 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
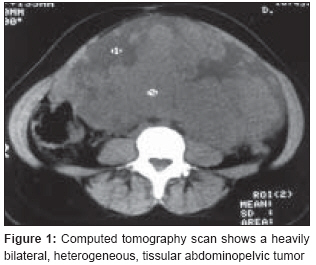
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 195-196 Case Report Primary lymphoma of the ovary Elharroudi Tijani, Ismaili Nabil, Errihani Hassan, Jalil Abdelouahed Department of Medical Oncology, National Institute of Oncology, Rabat Code Number: cr08055 Abstract Involvement of the ovary by malignant lymphoma is a well-known late manifestation of disseminated nodal disease. Primary ovarian lymphoma is rare. We report a case of primary ovarian non-Hodgkin's lymphoma with bilateral involvement which was managed by surgery and chemotherapy. A 29-year-old woman was admitted with signs and symptoms suggestive of an ovarian cancer. Computed tomography revealed an abdominal tumor measuring 20 cm in diameter, without enlarged lymph nodes. The diagnosis of malignant lymphoma was established after bilateral adnexectomy and histological study of the excised tissue. The tumor was classified as a diffuse large B-cell lymphoma. The patient has been advised 8 cycles of standard CHOP regimen and is presently on treatment. She has now been without disease for 7 months after the surgery. According to previous reports the treatment principles and prognosis of primary ovarian lymphoma is the same as that of other nodal lymphomas.Keywords: Lymphoma, ovary, primary Introduction Involvement of the ovary by malignant lymphoma is well known as a late manifestation of disseminated nodal disease, almost always of the non-Hodgkin′s type. But primary ovarian lymphomas are unusual. [1] Primary ovarian non-Hodgkin′s lymphoma accounts for 0.5% of all non-Hodgkin′s lymphomas and 1.5% of all ovarian neoplasms. [2] We present a case of ovarian non-Hodgkin′s lymphoma, manifesting like ovarian cancer, which was managed by surgery and chemotherapy.Case Report A 29-year-old woman (gravida 2, para 2) was admitted to our hospital with increasing abdominal volume, weight loss (12 kg), and extreme fatigue for 4 months. A physical examination revealed a mobile abdominopelvic mass reaching up to the epigastrium, mobile with regard to the deep and superficial plans. The pelvic exam and digital rectal examination were normal. The ganglionic areas were free from the disease. Computed tomography (CT) scan showed a heavily bilateral heterogeneous tissular abdominopelvic tumor, the largest one measuring 20 x 12 cm in diameter; there were no enlarged lymph nodes [Figure - 1]. The serum tumor markers were positive, with CA-125 being 252 U/ml (normal < 25 U/ml). The erythrocyte sedimentation rate was increased, being 85 mm in the first hour and 105 mm in the second hour. An exploratory laparotomy was done through a large abdominal vertical midline incision so as to establish the diagnosis. Laparotomy revealed a left ovarian tumor measuring 28 x 11 cm in diameter [Figure - 2] and a right ovarian mass measuring 7 cm, which was coarse, tissular, and without extracystic vegetations or ascetic fluid accumulation; there were no peritoneal implants, hepatic metastases, or adenomegaly. A bilateral adnexectomy with omentectomy, appendectomy, peritoneal cytology, and peritoneal biopsy were performed. The extemporaneous studyof the left ovarian tumor was not decisive. The histological study and immunohistochemistry were suggestive of a large B-cell non-Hodgkin′s lymphoma in both the ovaries. Most of the neoplastic cells were positive for CD-20 and for leucocyte common antigen (LCA) antibody. Peritoneal cytology was positive. The rest of prelevements was negative. After surgery, CT of the chest, abdomen, and pelvis was normal and serum CA-125 was also normal. A bone marrow biopsy showed no abnormalities. The patient was staged IIE according to the Ann Arbor staging system. The patient was prescribed eight cycles of the standard CHOP regimen (cyclophosphamide 750 mg/m² d1, doxorubicin 50 mg/m² d1, vincristine 1.4 mg/m² d1, and prednisone 50 mg/m² d1-5); she has completed six cycles and, 7 months after surgery, she remains disease free.Discussion Lymphoma is a rare tumor of the ovary and its presence most commonly represents involvement in overt systemic disease, almost always of the non-Hodgkin′s type. [1] The diffuse, large B-cell lymphoma appears to be the most common type of primary ovarian non-Hodgkin′s lymphoma. [2] There has been debate as to whether lymphoma can arise de novo in the ovary; lymphoid aggregates do exist in normal ovarian tissue, which could give rise to such lesions. [3] The majority of primary ovarian lymphomas present with pelvic complaints; some cases present with ascites and elevated serum CA-125. [4],[5] Our patient presented with a pelvic mass and elevated serum CA-125. The bilateral ovarian involvement, peritoneal implants, and omental involvement at the time of surgery may argue against a primary ovarian disease. [6] Our patient presented with bilateral ovarian involvement and positive peritoneal cytology. The presence of positive staining for leukocyte common antigen (LCA) in the histological specimen distinguishes malignant lymphoma from nonlymphoid neoplasm. [7] Diffuse, large B-cell lymphomas were positive for CD20 and BCL-6 and or CD-10 and or BCL-2. [5] CT is the mainstay of lymphoma staging in the chest, abdomen, and pelvis as well as in other nodal lymphomas. Bone marrow biopsy is also mandatory for staging. Positron emission tomography (PET) with 18 F-fluorodeoxyglucose (FDG) has been reported as being a useful method for staging and for assessment of therapeutic response. [8] Patients with disease localized to one ovary usually do well with unilateral surgical resection followed by systemic chemotherapy. [1] The use of chemotherapy is based on the principle that ovarian lymphoma must be considered a localized manifestation of systemic disease. [9] The prognosis for such patients is much better than that of patients with obvious systemic disease. [1] In primary ovarian lymphoma stages I-II, a conservative management based on exclusive chemotherapy may be attempted in selected patients desiring pregnancy. [10] The protocol of chemotherapy used in diffuse, large B-cell histology is the standard CHOP regimen. [2] Our patient was treated with bilateral adnexectomy, omentectomy, and appendectomy followed by eight cycles of CHOP. The outcome of these patients, treated with appropriate chemotherapy, appears to be similar to that of patients with other nodal non-Hodgkin′s lymphomas. [2] Conclusion Primary lymphoma of the ovary is rare. Its must be considered as a localized manifestation of systemic disease. According to the previous reports in literature, the treatment principles and the prognosis are the same as that of other nodal lymphomas.Acknowledgment Mohammed Ismaili.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08055f2.jpg] [cr08055f1.jpg] |
| |||||||||

{kind=link}
{kind=link}