 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
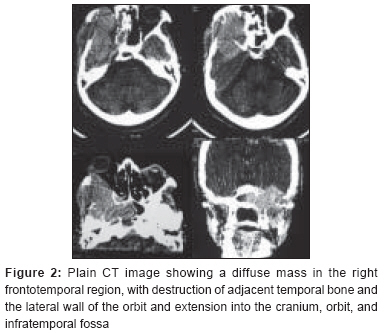
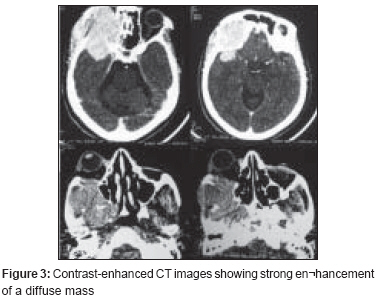
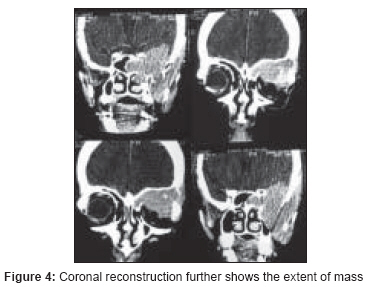
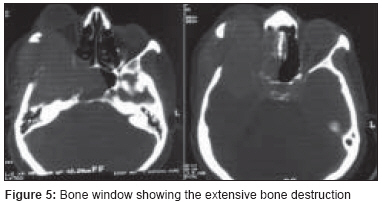
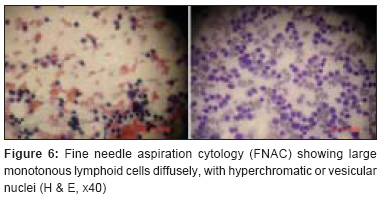
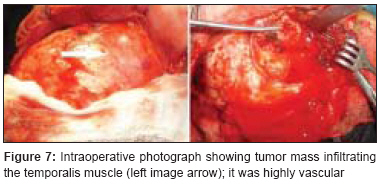
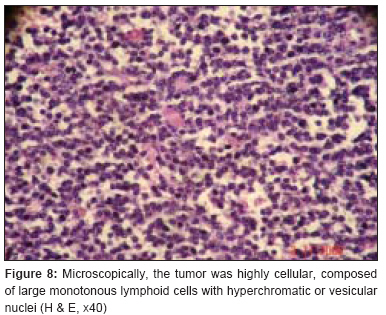
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 203-205 Case Report Lymphoma of frontotemporal region with massive bone destruction and intracranial and intraorbital extension Agrawal Amit, Sinha Arvind Department of Surgery, Datta Meghe Institute of Medical Sciences, Sawangi (Meghe), Wardha Code Number: cr08058 Abstract Primary non-Hodgkin's lymphoma with unilateral proptosis and diffuse involvement of the cra¬nial vault and brain parenchyma is extremely rare. A 50-year-old woman developed a progressively increasing proptosis of her right eye, associated with a subcutaneous mass over the right frontotemporal region over the last 5 months. CT scan showed a high-density contrast-enhancing lesion with wide involvement of the cranium and intracranial and intraorbital extension. We performed a wedge biopsy for further analysis. Histological examination revealed that the tumor was non-Hodgkin's lymphoma. There was no evidence of systemic involvement. The patient received radiotherapy and was doing well at 18 months' follow-up. Primary malignant lymphoma involving the orbit and cranial vault is a rare malignancy, and treatment remains to be defined.Keywords: Calvaria, lymphoma, orbital lymphoma, proptosis Introduction Non-Hodgkin′s lymphoma originating from the cranial vault is extremely rare. [1],[2] On clinical and imaging findings, these lesions with cranial vault involvement, soft-tissue scalp swelling, and underlying intracranial mass can mimic a meningioma. [2] Only one case of primary non-Hodgkin′s lymphoma with unilateral proptosis and diffuse involvement of the cra-nial vault and brain parenchyma has been reported in the literature. [3] We describe a rare case of non-Hodgkin′s lymphoma involving the cranial vault, with intracranial and intraorbital extension. Case Report A 50-year-old woman presented with progressive proptosis of her right eye, associated with a subcutaneous mass over the right frontotemporal region of 5 months′ duration. The mass was firm, nonpulsatile, mildly tender, and attached to the skull; there was overlying healthy skin. Neurological examination revealed no abnormalities. On examination, there was proptosis of the right eye without restriction of extraocular movements [Figure - 1]. Vision in both the eyes was normal. Fundus examination was normal. Plain computerized tomography (CT) scan showed a large high-density mass lesion involving the right frontotemporal region and extending into the right orbit and ipsilateral infratemporal fossa. After contrast administration, the mass was well enhanced and the associated intracranial extension could be seen. The lesion had caused extensive destruction of the underlying skull bones [Figure - 2],[Figure - 3],[Figure - 4],[Figure - 5]. Fine needle aspiration cytology (FNAC) from the lesion showed large monotonous lymphoid cells with hyperchromatic or vesicular nuclei [Figure - 6]. We could perform only a wedge biopsy for further analysis as debulking was not possible due to the highly vascular nature of the lesion [Figure - 7]. Histological examination revealed that the tumor was non-Hodgkin′s lymphoma (diffuse and medium-sized) [Figure - 8]. X-ray chest was normal. Bone marrow biopsy showed hypocellularity but no findings of lymphoma or leukemia infiltrations.There was no evidence of systemic involvement. The patient received radiotherapy and was doing well at 18 months′ follow-up.Discussion Non-Hodgkin′s lymphoma represents only 3-4% of all neoplasms in the general population. It occurs more frequently in patients with acquired immunodeficiency syndrome (AIDS). Di-rect involvement of the central nervous system (CNS) occurs in only 1-2% of patients with lymphoma, and the peak age at onset is during the sixth decade.[4] The incidence of CNS lymphoma has increased in both immunocompromised and immunocompetent persons. [5] Malignant lymphoma originating from the skull may initially extend outside the cranium, extension within the cranium occurring only subsequently. The initial symptoms and signs of lymphoma in the skull include a painless scalp lump, headache due to bone destruction or tumor infiltration of meninges, seizures, and focal neurological deficits resulting from infiltration of the cortex; [1] rarely, there may be unilateral proptosis and diverse features due to diffuse involvement of cranial vault and brain parenchyma. [3] Our present case had unilateral proptosis and diffuse involvement of cranial vault, but because of lack of MRI facilities it was not possible to demonstrate or rule out invasion of the brain parenchyma. Thorough physical examination, complete blood count, CT of the chest and abdomen, and bone marrow biopsy must be performed in these cases to exclude systemic involvement. [6] Our patient did not have any evidence of systemic involvement and the lesion was localized to the cranial region. CT scan of the head will show an extra-intra cranial isodensity lesionof the cranial vault [1] or, alternatively, the lesion may appear as a homogeneous molding mass with sharp margins. [7] MR imaging with contrast administration is superior to CT scan and will give better delineation of these lesions, including brain invasion, thus aiding in the decision making regarding the treatment strategy. [3] The signal intensity on MR images is nonspecific; most reported cases of skull lymphomas report the signal intensity to be isointense on unenhanced MR images and to show marked enhancement on contrast-enhanced images. [3],[4],[5],[7] MR imaging is not definitively diagnostic and the appearance of lymphoma can mimic that of metastatic carcinoma, osteomyelitis, or meningi-oma. [3],[4],[5],[7] Based on other characteristics the lesions can be differentiated, e.g., patients with osteomyelitis have lytic bone lesions and soft-tissue masses, (though systemic signs are usually present by the time soft-tissue masses develop) and meningiomas may have associated hyperostosis. [3],[7] Although the prognostic factors of this rare tumor are unknown, invasion of the CNS indicates a poor prognosis. [3],[5] Primary malignant lymphoma involving the orbit and the cranial vault is a rare malignancy, and treatment remains to be defined. [3],[4],[6] The literature indicates that if there is suspicion of lymphoma, a wedge biopsy must be done. [7] We could not proceed beyond wedge biopsy in the present case as the lesion was highly vascular and we had to abandon the surgical decompression. Individualized microsurgical approaches to the orbit and adequate adjuvant therapy (radiotherapy, steroids, and chemotherapy, administered separately or in combination) are necessary to achieve satisfactory remission of these lesions. [8] The addition of chemotherapy has been reported as not offering any additional benefit, and radiotherapy is considered the treatment of choice in these patients. [9] For the patients with orbital lymphoma an effective dose of radiotherapy of 25 Gy is recommended and it also associated with minimal morbidity even when delivered to the entire orbit. [10],[11] However, recent reports suggest that the addition of combination chemotherapy can improve the outcome in these patients. [6]References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08058f7.jpg] [cr08058f3.jpg] [cr08058f4.jpg] [cr08058f2.jpg] [cr08058f8.jpg] [cr08058f5.jpg] [cr08058f1.jpg] [cr08058f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}