gliosarcoma may therefore be treated on the same lines as GBM, with maximal surgical decompression followed by post-operative RT. The possible role of chemotherapy in GS is still undefined and could be explored in future studies. References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08049t3.jpg] [cr08049t1.jpg] [cr08049f2.jpg] [cr08049f3.jpg] [cr08049f1.jpg] [cr08049t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}