 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
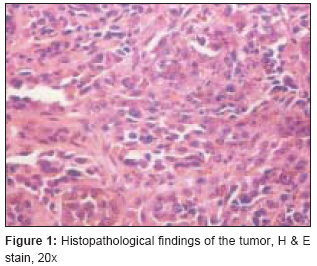
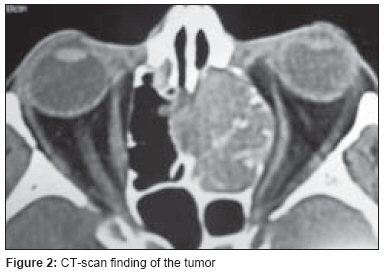
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 200-202 Case Report Mucosal melanoma of nasal cavity and paranasal sinus Dwivedi Raghav, Dwivedi Ravi, Kazi Rehan, Kumar Sumit, Agarwal SatyaP Head-Neck Unit, Royal Marsden Hospital, Fulham Road, London, U.K; King George's Medical University, Lucknow, India Code Number: cr08057 Abstract Mucosal melanoma of the nasal cavity and paranasal sinuses is seldom encountered in routine ENT practice. These tumors have poor prognosis owing to higher rates of locoregional recurrence and distant metastasis. Various treatment modalities have been employed over time but the ideal treatment approach still remains an open issue. This article presents some commonly accepted guidelines in treating these rare mucosal neoplasms.Keywords: Epistaxis, mucosal melanoma, paranasal sinus Introduction Melanomas are tumors arising from melanocytes, which are neuroectodermal-derived cells located in the basal layers of the skin, skin adnexa, and some mucosal membranes. Common sites for melanomas are the head, neck, and lower extremities as these are areas exposed to sunlight, which is one of the predisposing factors. Less common sites of involvement are oral and genital mucosa, nail beds, conjunctiva, orbit, esophagus, nasal mucosa or nasopharynx, vagina, and the leptomeninges. Melanomas arising in the nasal cavity or paranasal sinus are rare and have a poor prognosis. [1] Primary melanoma of the head/neck accounts for 25-30% of all melanomas. [2] However, the incidence of melanomas arising from the mucosal surface of the aerodigestive tract varies from 0.4 to 4%, the majority arising in the nasal cavity or paranasal sinuses. [3],[4] The nasal cavity is more commonly affected than the paranasal sinuses, and the maxillary antrum is more frequently involved than the ethmoid sinuses. The peak incidence is between the fifth and eighth decade, and it is seen slightly more commonly in males than in females; age and sex do not affect the prognosis. [5],[6] Case Report A 58-year-old gentleman presented in the emergency department with massive epistaxis. The patient′s history revealed recurrent episodes of nasal bleeding for the past 3 months. He also complained of progressively increasing nasal obstruction on the left side since 2 months. A few days later, when the patient′s condition had settled, diagnostic nasal endoscopy was performed; this revealed a pink, smooth mass in the left nasal cavity, filling the whole middle meatus and extending up to the choana. Nasal endoscopy on the right side was within normal limits. Biopsy was taken in the same sitting and sent for histopathological examination, which gave a conclusive diagnosis of malignant melanoma [Figure - 1]. CT scan of the paranasal sinuses confirmed the finding of a localized mass in the right nasal cavity, involving the left anterior and posterior ethmoid sinuses and also blocking the infundibulum of the maxillary antrum [Figure - 2]. There was a mass effect on the left orbit pushing the medial wall. However, there was no evidence of direct orbital involvement. Superiorly, the mass extended up to the cribriform plate, raising the possibility of its erosion at some places; however, the patient did not have any complaints of altered smell or any signs of meningeal irritation. There was no involvement of the sphenoid sinuses, regional lymph nodes, or any distant organ. There was no erosion of the nasal septum and the disease was limited to the left side. Metastatic workup was within normal limits. The patient opted for medical management over surgical, and was referred to the department of radiation oncology for further management.Discussion Among the cancers that arise in nasal cavity and paranasal sinuses, mucosal melanomas are rare in comparison to squamous cell carcinomas. The presentation depends on the size and site of the lesion. The majority of the patients present with epistaxis and progressively increasing nasal obstruction.[1] At initial presentation these tumors are fairly advanced, due to the ample space available to accommodate their growth and the obscure anatomy of the sinuses. The natural course of malignant melanomas is marked by early local recurrences, extensions, and frequent metastasis to lymph nodes and viscera, making it one of the most dangerous forms of nasal and paranasal sinus tumors. The incidence of regional lymph node metastasis on admission is approximately 5-15%. [7] The submandibular lymph nodes are most commonly involved. A high index of suspicion is required to make an early diagnosis. Generally, ENT surgeons do not have problems in diagnosing and staging this disease, but owing to its rarity there remains some disagreement regarding proper treatment. In general, the management of mucosal melanomas has not been uniform. The only definitive prognostic factor is the presence of distant metastasis at the time of diagnosis. As a rule, patients with localized disease should undergo surgery followed by postoperative radiotherapy for better local control of the disease, unless the patient is unwilling to undergo surgery, as in the present case. Historically, mucosal melanoma was characterized as a radioresistant disease, but recent observations suggest that radiotherapy has a significant role in their treatment. Literature shows overall initial response rate of 50-75% if radiotherapy alone is used for treating localized mucosal melanomas; however, long-term survival remains a big issue. [8],[9] So far, surgery has been the mainstay of the treatment of these tumors, provided they are resectable. Surgery, along with adjuvant radiotherapy, should be used for patients with either regional metastases or large bulky primary disease (with or without positive neck nodes). Prophylactic neck irradiation should be used in such cases. Patients with unresectable local disease or those who do not agree for surgery should be considered for radiotherapy alone as a definitive management, whereas chemotherapy should be reserved for patients with systemic disease. Bonner et al. have demonstrated the usefulness of concomitant chemoradiotherapy in squamous cell carcinomas of the head and neck region, indicating the possible role of primary concomitant chemoradiation in mucosal melanomas as well. [10] Chemotherapy may have some role to play in the postoperative period also. A number of questions and controversies still remain. To conclude, at present the most accepted treatment of malignant melanoma is surgery and post operative radiotherapy. Mucosal melanomas tend to be more aggressive and have a poorer prognosis than the cutaneous ones, with affected patients having only 10-15% 5-year survival rates. [11],[12] The poor prognosis may be attributed to local recurrence, distant metastasis, and/or a second primary. Hence the importance of life-time surveillance and patient education; monthly self-examination of skin and regional lymph nodes for A (asymmetry), B (border), C (color), and D (diameter) of melanoma surveillance should not be overlooked. Several new biologic and immunomodulatory treatments are currently being investigated for use in patients with mucosal melanoma. OK-432, interleukin 2, lymphokine-activated killer cells, and bacille Calmette-Guerin (BCG) vaccine have met with partial success and require further trials with large cohorts. Newer radiotherapy modalities like intensity-modulated radiotherapy (IMRT) and three-dimensional conformal radiotherapy (3-D-CRT) etc. are being investigated and show some promise for use in treating these tumors in the future. Acknowledgment The authors would like to thank Dr Namita Kanwar for her contribution in the preparation of the manuscript.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08057f2.jpg] [cr08057f1.jpg] |
| |||||||||

{kind=link}
{kind=link}