 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
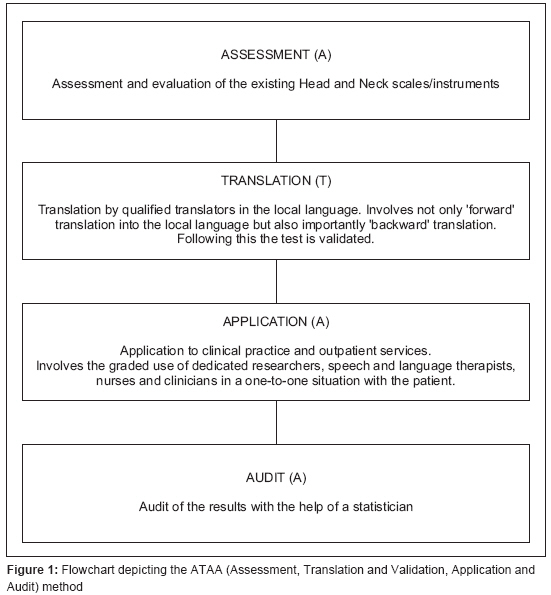
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 192-194 Brief Communication Need for a paradigm for application of outcome measure (QOL scales) in head and neck cancer patients in India Sayed SuhailI, Kazi RehanA ENT and Head-Neck Surgery, Grant Medical College and J. J. Group of Hospitals, Byculla, Mumbai-400 008 Code Number: cr08054 Abstract Quality of life (QOL) is a multidimensional construct that minimally includes broadly defined assessments of the physical, psychological, and social domains of functioning. However, measuring this QOL is complicated by the fact that there are many different validated questionnaires available. In India, with people now wanting self-directed care and greater autonomy, we must direct increased efforts towards QOL and its assessment. We propose the Assessment, Translation & Validation, Application and Audit method to increase the use of QOL scales in our country.Keywords: Head-neck cancers, instruments, outcome measurement, quality of life, scales Quality of life (QOL) is a multidimensional construct that minimally includes broadly defined assessments of the physical, psychological, and social domains of functioning. [1] When determining treatment for head and neck cancer, different therapeutic options may provide a similar prognosis or chance of cure, but with very different quality of life (QOL) outcomes. The evaluation of QOL and performance outcome in HNC is critical to optimal patient care, comprehensive evaluation of treatment alternatives, and the development of informed rehabilitative services and patient education. However, measuring this QOL is complicated by the fact that there are many different validated questionnaires available. [2] In addition, QOL is an individual perception that can be affected by health status, as well as by disease. When quantifying QOL, we must consider the influence of numerous factors and their potential interdependence if accurate representations of QOL status are to be gathered. [3] Outcome measurement using validated questionnaires and research have been a topic of discussion among the medical fraternity, the government, and insuring agencies in the West for past many years. In the case of laryngeal cancer, results from the use of QOL scales highlight the fact that although treatment of the cancer is successful, individuals continue to experience difficulties in daily activities and social participation, regardless of the type of treatment (i.e. radiation therapy, conservative or radical surgery, chemotherapy, or a combined treatment protocol). [4],[5],[6] There is evidence that with time patients adjust and learn to cope with the disease and treatment sequelae. [3],[5],[6],[7],[8],[12] QOL outcome measurement is, largely, subjective and highly individualized. [9] In India, with people now wanting self-directed care and greater autonomy, we must direct increased efforts towards QOL and its assessment. We propose the Assessment, Translation & Validation, Application and Audit (ATAA) method to increase the use of QOL scales in our country [Figure - 1]. For far too long, we have neglected this important domain citing an over-burden on our healthcare infrastructure. However, if we want to move forward, we must incorporate this model. Stage 1 of this paradigm includes a rigorous assessment (A) and evaluation of the existing head, neck QOL scales/instruments. In the literature, as many as 20 health-related outcome measurements have been described. Most questionnaires involve the judicious combination of disease, treatment and site along with generic measures to assess the QOL. These scales can be classified as: general head, neck QOL scales like the EORTC H & N 35, UWQOL v4, HNQOLQ, FACT-H&N v4, HNCI and symptom-specific ones like the MDADI, LASA and DSHNC. [10],[11],[12],[13],[14],[15],[16],[17],[18],[19] It is easy to get confused with the semantics of all these scales but it is imperative to check their quality and content prior to use. All existing scales vary widely in respect of their development and validation and information to this end must be gathered. Once an appropriate scale is identified and selected, stage 2 is the translation (T) by qualified translators to the local language. This is a lengthy process that involves not only ′forward′ translation into the local language but also importantly ′backward′ translation. This is crucial to ensure that final scale/questionnaire compares favorably to the original English version not only in the translation but logically as in the nuances of the meaning. Following translation, the scale must be then validated in a study that assesses both the reliability (internal consistency and test-retest) and validity (content, construct and criterion) domains. The third stage is that of application (A) to clinical practice and outpatient services. This should involve the graded use of dedicated researchers, speech and language therapists, nurses and clinicians in a one-to-one situation with the patient. Although this is not the ideal way and the self-administered route is best, the prevailing low literacy may make the self-administered approach challenging. But this problem can be solved by using methods like reading out questions verbatim to the patient and noting down the response. This procedure will require training those who will be assisting patients with questionnaire completion very carefully to avoid biasing results. To aid us in patient evaluation, validated instruments like EORTC and FACT are available in regional languages viz. Hindi and Marathi. [20] The last stage (4) of the exercise involves an honest and independent audit (A) of the results with the help of a statistician. Only then can we elucidate meaningful directions for future research and clinical care for our patients. Finally, mention has to be made of longitudinal data (follow-up) of the patients, which may prove to be a daunting task. But the principle of the patient acting as their own control, over time, collecting their own history pertaining to symptoms/complications is a critical point. The use of such a role-model/paradigm with due emphasis at every stage will ensure that valid and reliable data is collected to bridge the gap between treatment and QOL outcomes in this country. References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08054f1.jpg] |
| |||||||||


{kind=link}