 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
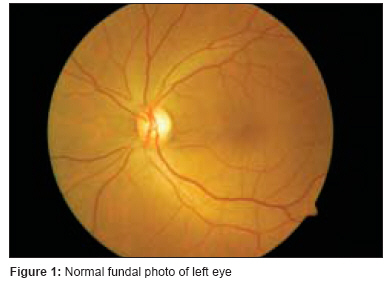
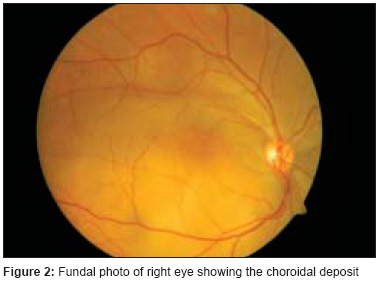
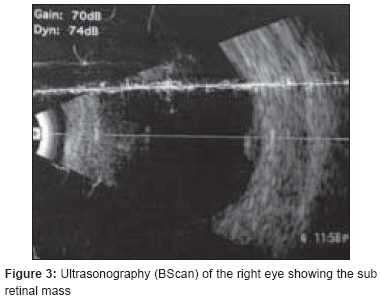
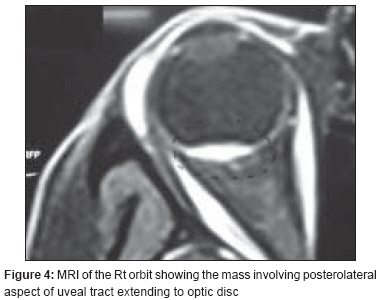
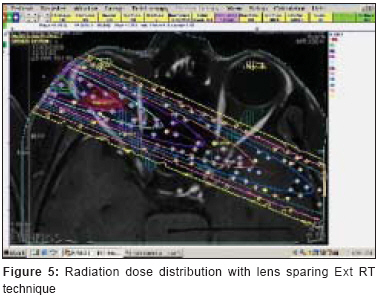
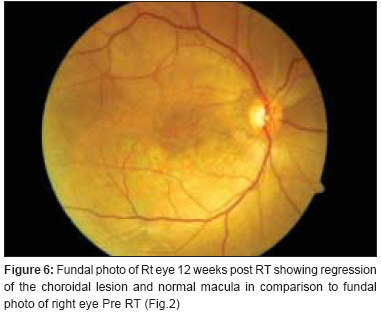
Journal of Cancer Research and Therapeutics, Vol. 4, No. 4, October-December, 2008, pp. 206-208 Case Report Unilateral solitary choroid metastasis from breast cancer: Rewarding results of external radiotherapy Nirmala S, Krishnaswamy Malavika, Janaki MG, Kaushik KirthiS Department of Radiotherapy, MS Ramaiah Medical College, Bangalore - 560 085 Code Number: cr08059 Abstract Intraocular metastatic tumor is the commonest intraocular malignancy in adults, with uveal tract the commonest site. In nearly 85% of cases the choroid is the afflicted site due to its vascularity. Breast and lung are the common primaries. In breast primaries, this could be the first metastatic disease. This condition should always be kept in mind in patients with visual symptoms. Fundus examination, ultrasonography and CT/MRI of the orbit help in diagnosis. Early recognition and timely treatment can save the visual function thus imparting good quality of life to the patient. External beam radiotherapy is a good local form of treatment. Hormone therapy in hormone receptor positive tumors can have additional benefits. Here we report a case of unilateral solitary choroid metastasis in a case of breast cancer treated with external beam radiotherapy. Keywords: Breast cancer, choroid metastasis, ocular malignancy, uveal metastasis Introduction Intraocular metastatic tumor is the most common ocular malignancy in adults. Uveal tract is the most common site of metastasis with the choroid the involved site in 85% of cases, due to its high vascularity. [1] Its frequency in autopsy findings is 12%. [2] The common primaries metastasizing to eye are breast (47%) and lung (21%). [3] Early detection and prompt institution of appropriate treatment saves the vision and improves quality of life. External beam radiotherapy can improve the vision to near normal. Addition of hormone therapy in hormone receptor positive tumors adds to the benefit. Here we report a case of unilateral solitary choroidal metastasis from breast cancer treated with external beam radiotherapy (EBRT) and hormone therapy.Case Report A 60-year-old female patient presented in March 2006 with complaints of diminution of vision in the right eye of 15 days duration. Vision in the left eye was normal. She was a known case of breast cancer (right) diagnosed 3 years previously and underwent modified radical mastectomy followed by adjuvant chemotherapy with 6 cycles of FAC regime and external radiotherapy to the chest wall and drainage areas to a dose of 50Gy/25Fr. Clinical examination showed no signs of loco regional recurrence. On ophthalmologic examination, the left eye was normal [Figure - 1]. Right eye examination findings were as follows: Visual acuity: counting finger -1m. Anterior segment was within normal limits. Fundus: [Figure - 2] Cup/Disc: 0.3/N Blood vessels were normal. Macula showed a dull fundal reflex. Background retina showed a flat amelanotic lesion with no retinal detachment. Ultrasonography of the right eye (B-Scan) showed a subretinal mass [Figure - 3]. MRI of the right eye [Figure - 4] showed a soft tissue mass involving uveal tract of the right globe, posterolaterally extending on to the optic disc. Also shown are MRI of both orbits [Figure - 4]a and MRI of Brain [Figure - 4]b being normal. Other metastatic workups were normal. She received external radiotherapy to the right eye by a single lateral portal with a 15° posterior tilt on a Co-60 teletherapy unit to a dose of 44Gy/22Fr with a palliative intent [Figure - 5]. She was put on anastrazole in view of her hormone receptor positive status. At 12 weeks post therapy ophthalmologic examination of the right eye showed a visual acuity of 6/6. The anterior segment was normal. Background retina showed a flat area, with macular stippling [Figure - 2] and [Figure - 6]. At last follow up i.e., 11 months after radiotherapy, the right eye fundus showed a total disappearance of the lesion with a flat mottled appearance. At the time of sending this paper for publication i.e. 24 months post therapy the patient has normal vision. Discussion The choroid accounts for 85% of uveal metastasis, other sites being ciliary body, iris, rarely retina, optic nerve head and vitreous. [3] The choroid is the most vascular tissue in the eye supplied by about 20 short and long posterior ciliary arteries. Among the primary cancers that metastasize to the eye, breast cancer ranks first (47%), and the next is lung (21%). [3] In a study by Wang et al. , lung primary constituted 50%, breast 22%. The other primaries include GIT 8.3%, kidney 2.8%, liver 2.8%, and unknown 2.8%. [4] The uncommon primaries reported in the literature with choroid metastasis are carcinoid tumor, choriocarcinoma, salivary gland carcinoma, gingival carcinoma, carcinoma of cervix, ovary and endometrium, papillary carcinoma of thyroid and urinary bladder. The common symptoms are decrease in visual acuity, positive scotoma, seeing of black spots, pain, redness of eye due to uveitis and visual loss when complicated by retinal detachment. Some asymptomatic cases are detected during routine fundal examination. In 3% of cases choroid metastasis could be the initial manifestation of the primary disease, and first systemic metastasis in 16% of previously diagnosed breast cancer. [1] The fellow eye should always be examined for asymptomatic lesions. Risk factors for choroidal metastases were dissemination of disease in more than one organ and the presence of lung and brain metastases. [5] Diagnosis is based on opthalmoscopic examination supplemented by imaging studies. The investigations of choice are fluorescein angiography, ultrasonography, CT or MRI of orbit to diagnose primary intraocular spread and extensions. An amelanotic plateau-shaped mass strongly suggests a metastatic tumor. Metastasis from breast is usually multiple and bilateral in 30% of cases. CT scan of the brain helps in diagnosing synchronous brain metastasis seen in nearly 25% of cases. [6] Confirmation is by FNAC in accessible site. Differential diagnoses include amelanotic nevus, amelanotic melanoma, choroidal hemangioma, circumscribed choroidal hemorrhage, posterior scleritis, leukemic deposits, retinitis, choroiditis, and exudative retinal detachment. [7] Treatment options include local forms like external beam radiotherapy, proton beam therapy, plaque brachytherapy (for lesions less than 3 mm in height and away from macula), transpupillary thermotherapy and laser photocoagulation.[8] Systemic chemotherapy, and in tumors over expressing Her2neu, Trastuzumab has shown good results. Local treatment is preferred in cases of choroidal metastasis alone, which can allow conservation of visual function yet minimal morbidity of systemic treatment, but in disseminated disease systemic treatment with or without local therapy is preferred. Median survival after diagnosing symptomatic choroidal metastasis is 4.3 to 7.4 months in the literature. [3],[4] Our patient subsequently developed skeletal metastasis that was treated with radiotherapy and bisphosphonates and presently has normal vision 20 months after the diagnosis of choroidal metastasis. External beam radiotherapy is efficacious in the palliation of posterior uveal metastasis. Rudoler et al. , in a multivariate analysis of 188 patients treated with external radiotherapy concluded that EBRT effectively restores and maintains useful vision with a globe preservation rate of 98%. [8] The complications expected are nearly 12% in the form of cataracts, radiation retinopathy, optic neuropathy, exposure keratopathy, and neovascularization of the iris and rarely narrow-angle glaucoma. [9] Radiation therapy to a dose of 40 Gy in 20 F is an effective and safe palliative treatment for symptomatic and asymptomatic choroidal metastases to preserve vision. [10] Visual complaints should always be taken seriously and probed for choroid involvement in breast cancer cases. External beam radiotherapy is a good local treatment modality to save vision and give good quality of life to patient. Acknowledgment We acknowledge Dr. B. R. Sathyakrishna, Specialist Surgeon, St. Martha′s Hospital, Bangalore, who is the primary surgeon of this case and who first recognized the condition and referred the case timely for treatment. We also acknowledge Dr. Girish Kamath, Consultant Ophthalmologist, Mahavir Eye Hospital, Bangalore, who helped us in acquiring the fundal photographs.References
Copyright 2008 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr08059f1.jpg] [cr08059f5.jpg] [cr08059f2.jpg] [cr08059f3.jpg] [cr08059f6.jpg] [cr08059f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}