 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
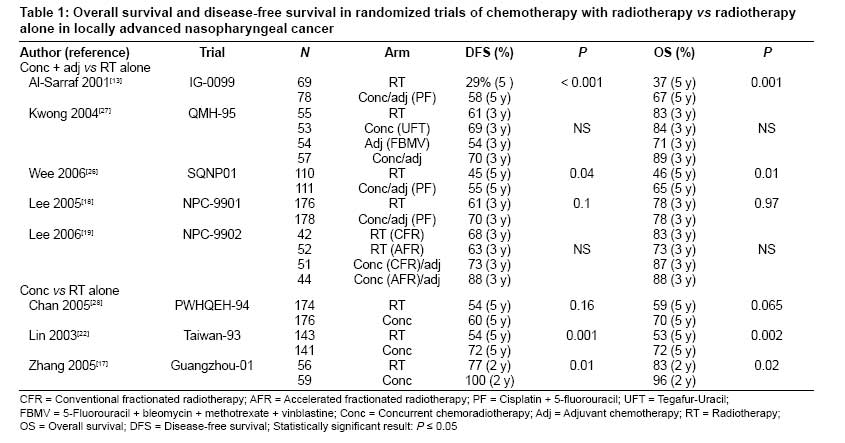
Journal of Cancer Research and Therapeutics, Vol. 5, No. 1, January-March, 2009, pp. 3-7 Review Article Concurrent chemoradiotherapy in the management of advanced nasopharyngeal carcinoma: Current status Afqir, Said; Ismaili, Nabil & Errihani, Hassan Department of Medical Oncology, National Institute of Oncology, Rabat, Morocco. Code Number: cr09002 Abstract Nasopharyngeal carcinoma (NPC) differs from other head and neck cancers in its epidemiology, natural behavior and, particularly, in the therapeutic considerations. In addition, NPC is responsive to both chemotherapy and radiotherapy (RT). This article reviews the recent advances in concurrent chemoradiotherapy (CCRT) for NPC. To identify the studies mentioned in this article, we searched the MEDLINE database, and abstracts of selected conference proceedings (up to 2008) using the key words 'nasopharyngeal carcinoma,' 'advanced,' 'radiotherapy,' and 'concurrent chemotherapy.' Eight randomized clinical trials of CCRT in NPC have been reported in the English literature. These trials can be classified according to the timing of the chemotherapy, which was given either concurrently with RT (in three trials) or concurrently with radiotherapy and adjuvant after the and of concurrent chemoradiotherapy (in five trials). There have also been four meta-analyses addressing the value and scheduling of chemotherapy in the curative treatment of NPC. This article reviews the recent literature and the pertinent issues concerning the role of CCRT in the treatment of patients with locoregionally advanced NPC.Keywords: Advanced, concurrent chemotherapy, nasopharyngeal carcinoma, radiotherapy Introduction Nasopharyngeal carcinoma (NPC) NPC is different from other head and neck cancers; it has a well-defined geographic distribution, a strong relationship with Epstein-Barr virus (EBV) in endemic regions, and remarkable radiosensitivity and chemoresponsiveness. NPC is endemic in Southern China, North Africa, and parts of the Mediterranean basin. [1] Unlike most other squamous cell carcinomas seen in the head and neck, in NPC local recurrence and distant metastases are responsible for treatment failure after therapeutic attempts. [2] The prognosis of patients with NPC depends on the stage of the disease at diagnosis. Unfortunately, at diagnosis, 70% of patients have locally advanced, nonmetastatic stage III or IV disease. [3],[4],[5],[6],[7] Different prognostic groups have been reported by Wei and Sham. [8] Currently, the major challenges in the treatment of advanced stages of NPC center around methods to improve locoregional control and prevent distant metastases. [9],[10],[11],[12],[13] Recent data suggest that chemotherapy (CT) administered concurrently with radiotherapy (RT) improves the effect of RT through volume reduction, increase in radiosensitization, and reduction in the number of micrometastases, thus decreasing the possibility of distant metastases and improving overall survival (OS). However, the optimal regimens of CT and RT are still undecided. [14] In this article we review the findings of studies on the role of concurrent chemoradiotherapy (CCRT) in the management of locoregionally advanced NPC. To identify the relevant studies we searched the MEDLINE database and abstracts from selected conference proceedings (up to 2008) using the key words 'nasopharyngeal carcinoma,' 'advanced,' 'radiotherapy,' and 'concurrent chemotherapy.' How to best incorporate chemotherapy with radiotherapy? Fifteen randomized clinical trials of CT combined with RT have been reported in the English literature for patients with locally advanced NPC. [14],[15] While all 15 trials have used as a same treatment control RT, for the CT treatment the timing of the CT regimen was greatly variable. In four trials, neoadjuvant CT was used prior to the RT; in three trials, CT was given concurrently with RT; in two trials, RT was followed by adjuvant CT; in one trial, neoadjuvant CT was followed by RT, and then by adjuvant CT; and in five trials, concurrent chemoradiotherapy (CCRT) was followed by CT. A recent meta-analysis that evaluated chemotherapy in NPC, which was conducted by the MAC-NPC collaborative group (Meta-Analysis of Chemotherapy in Nasopharyngeal Carcinoma collaborative group), was the only one that used an individual patient data design. [16] This meta-analysis of eight randomized trials (PWH-88, AOCOA, VUMCA 1, Japan-91, IG-0099, PWHQEH-94, QMH-95, and TCOG-94), with a total of 1753 patients, demonstrated a survival improvement with CT. However, CCRT produced statistically significant higher survival. Unfortunately, this meta-analysis only incorporates 8 of the 15 randomized trials; four trials had not completed accrual prior to January 1, 2002 [17],[18],[19],[20] and three trials were excluded. [21],[22],[23] Ten randomized clinical studies, which included a total of 2450 patients, were used in the meta-analysis conducted by Langendijk. [24] In the CT group, absolute survival increased by 4% after 5 years. However, CCRT improved survival by 20% after 5 years. Huncharek and Thephamongkhol [25],[26] reported that the survival benefit was predominantly observed with CCRT using platinum-based agents; the benefit of induction and adjuvant CT remains unclear. Concurrent chemoradiation for locoregionally advanced NPC Data of eight randomized trials published in the English literature demonstrated the superiority of concurrent cisplatin plus RT over RT alone in terms of survival or locoregional control among patients with locoregionally advanced NPC [Table - 1]. Concurrent and adjuvant chemotherapy + RT vs RT alone Five studies have compared CCRT followed by adjuvant CT vs RT alone. [13],[18],[19],[27],[28] The first study was conducted by the Intergroup 0099 (IG 0099) and was reported by Al-Sarraf et al. in 1998 [12] and updated with 5-year results in 2001 [13] by the same authors. In this study, the randomized patients received identical RT (70 Gy) in both arms. In the CT arm, the patients received both concomitant CT (three cycles of cisplatin 100mg/m 2 ) and adjuvant CT (three cycles of cisplatin and 5-FU). At 5 years, the disease-free survival (DFS) was 58% in the chemoradiotherapy arm and 29% in the RT-alone arm, and overall survival (OS) was 67% vs 37%, showing the additional benefit provided by chemotherapy [Table - 1]. In addition, in both locoregional and distant failure were reduced. Despite the significant survival benefit with chemoradiotherapy demonstrated in the intergroup 0099 study, this treatment strategy did not find wide acceptance among the oncologist from the Asian region for the following reasons. The most important reason is the less aggressive form of radiotherapy technique used in the 0099 study that could have lead to inferior result un the RT arm. The second reason is the histological subtypes in the 0099 study: less than half of the patients have the endemic WHO type III undifferentiated carcinoma. [27] Also, compliance with adjuvant chemotherapy was suboptimal, with only 55% of patients completing treatment as planned. Two Asian studies with a design similar to that of the IG-0099 study have been recently published. In the first study, wee et al . attempted to confirm the results of the IG-0099 study and randomized 221 patients with nonmetastatic, stage III/IV NPC to undergo RT, with or without concurrent cisplatin administered over 4 days at a dose of 25mg/m 2 /day every 3 weeks. [27] A significant 19% improvement ( P = 0.01) in the OS rate and 10% improvement ( P = 0.04) in the DFS rate was observed at 5 years, supporting the findings of the IG-0099 study. Compliance with CT in this trial was as unsatisfactory as that in the IG-0099 study, such that 40% of patients required a dose reduction or omission during concurrent cisplatin therapy and 58% did not receive the planned adjuvant CT at the full dose. [27] In the second study (NPC-9901), which was by Lee et al ., [18] patients with nonkeratinizing (WHO IIa) or undifferentiated (WHO IIb) NPC were treated with a CT schedule that was identical to that of the IG-0099 study. At the median follow-up of 28 months, the 3-year DFS rate was 9% more in the chemoradiation arm ( P = 0.1). Longer follow-up is needed before definitive conclusions can be drawn from these Asian studies. In the CCRT arm, 65% of patients completed all six cycles of CT and 79% had ≥ five cycles. The mean number of cycles given during the concurrent phase was 2.5 (±0.6) and 2.6 (±1.3) cycles during the adjuvant phase. [18] Another study conducted by Lee et al . [19] (NPC-9902) used the same CT regimen as IG-0099, but also assessed the therapeutic gain by using concurrent and adjuvant CT and/or accelerated RT. Four arms were evaluated: 1) conventional fractionated RT (CFR); 2) accelerated fractionated RT (AFR) (2-Gy fractions, 6fractions per week); 3) CFR with concurrent and adjuvant CT; and 4) AFR with concurrent and adjuvant CT [Table - 1]. After 189patients had been randomized, the study was stopped due to slow accrual. Preliminary data, after a median follow-up of 33 months, showed no statistically significant difference in 3-year OS and a trend toward improvement in DFS at 3 years. Tumor control may be improved when CT is added to AFR as compared to CFR alone. The proportion of patients who completed all six cycles of chemotherapy was similar in the two arms: 57% in the AFR + CT arm and 55% in the CFR + CTarm. A factorial randomized study (QMH-95) was carried out by Kwong et al ., [28] with four different treatment regimens. The study sought to answer two questions: 1) whether a non-platinum agent, UFT (uracil-tegafur), can achieve results that are comparable to that obtained with concurrent treatment with cisplatin and RT; and 2) whether adjuvant CT (FBMV: 5-FU, bleomycin, methotrexate, and vincristine) is valuable. Although a trend toward improved DFS and OS was noted with the addition of CCRT, statistical significance was not achieved at 3 years. However, a significant reduction in distant metastases was seen for patients receiving CCRT. In this study, adjuvant CT did not improve the outcome of the treatment result, which might be due to the study being underpowered because of a poor accrual rate. Concurrent chemotherapy + RT vs RT alone Three studies have compared CCRT vs RT alone. [17],[22],[29] The most important was conducted in Hong Kong (PWHQEH-94) by Chan et al . [29] The 350 patients with AJCC/UICC stage II to stage IV NPC were randomized to receive either weekly treatment with low-dose cisplatin (40 mg/m²/week without adjuvant CT) and standard RT or RT alone. In a recent update of this study, after a median follow-up of 66 months, a borderline significant 11% improvement in OS (70% in the CCRT group vs 59% in the RT group; P = 0.065) and a trend for improvement in DFS (6% improvement; P = 0.16) was reported favoring the chemoradiation arm for all disease stages. Subgroup analysis demonstrated that patients with T3 and T4 primary disease derived the most benefit from CCRT treatment. In a similar trial conducted by Lin et al ., [22] in Taiwan 284 patients with stage III/IV NPC were randomized to receive either RT alone or RT plus two concurrent cycles of cisplatin and 5-FU administered as a 96-h continuous infusion during week 1 and week 5. However, this trial has been criticized because 14% of the patients were treated with hyperfractionated accelerated RT, whereas the majority of patients received standard RT. Furthermore, there was a slight predominance of patients with stage IV disease in the RT-alone arm (84.6% stage IV vs 75.9% stage III). At a median follow-up of 65 months, an improvement of 19% was noted in the 5-year OS in the chemoradiation arm (72% vs 53%; P = 0.002) and 18% improvement was seen in the DFS rates (72% vs 54%; P = 0.001). The addition of 5-FU to cisplatin during RT did not appear to significantly increase the incidence of grade 3 to grade 4 mucositis (45.4%) or neutropenia (4.3%) compared with the studies by the Intergroup and Chan et al ., [13],[29] in both of which cisplatin alone was used. Guangzhou-01, the smallest of these three trials, randomized 115 patients to receive RT alone or CCRT with weekly oxaliplatin for 6weeks. [17] After a median follow-up of 24months, a statistically significant difference in 2-year OS was reported, favoring the CCRT arm (100% vs 77%; P = 0.01). Both 2-year metastasis-free survival and relapse-free survival were also statistically significantly higher in the CCRT arm (96% vs 83%; P = 0.002). However, longer follow-up is needed before definitive conclusions can be drawn from this study. We conclude that patients with advanced locoregional NPC can be better treated by concurrent chemoradiotherapy than by RT alone. The randomized trials discussed earlier all demonstrate a better treatment outcome with CCRT, but this is at the expense of a higher incidence of acute mucosal and hematologic toxicities. To summarize, concurrent chemoradiation should be adopted as the standard therapy for patients with stage III/IV NPC. [30] Induction chemotherapy followed by concurrent chemoradiotherapy Induction CT led to significant reduction in the incidence of locoregional failures and distant metastases but no improvement in OS was observed; however, reduction in the size of the primary tumor should help to achieve better locoregional control with RT. [31],[32],[33],[34] Recent works have developed the concept of induction therapy by combining it with chemoradiation. Thus, new agents such as paclitaxel, [35] 'ECF' regimen (epirubicin, cisplatin, and infusional 5-FU), [36] interferon, [37] docetaxel, [38],[39] and gemcitabine [40] have all been used and evaluated. EORTC 24971/TAX 323, a phase III randomized trial, [41] evaluated the benefit derived from a docetaxel-based CT regimen (docetaxel, cisplatin, and 5-fluorouracil: TCF) in inoperable, locally advanced head and neck cancer (NPC patients were excluded). Patients treated with the TCF regimen had a significantly longer median OS and time to disease progression compared to a standard treatment with cisplatin and 5-fluorouracil. On the basis of these results, the authors believe that docetaxel could improve the tumor response, specifically the complete response (CR), following the induction period of the treatment of NPC prior to RT, leading ultimately to an improved outcome in terms of survival. This drove the authors to begin another trial, EFC 10339, which is currently underway. [42] It is about 2:1 ratio randomized study which seeks to evaluate the effect of docetaxel given in combination with CF (TCF) on CR, as compared to the standard combination of CF (the control treatment). We conclude that the use of induction chemotherapy is encouraged by the interesting results of studies conducted by Chan et al. [35] and Rischin et al . [36] However, further investigations are necessary to recommend this way to use in practice. [36] Molecular-targeted therapy and immunotherapy Several molecular targets have been identified in NPC. [15] Expression or over-expression of epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEGF), c-KIT, and c-erbB-2 (HER2) has been seen in NPC. [15] Furthermore, phase II studies of cetuximab, gefitinib, and sorafenib, [43],[44],[45] suggested that targeted therapy is effective in achieving satisfactory response in patients with metastatic or recurrent NPC. A recent study suggested that EBV DNA quantification has the potential to act as a marker for monitoring and predicting treatment outcomes in patients with advanced NPC. [46] The association of EBV and NPC has raised hopes for the possibility of immunotherapy. NPC cells express two distinct EBV latent membrane proteins: LMP-1 and LMP-2. These proteins may become targets for adoptive immunotherapy. A phase I study using EBV-specific cytotoxic T lymphocytes (CTL) reported promising results, [47] and further studies utilizing CTL appear indicated. Conclusion
Acknowledgment We sincerely thanks Mohammed Ismaili, Professor of Microbiology at Moulay Ismail University, Meknes, Morocco.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09002t1.jpg] |
| |||||||||

{kind=link}